
Abstract
Purpose:
Limited data exist on differences of erythema migrans patients with either positive or negative Borrelia burgdorferi sensu lato skin culture.
Methods:
We analyzed 252 adult patients with erythema migrans in whom skin biopsy specimen was cultured for the presence of B. burgdorferi sensu lato. Evaluations of epidemiological, clinical, and microbiological findings were conducted at baseline, 14 days, 2, 6, and 12 months after treatment with either doxycycline or cefuroxime axetil.
Results:
One hundred fifty-one (59.9%) patients had positive skin culture (86.9% B. afzelii, 8.0% B. garinii, 5.1% B. burgdorferi sensu stricto) and 101 (40.1%) had negative skin culture. Patients in the culture-positive and culture-negative groups were comparable for the basic demographic, epidemiological, clinical, and laboratory characteristics at presentation. Statistically significantly worse selected treatment outcome parameters in the culture-positive group compared with the culture-negative group were established during follow-up. Treatment failure was documented in two patients who were culture positive and in none in the culture-negative group.
Conclusions:
Although findings for the pretreatment characteristics were comparable between the erythema migrans skin culture-positive and culture-negative patients, some parameters indicate that borrelia skin culture positivity may predict a less-favorable treatment outcome.
Introduction
To further evaluate the pretreatment characteristics and to investigate possible differences in the posttreatment course between the patients with culture-positive and culture-negative erythema migrans, we compared demographic, epidemiological, clinical, and laboratory findings according to the presence or absence of B. burgdorferi sensu lato as detected by skin culture before antibiotic treatment. We hypothesized that the patients with positive skin culture results have a higher borrelial burden in the skin than the culture-negative patients, which might influence the course and posttreatment outcome of the disease.
Patients and Methods
Selection of patients
All patients evaluated from June through September 2006 at the Lyme Borreliosis Outpatient's Clinic, University Medical Center Ljubljana, Slovenia, were eligible for participation in the study if they were at least 15 years of age and had typical solitary erythema migrans. Typical erythema migrans was defined according to the criteria proposed by the CDC (1997). In addition, patients with skin lesion less than 5 cm in diameter were also included if they recalled a recent tick bite at the site of later skin lesion, had a symptom-free interval between the bite and the onset of the lesion, and reported an expanding skin lesion prior to diagnosis. Patients were excluded if they did not consent with the skin biopsy; had a medical history of Lyme borreliosis; were pregnant, lactating, or immunocompromised; have had a serious adverse reaction to a beta-lactam or tetracycline drug; received an antibiotic with known antiborrelial activity within 10 days; and had multiple erythema migrans lesions or an extracutaneous manifestation of Lyme borreliosis. The study was approved by the Medical Ethics Committee of the Ministry of Health of the Republic of Slovenia.
Antibiotic therapy
The patients were assigned to receive a 15-day oral treatment with either doxycycline 100 mg or cefuroxime axetil 500 mg twice daily. The treatment option changed on a weekly basis.
Clinical evaluation
At each visit a detailed medical history was obtained and physical examination was performed. Patients were asked about the presence of subjective symptoms. After responding to this open question, patients were asked specifically about the presence of eight particular symptoms (fatigue, arthralgias, myalgias, headache, paresthesias, dizziness, irritability, or nausea). Symptoms that newly developed or worsened since the onset of the erythema migrans and had no other known medical explanation were regarded as new or increased symptoms (NOIS). The severity of any individual symptom was graded by the patient on an 8-cm visual analog scale (8 = most severe) (Wormser et al. 1999). The number of symptoms and the symptom severity score (the sum of symptom severities) were calculated.
Laboratory evaluation and microbiological analysis
Complete blood cell count and basic serum chemistries were performed at baseline and after 14 days. At baseline as well as 2, 6, and 12 months thereafter, serum IgM antibodies to outer surface protein C (OspC) and variable surface antigen (VlsE), and IgG antibodies to VlsE B. burgdorferi sensu lato antigens (Diasorin) were determined. Seropositivity to borrelia was defined as positive borrelial IgM or IgG.
At baseline, prior to antibiotic treatment, skin specimen obtained from the expanding edge of erythema migrans (2.5 × 2 × 2 mm) was put in the tube with 10 mL of modified Kelly-Pettenkofer culture medium (Preac-Mursic et al. 1986). Skin biopsy was repeated 2–3 months later in all patients with B. burgdorferi sensu lato cultivated from the first skin biopsy specimen.
Cultures were examined weekly for the presence of spirochetes by dark-field microscopy (Ruzić-Sabljić et al. 2000) and were interpreted as negative if no growth was established up till 9 weeks. Strains were characterized to species level by PFGE after MluI restriction of genomic DNA as reported elsewhere (Ruzić-Sabljić et al. 2002).
