
Abstract
Introduction:
In May 2007, five patients with Q fever-like symptoms were reported in an agricultural educational center in the rural southern French town of Florac. An investigation was undertaken to identify the outbreak source and risk factors for infection, and to implement control measures.
Materials and methods:
We undertook active case finding. Patients were defined as individuals with an unexplained fever of ≥38.5°C who lived in, worked in, or visited Florac between April 1 and June 30, 2007. Patients were confirmed by a positive Q fever serology test. A cross-sectional survey with a seroprevalence component was carried out in the educational center and surrounding area. A standardized questionnaire on known risk factors for the infection was used and serological testing was carried out on finger prick blood specimens from participants. The veterinary services investigated local herds within a 5-mile radius using polymerase chain reaction and serological tests.
Results:
One hundred twenty-two people were included in the cross-sectional survey. Eighteen serologically confirmed acute cases were identified, of whom 12 were from the educational center. The statistical analysis showed an independent association between acute infection and living or working near an area where manure had been spread (p = 0.0.042) and male gender (p = 0.022). Frequenting the educational center's canteen was also associated with infection (p = 0.008) among staff and students. The veterinary investigations identified 11 of the 26 tested flocks of goats and sheep as seropositive for Coxiella burnetii, including 2 ovine flocks located northwest of Florac that had high shedding levels of the bacterium.
Discussion:
The observed excess of cases of Q fever in Florac, an area endemic for this infection, in spring 2007 could be explained by an aerial transmission from infectious ovine flocks situated close to the town. All local herd owners were re-educated about the risks and prevention practices for Q fever.
Introduction
Human infection with C. burnetii can cause acute Q fever after an incubation period of ∼2 to 3 weeks (Heymann 2004). Acute Q fever generally presents as a self-limited febrile illness, sometimes associated with pneumonia and/or hepatitis. Sixty percent of patients remain asymptomatic (Tissot-Dupont et al. 1992, Raoult et al. 2000). Pregnant women, immunosuppressed individuals, and people with valvular heart disease are particularly at risk for the chronic form of Q fever infection, which can manifest as endocarditis, valvular infection, osteoarticular infection, or repeated abortion (Maurin and Raoult 1999, Raoult et al. 2000).
The disease is endemic in several rural areas in France that practice animal husbandry, particularly in the south of the country. Q fever infection is not notifiable in France. The National Reference Centre (NRC) has estimated an annual incidence in the south of the country of 50 patients per 100,000 inhabitants (Tissot-Dupont et al. 1992, Maurin and Raoult 1999).
On May 10, 2007, local health authorities and the French National Public Health Surveillance Institute were informed of five patients with high, persistent, and unexplained fever. The patients were staff members of an agricultural training center located in southeast Florac, a town of 2000 inhabitants in rural southern France. We describe the investigations conducted to identify patients, determine risk factors for acute human infection, and identify the outbreak source and the control measures implemented.
Materials and Methods
Case definition
Possible cases of acute Q fever infection were defined as individuals with an unexplained fever of ≥38.5°C who lived or worked in or had visited the town of Florac or been within a 5 km radius around Florac, between March 1 and June 30, 2007, in the absence of a blood test.
Confirmed acute cases were individuals with or without symptoms who lived in, worked in, or had visited the town of Florac or been within a 5 km radius around Florac, between March 1 and June 30, 2007, with an IgM anti-phase II titer ≥50 and IgG anti-phase II titer ≥200 assessed by indirect immunofluorescence at the NRC.
Active case finding
Between May 11 and June 30, we carried out active case finding by daily and then weekly contact with all general practitioners serving Florac and the surrounding areas, doctors of local hospitals, and medical laboratories. In addition, we interviewed all students and employees who frequented the training center between April 1st and the time of the survey.
Cross sectional seroprevalence study
During May 2007, we carried out a cross-sectional seroprevalence study among adults (≥18 years) in Florac. We interviewed all employees of the training center and all students enrolled in long-term training courses that were present during the survey. We also interviewed all available inhabitants and workers of a predefined study zone in the center's immediate neighborhood, using a door-to-door approach. A structured standardized questionnaire was used. Data collected included demographical, biological, and clinical data and data on potential risk factors for acquiring acute Q fever between March 1, 2007, and the date of interview. Because of the high frequency of asymptomatic infections, case status was defined by serological test results. We collected finger prick blood specimens on blotting paper from each participant. The confirmed acute case definition from the active case finding was also used here. In addition, previous Q fever infection was defined as the absence of an IgM titer and an IgG anti-phase II ≥25; chronic Q fever was defined as an IgG anti-phase I ≥1600.
