
Abstract
Crimean-Congo hemorrhagic fever (CCHF) is viral hemorrhagic fever caused by CCHF virus, which belongs to the family Bunyaviridae and the genus Nairovirus. The virus is transmitted to humans via contact with blood and tissue from infected livestock, a tick bite, or contact with an infected person. Since 2000, we have shown the disease to be prevalent in 23 out of 30 provinces of Iran. Among those, Sistan-va-Baluchistan, Isfahan, Fars, Tehran, Khorasan, and Khuzestan demonstrated the highest infection, respectively. Notably, Sistan-va-Baluchistan province, southeast of Iran, has the highest prevalence of CCHF, and has shown to be present since at least 2000. Phylogenetic study of the CCHF virus genome isolated from Iranian patients showed a close relationship with the CCHF Matin strain (Pakistan). Our epidemiological data in the last decade have implied that the severity and fatality rate of the disease has ranged variably in different provinces of Iran. More pathogenesis and phylogenetic studies should therefore be investigated to clarify these differences.
Introduction
Since CCHF was first discovered in the Crimea and Belgian Congo, the disease has been reported in many regions of Africa, the Middle East, Europe, and Asia (Hoogstraal 1979, Swanepoel et al. 1987, Nichol 2001, Whitehouse 2004, Seimenis 2006). The history of CCHF in Iran refers to sporadic surveys between 1970 and 1978; however, between 1978 and 1999 there were no evidence of CCHF investigations (Asefi 1974, Saidi et al. 1975, Sureau et al. 1980, Ardoin and Karimi 1982, Chinikar et al. 2008). A CCHF surveillance and control program in Iran in 1999 was established by three collaborating organizations; the Center for Disease Control in the Ministry of Health, Pasteur Institute of Iran, and the Veterinary Organization, which are all categorized on the national level. Moreover, three organizations were constituted to form a National Expert Committee on Viral Hemorrhagic Fevers (NECVHFs), dedicated to the control, awareness, diagnosis, and treatment of VHFs. According to the NECVHF's schedule, the Arboviruses and Viral Hemorrhagic Fevers Laboratory (National Reference Laboratory) performs on time and free-of-charge serological (specific ELISA with recombinant antigen) and molecular (gel-based and real-time RT-polymerase chain reaction) assays (Chinikar et al. 2004, Ergonul 2006, Garcia et al. 2006, Chinikar et al. 2008). The Center for Disease Control supervises the sending of CCHF probable cases' sera to the National Reference Laboratory, and the immediate and free-of-charge treatment of patients. The Veterinary Organization collects suspected livestock sera and ticks from high-risk regions, sends samples to the National Reference Laboratory, and plays an important role in prevention and control of tick populations (Chinikar et al. 2008). Our classified epidemiological data on CCHF patients further address an advance in the geographical distribution of CCHF infection, and the efficient role of the CCHF surveillance program in controlling mortality rate and prevalence of CCHF disease in Iran since 2000 is also explained.
Results
As illustrated in Figure 1, from June 7, 2000, to December 31, 2009, serum samples of 1638 CCHF probable cases were collected from different provinces of Iran. Among these CCHF probable cases, 635 were confirmed cases, and among them 89 died. Similarly, in the same period, among 4846 livestock sera, which were collected from high-risk regions, 2014 were positive for anti-CCHFV IgG. Since 2000, it has been demonstrated that the disease has infected 23 out of 30 provinces of Iran. Sistan-va-Baluchistan (with 283 confirmed cases), Isfahan (with 44 confirmed cases), Fars (with 26 confirmed cases), Tehran (with 17 confirmed cases), Khorasan (with 12 confirmed cases), and Khuzestan (with 10 confirmed cases) had the highest prevalence of CCHF infections, respectively. Notably, Sistan-va-Baluchistan province (southeast of Iran) has not only had the highest number of cases, but also CCHF infection has been observed since 2000.