Assessment of outcome
At day 14, patients were asked about medication compliance and adverse events. A complete response was defined as resolution of erythema migrans with return to pre-Lyme borreliosis health status. Incomplete response was defined as either incomplete resolution of erythema migrans or the presence of NOIS (partial response), or occurrence of new objective signs of Lyme borreliosis (failure).
Complete response at 2, 6, and 12 months postenrollment was defined as continued absence of objective manifestations of Lyme borreliosis, with return to pre-Lyme borreliosis health status. Incomplete response was defined as either the presence of NOIS without an objective manifestation (partial response), or occurrence of objective manifestations of Lyme borreliosis or persistence of B. burgdorferi sensu lato in skin at the site of the previous erythema migrans (failure).
As failure is a rare event (Cerar et al. 2010), we did not attempt to analyze this outcome separately, but rather grouped partial responses and failures in the incomplete response category. The number of failures per group is reported and the clinical history of the patients with failure is described.
Statistical analysis
Data were summarized as frequencies (%) for categorical data and as medians (interquartile range [IQR]) for numerical data.
The characteristics at enrollment and laboratory findings of the patients with positive and negative skin cultures were compared using Mann–Whitney test for numerical variables, and Yates' corrected chi-squared test or Fisher's exact test for categorical variables. To control for multiple comparisons, a significance level of 0.01 was used (p < 0.01).
To evaluate if complete response was associated with skin culture positivity, we used a logistic regression model with complete response as the dependent variable and skin culture positivity as a covariate; to take into account the multiple measurements repeated in each patient, the analyses were adjusted for a subject variable as a random effect and for follow-up time (used as a categorical variable).
We considered three additional outcomes: the number of NOIS, the symptom severity score, and seropositivity to borrelia; to evaluate the association of number or severity of NOIS with culture positivity, we used Poisson regression models, adjusting the analysis for repeated measurements and time, as described for the logistic model. Seropositivity to borrelia was analyzed as described for the analysis of complete response.
Effect estimates and their 95% confidence intervals (CI) were obtained from the resulting regression coefficients and their standard errors; the association of the covariates with the outcome was assessed by Wald test and a significance level of 0.05 was used (p < 0.05).
All reported p-values are two sided. Statistical analyses were performed using Epi info version 3.4.3 software (CDC) and R statistical language (R Development Core Team 2009). The random effect regression models were fitted using the lme4 R package.
Results
Epidemiological and clinical findings at presentation
A total of 252 patients with solitary erythema migrans were enrolled in the analysis: in 151 (59.9%) patients B. burgdorferi sensu lato was isolated from the skin biopsy specimens and 101 (40.1%) patients had a negative skin culture. Regarding the basic characteristics at presentation, patients in the culture-positive group and the culture-negative patients were comparable (Table 1).
Data are median (IQR), or number (%).
To control for multiple comparisons, a significance level of 0.01 was used (p < 0.01).
Underlying chronic illnesses such as arterial hypertension, hyperlipidemia, osteoporosis, diabetes mellitus, thyroid disease, cardiac rhythm abnormality, psychiatric illness, ischemic heart disease, osteoarthritis, or asthma.
Patients with a history of a tick bite at the site of the erythema migrans skin lesion.
Patients with erythema migrans who reported NOIS. Some patients had more than one NOIS.
Mean number of NOIS in the patients who had NOIS.
Mean symptom severity score of NOIS among the patients who had NOIS, based on an 8-cm visual analog scale, with a score of 8 being the most severe.
IgM and/or IgG to Borrelia burgdorferi sensu lato positive. Serological testing was done for 148 culture-positive patients and for 98 culture-negative patients.
EM, erythema migrans; IQR, interquartile range; NOIS, new or increased symptom.
Laboratory findings
Nonspecific laboratory values were only occasionally abnormal. The changes were usually mild and the proportions of patients with abnormal laboratory tests' results were similar in both groups (Table 2).
White blood cell count, normal: 4–10 × 109 L−1.
Blood platelet count, normal: 140–340 × 109 L−1.
Serum concentration of bilirubin, normal: ≤17 μmol/L.
Serum concentration of aspartate aminotransferase, normal: ≤0.58 μkat/L.
Serum concentration of alanine aminotransferase, normal: ≤0.74 μkat/L.
WBC, white blood cell count; Plt, platelets, AST, aspartate aminotransferase; ALT, alanine aminotransferase; μkat, expressing activity of AST, ALT.