Statistical analysis
Risk factor analyses were carried out including only confirmed acute infections, identified by both active case finding and the cross sectional study, and uninfected individuals according to serological test results. Individuals with previous or chronic infection were excluded.
Data were analyzed using SAS® v8.1. Prevalence ratios and their 95% confidence intervals were calculated for risk factors in the cross-sectional seroprevalence study. Differences between proportions were assessed using the chi-square or Fisher's exact test with p-values <5% defined as statistically significant. Two multivariable logistic regression models assessing risk factors independently associated with acute Q fever infection were built: one for the entire study population and one restricted to individuals working/studying at the training center. Exposures showing an association of p ≤ 0.10 in univariate analysis were included in the multivariable analysis. A backward stepwise variable selection strategy was used to construct a final model with a significance level of p < 0.05. Models were adjusted for age and sex. The Hosmer and Lemeshow test was used to assess the goodness of fit of the final model (Hosmer and Lemeshow 1989).
Veterinary investigation
The veterinary services identified and investigated all goat, sheep, and cattle herds within a 5 km radius from Florac. Q fever serological testing for was carried out on all herds between June 5 and 16, 2007, using the Ruminant serum Q-fever ELISA kit® (Laboratoire Service International, Lissieu, France). Thirty animals per flock were sampled or all animals if the flock size was <30 animals. The presence of C. burnetii shedding among seropositive herds was determined by real-time polymerase chain reaction (PCR) (TaqVet Cox; LSI, Lissieu, France) testing of vaginal swabs and milk samples. Vaginal swabs were taken from all females in flocks having <10 animals or on a maximum of 10 females having lambed or aborted in the previous months. Shedding levels were defined as low (<60% of animals with weakly positive PCR results), medium (60%–100% of animals with weakly positive or positive PCR results), and high (>90% of animals with strongly positive PCR results). PCR results were considered as weakly positive, positive, and strongly positive when 1–100, 100–1000, and >1000 bacteria per sample were found, respectively. Data on herds were collected including proximity to the training center, location and movements of herds since March 1, 2007, history of abortions and births, disposal of placentas and birth products, and manure spreading practices.
Meteorological data
Daily minimum and maximum temperatures and precipitation data were obtained from the Meteo France weather station at Florac from February to May 2005–2007. Monthly compass cards measuring wind strength and direction for the same period were obtained from the Meteo France wind-measuring station closest to Florac.
Results
Case finding/seroprevalence study
During the seroprevalence study, 158 people were interviewed: 90 in the center and 68 in its immediate neighborhood. Blood samples were obtained from 138 (87%) people.
We identified 18 confirmed and 4 possible cases of acute Q fever via active case finding and the seroprevalence study. Three possible cases were not confirmed by serology testing and one was not tested. Only confirmed cases are described hereafter. Twelve cases (67%) were among staff or students of the training center, 3 lived or worked in the zone of Florac included in the seroprevalence study and 3 lived in or had visited other sectors of Florac. Twelve patients (67%) reported symptoms. All symptomatic patients reported fever, 11 (92%) reported extreme fatigue and 8 (67%) reported headache. Raised liver enzymes were found in all 8 symptomatic patients that were tested. Symptomatic patients reported symptom onset between 12 March and 14 May 2007 (Fig. 1). The median age of patients was 41 years (extremes: 26–70). The male:female sex ratio was 2. Four patients (22%) were hospitalized for periods of 2 to 8 days; all recovered.