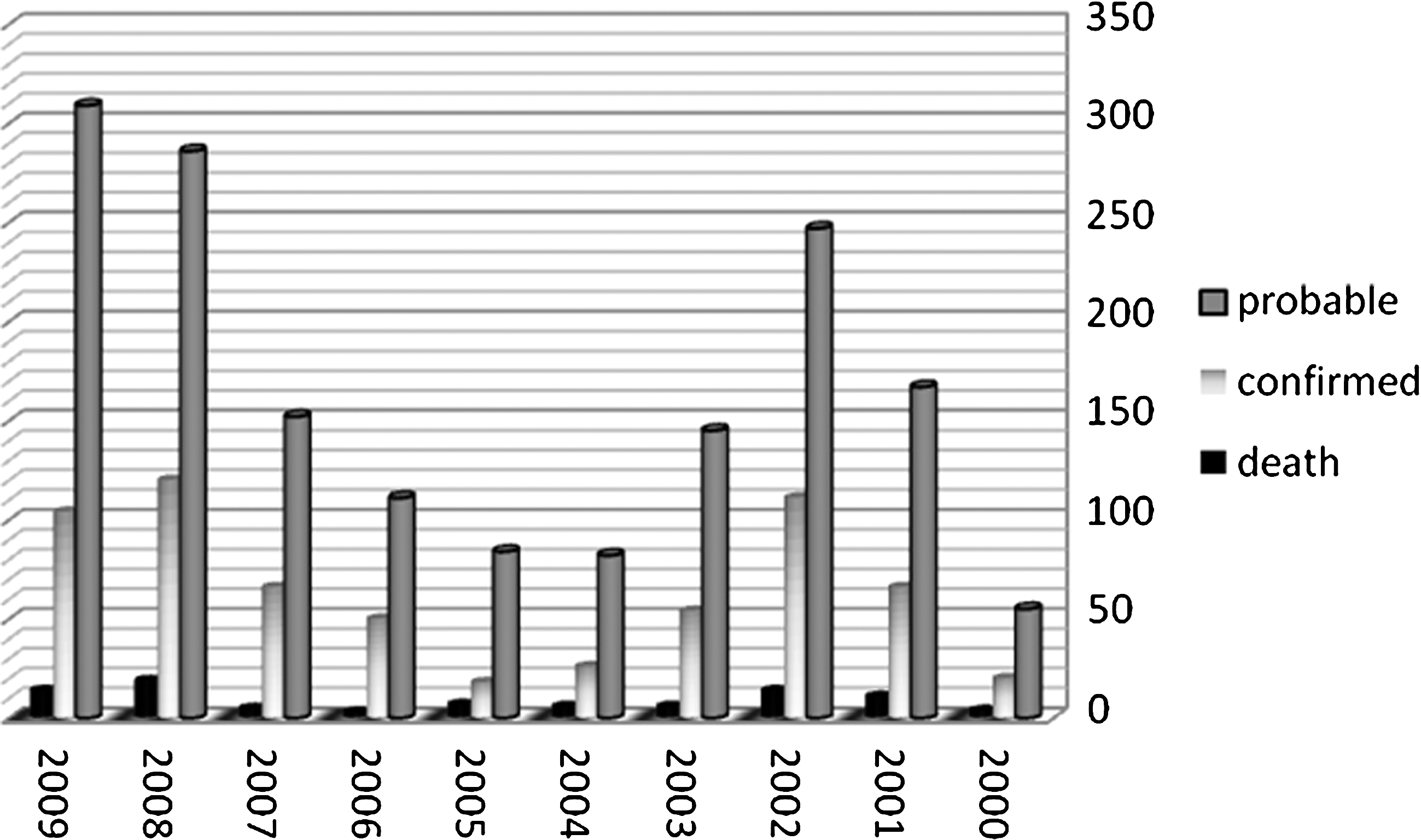
Number of human probable, confirmed, and death cases of Crimean-Congo hemorrhagic fever (CCHF) between 2000 and 2009.