Treatment outcome
All patients stated that they were compliant with taking the study drug. Doxycycline and cefuroxime axetil were comparable regarding treatment efficacy and drug-related adverse events. No adverse event resulted in discontinuation of treatment.
The median duration of the erythema migrans skin lesions after starting antibiotic treatment did not differ significantly between the culture-positive and culture-negative groups (5 [IQR 4–7] and 7 [IQR 4–8)] days, respectively; p = 0.46). The duration was longer than 14 days in only 16 patients (6.3%, eight per group).
The clinical outcomes for patients in the two groups at follow-up visits are summarized in Table 3. Complete response was observed more frequently among the patients with negative culture than among those who had a positive culture at each follow-up time point. In both patient groups there was a steady decrease in the proportion of patients with incomplete response (Fig. 1). The large majority of patients (84.3% and 94.5% for the culture-positive and culture-negative patients, respectively) had complete response from 2 months onward. Five of 129 (3.9%) culture-positive patients evaluated at 12 months posttreatment reported NOIS, but none of 75 patients in the culture-negative group. The logistic regression model for repeated measurements (Table 4, first and second columns) indicated that the risk of not reaching a complete response was significantly higher among those patients who had a positive culture (odds ratio [OR] of complete response associated with culture positivity was equal to 0.39, 95% CI: 0.17–0.88, p = 0.024). Moreover, the probability of reaching a complete response significantly increased with time from enrollment, most markedly between the first and second follow-up time points (OR for complete response at follow-up time of 2 months versus 14 days was equal to 4.36, 95% CI: 2.35–8.07, p < 0.001). Further, we observed significant differences in the mean number (p = 0.045; Table 4, columns 3 and 4) and severity of NOIS (p = 0.045; Table 4, columns 5 and 6) between the two patient groups: the culture-positive patients had more NOIS than the culture-negative patients, and their symptom severity score was higher.
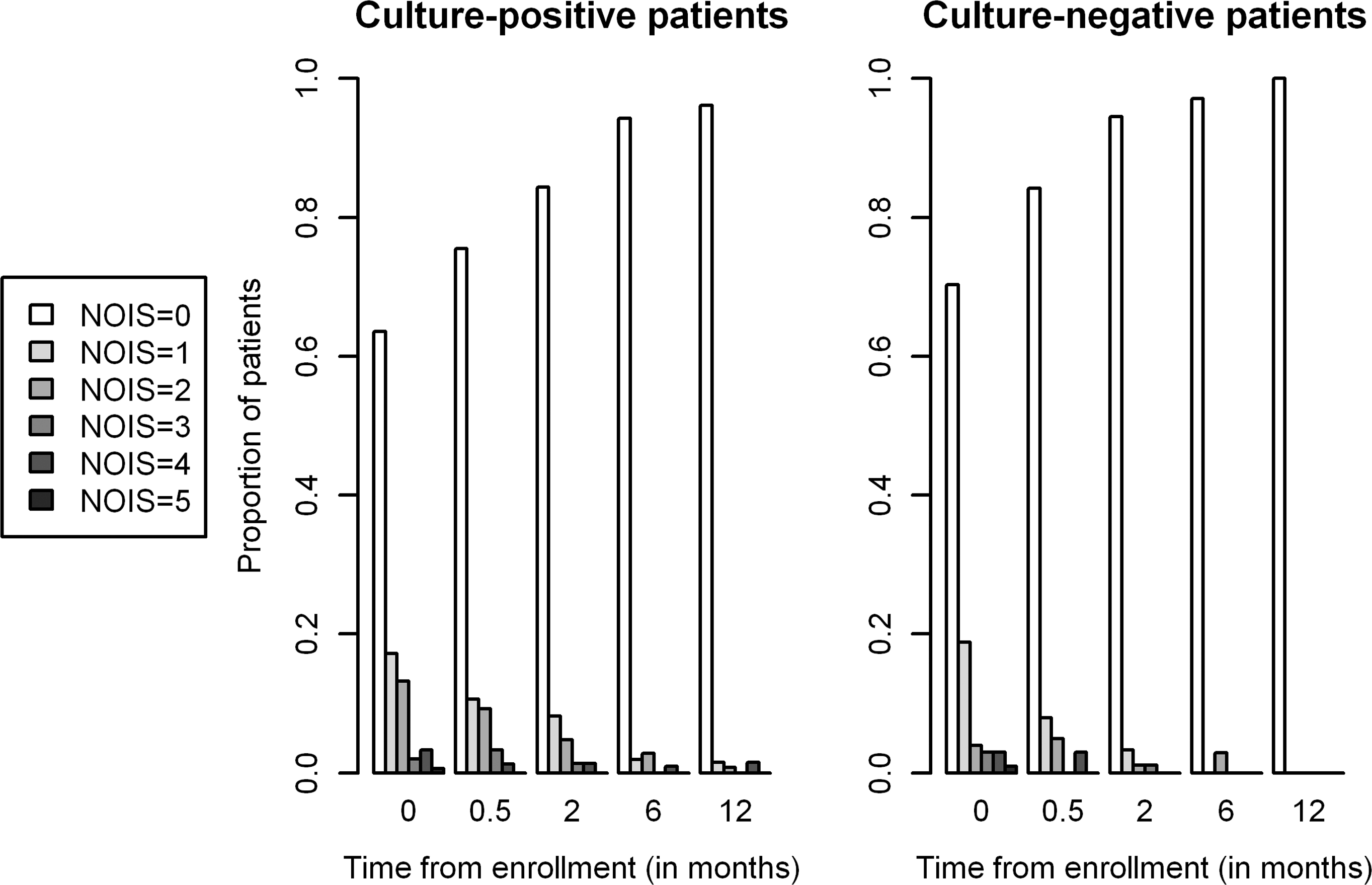
Distribution of number of new or increased symptoms (NOIS) over time, stratified by patient group.