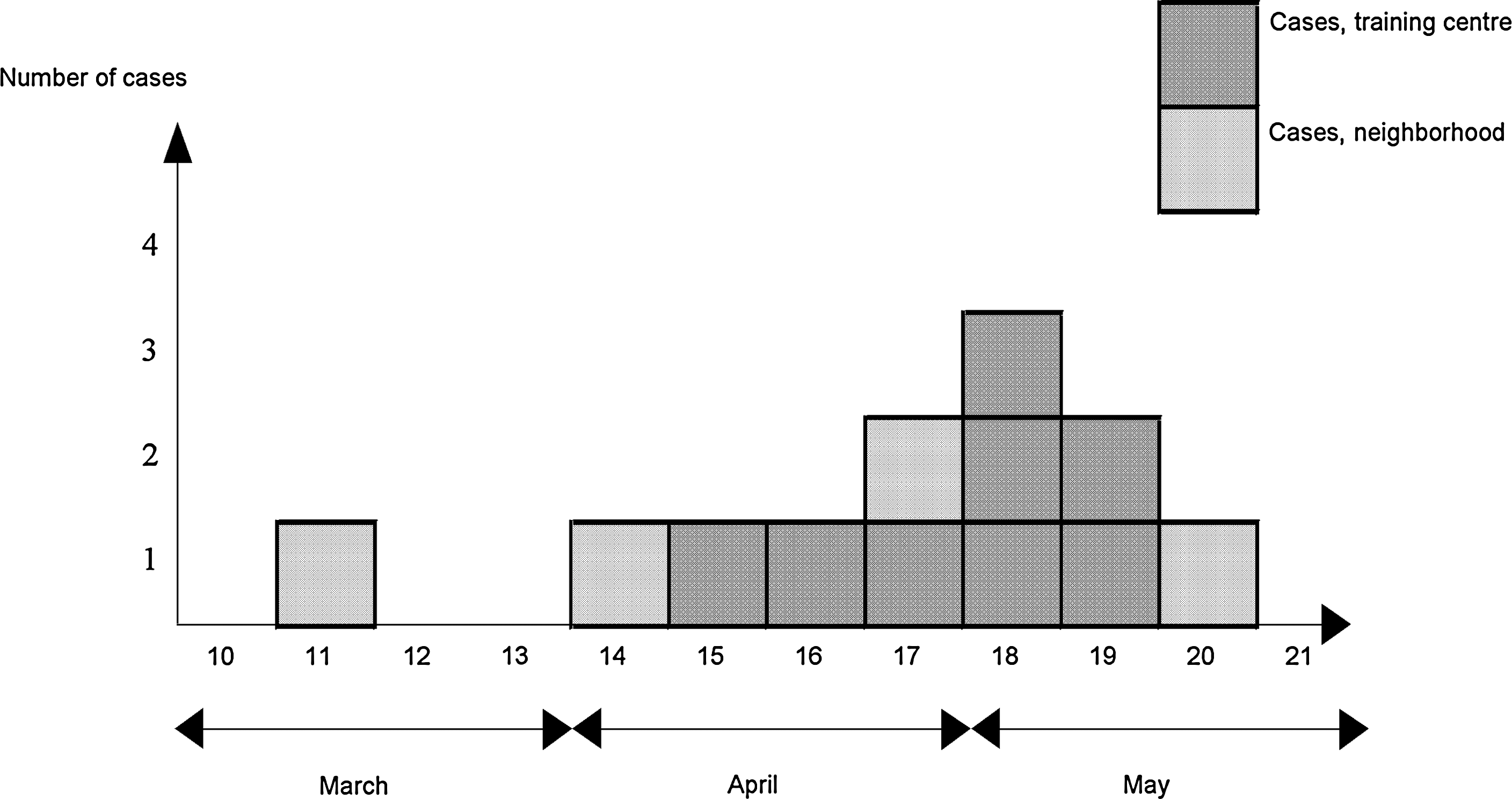
Date of symptom onset by week for the confirmed acute symptomatic Q fever patients, Florac, spring 2007 (n = 12).
The seroprevalence study additionally identified 14 people (10%) with evidence of a previous Q fever infection and 2 people (1%) with chronic infection.
Risk factor analysis
The statistical analysis of risk factors for acute infection included 122 people, after exclusion of 20 individuals without a serological test result and 16 people with a previous or a chronic infection. Sixty-eight (56%) people worked in the center. Fifteen confirmed cases were included in the analysis (12 in the center and 3 in the community).