The distribution of CCHF in terms of sex and age among the Iranian CCHF-confirmed cases showed that 77.5% were male and 22.5% were female. About 52.2% of the CCHF-confirmed cases were in the 21–40-year age range. As seen in Figure 2, the most affected professions included jobs that involved the handling of blood and organs from infected livestock (e.g., farmers, butchers, and slaughterers). Other CCHF patients often were those who resided in proximity to livestock and occasionally slaughtered the livestock, for example, housewives and workers or students living in rural areas (Fig. 2).
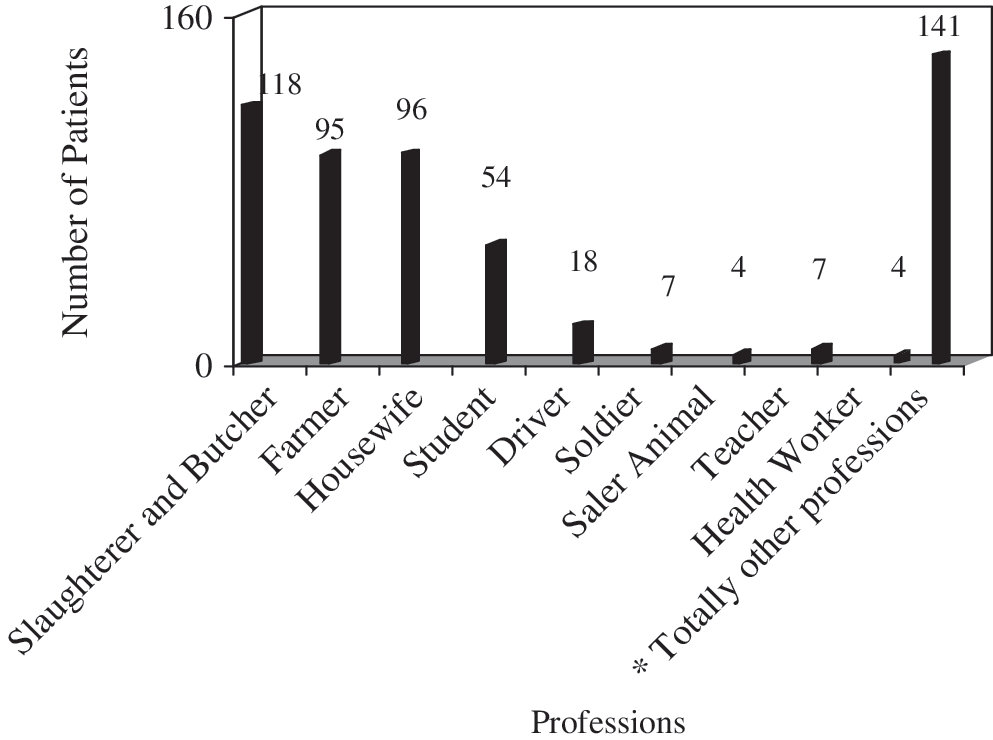
Proportion of CCHF cases in Iranian professions from 2000 to 25 May 2009 (*Other Professions include Mason, Carpenter, Cook, Baker, Worker, and Barber).
Our data showed that the presence of CCHF is gradually raised in March and reaches a peak in June and July during the study years in Iran (Fig. 3).
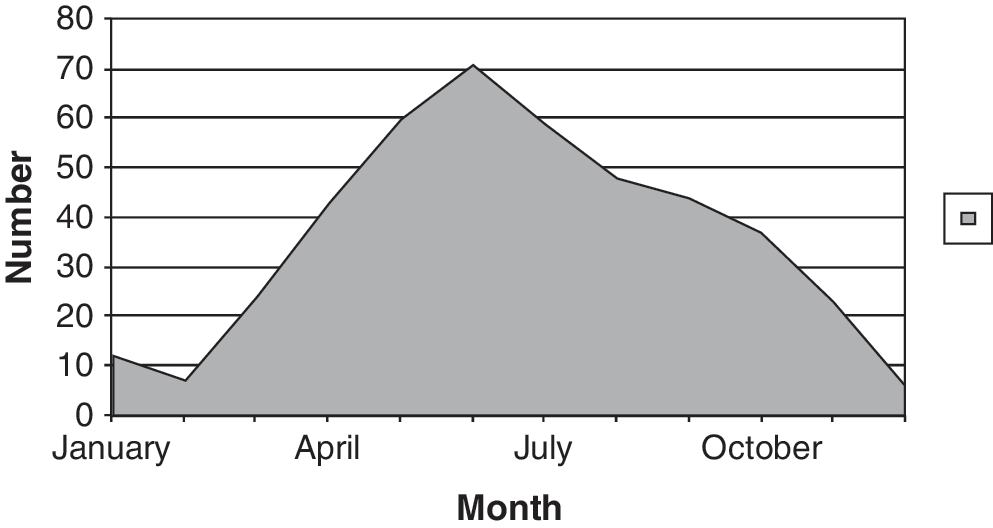
Distribution of CCHF throughout the year.