Data are frequency of evaluable patients (%).
Median time of last evaluable visit was 12 (IQR 12–12) months after enrollment in the culture-positive group versus 12 (IQR 6–12) months after enrollment in the culture-negative group (p = 0.02).
See Patients and Methods section for details.
Coefficient estimated from the multivariable regression models, adjusted for patient effect. The estimates for complete response are derived from a logistic model, whereas those for number of NOIS and symptom severity score are derived from Poisson regression models.
p-Values are derived from two-sided Wald test.
CI, confidence intervals; eb, odds ratio.
It is possible that the patients who reported NOIS were less likely to participate in the follow-up, but all patients were reexamined at 14 days. Only 8 of 252 (3%) patients were (completely) lost to follow-up after the second visit, 18 (7%) were reexamined only once, 81 (32%) twice, and 145 (58%) three times. The methods of analysis that we used (regression models for repeated measurements) do not require that all the subjects are observed at each follow-up, and therefore, also patients with incomplete follow-up were considered in the analysis.
Failure was documented in only two patients, both were treated with doxycycline and both were in the culture-positive group. One of these patients developed multiple erythema migrans by the 14th day visit and was retreated successfully with ceftriaxone. The second patient had a positive skin culture for B. afzelii before treatment as well as 2 months afterward. This patient had resolved the erythema migrans skin lesion and was asymptomatic after treatment with doxycycline. The strain of B. afzelii that grew, however, was different from the original isolate based on a comparison of the plasmid profiles of the two strains. This culture-positive patient was then treated with cefuroxime axetil. A repeat skin culture at 4 months was negative, and further clinical course was uneventful.
Microbiological findings
Borrelia antibody titers were positive in 167 of 246 (67.9%) tested serum samples at enrollment. During follow-up, there were no significant differences in the proportion of seropositive patients between the two groups, whereas the proportion of seropositive patients significantly decreased from the 2nd to the 6th month from enrollment (Table 3). Of 137 identified borrelial species, 119 (86.9%) were B. afzelii (Mla 1), 11 (8.0%) B. garinii (Mlg 2), and 7 (5.1%) B. burgdorferi sensu stricto (six Mlb 2, one Mlb 8). During follow-up, there were no significant differences in the proportion of seropositive patients between the two groups (OR of seropositivity associated with culture positivity was equal to 0.82, 95% CI: 0.25–2.62, p = 0.73; Table 5), whereas the proportion of seropositive patients significantly decreased between the 2- and 6-month follow-ups (OR = 0.14, 95% CI: 0.07–0.30, p < 0.001).
See Patients and Methods section for details.
Coefficient estimated from multivariable logistic regression models, adjusted for patient effect.
p-Values are derived from two-sided Wald test.