The whole study population analysis showed that people who worked in the training center or who lived or worked near a spreading of manure were 3.8 times more likely to have acute Q fever infection than those who did not (Table 1). People who reported undertaking outdoor sports were 2.8 times more likely to have acute infection than those who did not, but this association was not significant (Table 1). In the multivariable regression analysis, male sex and living or working near a manure spreading area were independently associated with acute infection (Table 2).
() missing values.
95% CI, 95% confidence intervals; PR, prevalence ratio.
OR, odds ratio.
In the analysis restricted to staff and students of the training center, individuals who reported attending the canteen for eating, working, or social activities were 5.9 times more likely to have acute infection than those who did not (Table 1). In the multivariable analysis, male sex, living or working near a manure spreading area, and frequenting the canteen were independently associated with acute infection (Table 2).
Veterinary investigation
In total, 26 herds of ruminants, representing 3627 animals, were located within a 5 km radius from Florac: 19 flocks of sheep, 6 flocks of goats, and 1 flock of cattle.
Samples from 447 animals of all 26 herds were tested for C. burnetii by serological tests. Eleven herds (44%) were positive. Six had a C. burnetii antibody seroprevalence >50%. Vaginal specimens were analyzed from 102 animals from the 11 seropositive herds. Nine (82%) herds were PCR positive, including 3 flocks of sheep and 1 flock of goats with low shedding levels, 2 flocks of sheep and 1 flock of goats with medium shedding levels, and 2 sheep flocks with high shedding levels (Fig. 2).

Geographic location of 25 ruminant flocks, including 2 high-level Coxiella burnetii–shedding flocks, identified within a 5 km radius around Florac, spring 2007.
Milk specimens were analyzed from 40 animals from 8 of the 9 seropositive herds with no excretion or with low or medium excretion levels of C. burnetii. Milk specimens were not available for one herd with no bacterial excretion. Ten samples (25%) from 4 herds were positive.
About 970 births were enumerated in the 26 herds during spring 2007. Births in the two herds with high C. burnetii shedding (herds A and B) represented >30% of all births. Abortions had occurred in herd A (10 abortions since March in a flock of 500) and in a herd with no seropositive animals (1 abortion in June). None of the breeders of the 5 flocks with medium or high excretion level undertook manure spreading between March and June 2007. Fourteen breeders reported contact with the training center, including the farmers of the sheep flocks A and B; 2 breeders worked in the center, and the others visited the center between March and June 2007.
Weather conditions
The weather in April 2007 was hotter but not dryer than in April 2006 and 2005. The weekly maximum temperatures were ∼4 degrees higher than in April 2006 and 2005. A 16-day period with a maximum temperature higher than 20 degrees was observed in April 2007, which is unusual in this region. The prevailing wind direction in April 2007 was from northwest to southeast.
Control measures
During the outbreak, individuals at high risk of developing chronic infection were advised to consult their doctor, even if asymptomatic, for a diagnostic test. Blood donations from Florac and the surrounding area were interrupted during the outbreak to avoid potential contaminations by infected blood and blood products. Samples already collected in May 2007 were not distributed and were retrospectively tested for C. burnetii to assess the extent of the outbreak.
Recommendations for good practice, in particular for manure spreading and dealing with animal birth and abortion products, were discussed with all local farmers and implemented during 2007. The vaccination of all animals in the 11 seropositive herds was recommended. It was also recommended to notify abortions among herds to their usual veterinarian, who in turn directs them to local-level state veterinary services, and to bury biological materials, such as placentas and birth products. Farmers were advised to carry out the removal of carcasses by quartering, to stock manure far from human dwellings, to spread it in fields not exposed to the most frequent winds, and to plough it in immediately after spreading. During the outbreak, dairy production from herds around Florac was pasteurized before distribution in accordance with recommendations of the French Agency for Food Safety (AFSSA 2004).
Discussion
Our investigation confirms the occurrence of a small outbreak of 18 cases of Q fever among residents and workers of Florac in rural southern France during the spring 2007. The first outbreak cases were identified in the agricultural training center in Florac. Three additional patients who had no identifiable links to the center were identified by active case finding. These elements led us to undertake a cross-sectional seroprevalence study in the training center and in the immediately surrounding population to examine the hypothesis of a community source of contamination.