For genetic analysis, single polymerase chain reaction bands, corresponding to the expected 536-bp product of the S-segment from analyzed Iranian patients' sera, were sequenced. Comparative analysis of the obtained sequences showed a close relationship. In addition, phylogenetic analysis using S-segment sequences demonstrated that the Iranian isolates formed a distinct lineage together with the Pakistani strain Matin (Chinikar et al. 2004).
Discussion
By considering CCHF infection in 23 out of 30 provinces, Sistan-va-Baluchistan has been shown to be the most infected province since 2000, as it is neighbored with a wide border to two CCHF endemic countries, Pakistan and Afghanistan. More prevention and control programs need to be monitored in this province as well as in the other endemic regions. As seen, the highest proportion of CCHF infection is among high-risk professions such as butchers and slaughterers, and the most common route of CCHF transmission in Iran is via contact with blood and secretions of infected livestock. However, nosocomial transmission has played an important role in the recently controlled outbreaks in the country. Owing to their involvement in high-risk professions, males comprised a high percentage of CCHF infection, and the proportion of the infection was also higher in the working age range of 21–40 years. As our epidemiological data have shown, the severity and mortality rate of CCHF infection in different provinces of Iran are variable. Also, apart from Sistan-va-Baluchistan province, CCHF infection has been seen in different provinces in different years. Therefore, further pathogenesis and phylogenetic studies and better surveillance system facilities should be considered to clarify these differences.
The occurrence of human CCHFV infections in Iran has been recognized; however, the circulation of CCHFV in ticks and livestock plays an important role in infection maintenance and this requires further investigation. Therefore, detection and sequencing of the S-segment of CCHFV genome from ticks, and drawing the relevant phylogenetic relationships are the main objectives for our laboratory in order for the national surveillance system of CCHF to survey origin and situation of geographical distribution of the CCHFV in the country. It is very likely that the livestock trade has played a significant role in distribution of the virus in the endemic regions of the country; thus, to achieve the main goal, a massive program of molecular epidemiology of CCHFV in ticks from over the country is being performed.
In the laboratory detection part of the national surveillance program of CCHF, one of the essential components of serological diagnosis is antigen. It is worth mentioning that the production of the CCHF native antigen requires biosafety containment level 4 that does not exist in Iran. Fortunately, in the National Reference Laboratory, we designed and expressed a new recombinant CCHF antigen in mammalian cells by Semliki Forest virus vectors (in a common project with Pasteur Institute of Paris) whose production does not require biosafety level 4 containment. Therefore, this rendered a great help to the CCHF diagnosis system in Iran (Garcia et al. 2006). In addition to specific abilities in the surveillance program of CCHF, the NECVHFs members had also common capabilities in the control program, with a strong, regular, and intersectorial collaboration with the relevant organizations inside the country.
In conclusion, the identification of the geographical distribution of CCHF and the decrease in the mortality rate of CCHF in Iran in recent years has been in accordance with all of the surveillance strategies of CCHF.
Footnotes
Acknowledgments
The authors really appreciate Prof. Dr. Tony Fooks for reading the article and editing its English language. Part of this work has been facilitated through the International Network for Capacity Building for the Control of Emerging Viral Vector Borne Zoonotic Diseases (Arbo-Zoonet) supported by the European Union under grant agreement no. 211757.
Disclosure Statement
No competing financial interests exist.