Discussion
Most investigators agree that objective manifestations of late Lyme borreliosis in the patients who had been previously treated for erythema migrans represent treatment failure (Steere et al. 1983b, Weber 1996). On the other hand, the association between adequately treated erythema migrans and subjective symptoms such as arthralgias, headache, and fatigue is less clear. Although there are several possible explanations for the persistence of residual symptoms—including continued infection, an immunologic process, permanent tissue damage resulting from the initial infection (Sigal 1994), and coinfection with another tick-borne pathogen—the cause of posttreatment symptoms remains insufficiently understood (Dattwyler et al. 1997). Realistic evidence that active infection accounts for this adverse outcome is lacking (Klempner 2002). For those patients with persistence of functionally disabling subjective symptoms for at least a 6-month period after completion of appropriate antibiotic therapy for Lyme borreliosis, Infectious Diseases Society of America (IDSA) experts proposed a term post-Lyme disease syndrome (Wormser et al. 2006). Nowakowski and colleagues, in their long-term follow-up study of patients with culture-confirmed erythema migrans, lend some support to the contention that at least some residual symptoms are related to the original B. burgdorferi infection. They base this assumption on their observation that symptoms during follow-up were associated with multiple erythema migrans lesions and more symptoms of greater severity at the time of initial diagnosis (Nowakowski et al. 2003). Accordingly, several other therapeutic trials from the United States and Europe have independently shown that in patients who reported posttreatment symptoms, greater frequency of multiple erythema migrans or accompanying symptoms such as fatigue, headache, stiff neck, arthralgias, myalgias, malaise, paresthesias, or irritability were present before treatment (Steere et al. 1983b, Weber and Neubert 1986, Dattwyler et al. 1990, Weber and Neubert 1986, Massarotti et al. 1992, Luger et al. 1995). However, in few other studies the severity of the initial illness did not have an impact on treatment outcome (Weber et al. 1993, Luft et al. 1996). Seropositivity to borrelia, either at presentation or follow-up, was uniformly found not to be a risk factor for treatment failure (Dattwyler et al. 1990, Massarotti et al. 1992, Weber et al. 1993, Luft et al. 1996, Nowakowski et al. 2003, Wormser et al. 2003). Thus, there are indications that the presence of erythema migrans-associated pretreatment symptoms (which have been interpreted as an indicator for disseminated borrelial infection) (Wormser et al. 2005) might suggest higher chances for unfavorable treatment outcome. However, treatment failure in patients with erythema migrans could also be associated with several other factors, including the amount of borrelia (borrelia burden). Erythema migrans skin culture result has not yet been evaluated as a potential influential factor for treatment outcome. According to Liveris et al., the number of spirochetes present in infected patients with erythema migrans might be a contributing factor to the variability of disease manifestations (Liveris et al. 2002). They evaluated clinical and laboratory findings for patients with erythema migrans with respect to the number of B. burgdorferi organisms detected by quantitative PCR in 2-mm skin biopsy specimens and found wide ranges of detected mean number of spirochetes. Larger numbers of spirochetes were significantly associated with a shorter duration of the erythema migrans skin lesion prior to diagnosis, smaller skin lesions, and infection with a specific genotype of B. burgdorferi but not with the number or severity of symptoms. In addition, skin culture positivity was significantly associated with skin lesions containing larger numbers of spirochetes. We assumed that the latter was also valid for our culture results.
In our study, we did not find significant association between borrelia skin culture results and selected pretreatment characteristics of patients with erythema migrans. Lower proportion of patients with complete response in the culture-positive group compared with the culture-negative group indicates less-favorable treatment outcome in the culture-positive patients. Moreover, patients in the culture-positive group had a statistically significantly higher number and severity of NOIS. Complete response, number of NOIS, and their severity are not independent outcomes; therefore, we expected that the findings related to these outcomes would be similar.
Further, of 252 patients there were only two treatment failures evidenced by objective findings, and they both occurred among culture-positive patients. We interpreted the case with a positive rebiopsy skin culture as a treatment failure based on the assumption that the original infection was mixed; however, other explanations are possible, such as reinfection or that the posttreatment culture became contaminated in the laboratory. Hypothesis of reinfection seems less plausible because the patient did not report additional tick bites during the 12-month follow-up. As patients knew their skin culture results, we could not exclude the possibility that this might have influenced/biased our results, which is a drawback of our study. However, the steady decline in proportion of symptomatic patients in the culture-positive as well as in the culture-negative group contradicts this assumption (Fig. 1). Although negative skin culture results do not exclude the presence of borrelia, our results suggest that borrelia skin culture positivity, which could, according to Liveris et al. (2002), reflect higher borrelia burden, may potentially influence the posttreatment outcome in the patients with erythema migrans. If valid, our assumptions can only refer to European Lyme borreliosis, which, as shown also in our study, is predominantly caused by B. afzelli. Although statistically significant, the established differences between the culture-positive and culture-negative groups were small and might not be of great clinical relevance. Additional studies are needed to further substantiate our findings.
In conclusion, although the findings for the pretreatment characteristics were comparable for the culture-positive and culture-negative patients, some parameters indicate that borrelia culture skin positivity may suggest a less-favorable treatment outcome in the patients with erythema migrans.