The cross-sectional seroprevalence study revealed a statistical association between acute Q fever infection and living or working near a manure spreading field. This association was found in the analysis of the whole study population and the sub-analysis for the training center. The veterinary investigations showed C. burnetii contamination of 11 of the 26 herds of ruminants within 5 km around Florac, including 9 herds that were shedding the bacterium at the time of testing. Two sheep flocks with high levels of C. burnetii shedding were located northwest of the town.
Combining the location of these two heavily shedding flocks, the geographic location of the town in a valley of north–south orientation, and the prevailing wind direction in the Florac area of northwest–southeast in April 2007, we suggest that airborne transmission of C. burnetii originating from these two flocks was the most likely source of the outbreak. Wind has been reported to play a role in the transmission of C. burnetii in previous outbreaks (Carrieri et al. 2002, Tissot-Dupont et al. 2004).
The association between acute infection and working in the training center could be explained by the fact that individuals working at the training center were more likely to be exposed to the heavily excreting flocks A and B due to the nature of their work. The centre offers post-secondary level training in subjects such as ecology, agriculture, biodiversity, and communication skills. Many students and staff were regularly exposed to the surrounding countryside. The administered questionnaire did not permit quantification of the duration of work-time spent outdoors or visiting farms in and around Florac, information that could have further supported such a hypothesis. No particular risk factors for Q fever were identified at the training center. It is also likely that additional asymptomatic cases outside of the training center and the study zone in Florac were not identified.
Attending the training center's canteen for eating, working, or social activities were independently associated with acute Q fever infection. The seroprevalence study did not identify a link between any particular dairy food item and the occurrence of acute infection. A large proportion of cases and noncases had consumed a particular type of raw milk goat's cheese. This cheese is a specialty of this region and so a high consummation rate is not unexpected. The epidemiological investigation showed that patients consumed raw-milk goat's cheese from multiple different sources and so a link between consumption of this food item and acute infection is unlikely. There is currently no consensus in the literature on the role of unpasteurized dairy products in the transmission of C. burnetii.
The canteen is located on the ground floor of the training center and has a south-facing picture window, which facilitates easy access to the center's garden. In good weather, the picture window is open, as was the case for several weeks during March 2007. The association between attending the canteen and illness could be explained by the entry of C. burnetii–contaminated dust into the canteen via the window.
The association between acute infection and male sex could be explained by occupational factors and associated longer outdoor expositions for men. A predominance of male patients has previously been described in similar outbreak situations (Armengaud et al. 1997, InVS 2003, Rey et al. 2005).
This study has several limitations. Information about the location of C. burnetii–excreting animal herds in relation to Florac and the training center was not available during the investigation. It was thus not possible to define precise places or itineraries at risk for the interviews. The intermittent shedding of C. burnetii by infected animals means that the shedding status of herds may vary depending on the day of sampling. Thus, the shedding status attributed to herds from our study samples may not represent the herd's status at the time of infection of human cases.
The cross-sectional seroprevalence study and the veterinary investigations have shown that Florac is an area endemic for Q fever. These results were confirmed by a serological survey that was carried out by the NRC and the French National Association for Blood on blood donations collected before the identification of this outbreak. Serum samples from 51 donors having donated blood in May 2007 in Florac were tested for antibodies to C. burnetii. Three donors (6%), all asymptomatic, had an acute Q fever infection, and 4 (8%) had had a previous infection (Daurat et al. 2009).
In conclusion, this investigation shows the occurrence of a small outbreak of Q fever in an area endemic for this infection in rural southern France. This outbreak highlights the need for continued efforts to control the spread of C. burnetii and for surveillance of Q fever infection.
Footnotes
Acknowledgments
The authors wish to acknowledge the following individuals for their assistance with the outbreak investigation: A. Mailles and V. Vaillant of the French Institute for Public Health Surveillance, P. Malfait and J. Berbis of the Regional Epidemiology Unit South of France, C. Colardelle et D. Meffray of the Direction départementale de la Protection des Populations in Lozère, and the staff and students of the Agricultural Training Center and the inhabitants of the town of Florac for their cooperation and assistance provided.
Disclosure Statement
No competing financial interests exist.