
Abstract
A representative, two-stage probability sampling design was used to select 40 villages in northern Azerbaijan with populations of <500 people to screen for evidence of prior infection with Francisella tularensis. Informed consent was provided, and samples were obtained from 796 volunteers and tested for the presence of immunoglobulin G antibodies using enzyme-linked immunosorbent assay. F. tularensis seropositivity was prevalent (15.5% of volunteers), but there was minimal reporting of signs and symptoms consistent with clinical tularemia, suggesting that mild or asymptomatic infection commonly occurs. Frequently seeing rodents around the home was a risk factor for seropositivity (POR = 1.6, p = 0.03), controlling for age and gender. Geospatial analysis identified associations between village-level tularemia prevalence and suitable tick habitats, annual rainfall, precipitation in the driest quarter, and altitude. This study contributes to the growing understanding of the geographic distribution of tularemia and provides further information on the climatic and landscape conditions that increased the potential for exposure to this pathogen. The potential occurrence of asymptomatic or mild F. tularensis infection warrants further study.
Introduction
Tularemia, the clinical manifestations of infection with the bacterium Francisella tularensis, has multiple forms, including ulceroglandular, oculoglandular, and oropharyngeal syndromes, along with pneumonic and typhoidal (systemic) presentations (Ellis et al. 2002). F. tularensis subspecies tularensis, also known as type A (or biovar A), occurs mainly in North America and is the most virulent subspecies in both animals and humans. F. tularensis subspecies holarctica, classified as type B (or biovar B), is the predominant biovar in Europe and Asia and tends to cause less-severe clinical disease.
Tularemia can be transmitted by direct contact with infected animals or their tissues, ingesting undercooked infected meat or contaminated water, animal bites or scratches, arthropod bites, and inhalation of aerosol or contaminated dust (Jellison 1974). The clinical manifestations are largely determined by the portal of entry for the organism. Contaminated water was likely responsible for outbreaks of oropharyngeal tularemia in Bulgaria (Christova et al. 2004) and Turkey (Helvaci et al. 2000, Akalin et al. 2009) and recently in Georgia (Chitadze et al. 2009). Evidence of aerosol transmission was provided by outbreaks in Sweden in the winter of 1966–1967 (676 cases) (Dahlstrand et al. 1971) and Martha's Vineyard USA (15 cases) (Feldman et al. 2001). Tularemia can be transmitted by a variety of insect vectors; Aedes Culex and Anopheles species mosquitoes and Ixodes and Dermacentor species ticks are thought to propagate the enzootic cycle as well as transmit the bacterium to humans (Hubalek et al. 1996, Ellis et al. 2002, Goethert et al. 2004). In the former Soviet Union, various aquatic rodent species are thought to serve as the primary reservoir, particularly Arvicola amphybius (Mörner 1992).
The environmental factors relevant to tularemia epidemiology are poorly understood, partially because of the myriad of possible transmission routes of this pathogen. Additionally, most countries have limited human and vector surveillance information available for tularemia. Geographic information system (GIS) technology has been recently utilized to investigate the ecoepidemiology of tularemia (Eisen et al. 2008, Svensson et al. 2009, Goethert and Telford 2009), but further studies are needed to understand the complex transmission dynamics of this pathogen.
We conducted a representative population-based study of rural villages, aiming to define the tularemia antibody prevalence in three regions of Azerbaijan. The demographic, epidemiologic, and climatic factors associated with tularemia prevalence were explored.
Materials and Methods
Study subjects
A two-stage, probability proportional to size sampling design (Macro International, Inc. 1996) was used to select 40 villages in northern Azerbaijan with populations of <500 people. Village registries served as the sampling frame for the selection of households; 20 households were selected in each village. After providing informed consent, adult volunteers responded to a questionnaire recording demographics, health care utilization, and history of clinical syndromes. A broad range of potential risk factors were evaluated, including exposure to rodents, insect vectors, water sources and treatment practices, and outdoor activities. The fieldwork was conducted from June to October 2008. The clinical protocol was reviewed and approved by ethics committees in the United States and Azerbaijan.
Tularemia enzyme-linked immunosorbent assay
The tularemia enzyme-linked immunosorbent assay utilized for this investigation was developed at the United States Army Medical Research Institute of Infectious Diseases (Waag et al. 1995), and the methods are described elsewhere (Chitadze et al. 2009). Sera reacting at a cutoff of ≥4 standard deviations above the average of the negative control titers were considered positive.
Originally, the assay was developed and tested on the recipients of the live, attenuated tularemia vaccine, which demonstrated a humoral response to vaccination that was statistically significant compared with controls (Waag et al. 1995). The assay was employed in a tularemia outbreak in Georgia, in which high titers were exhibited in infected patients (Chitadze et al. 2009). The enzyme-linked immunosorbent assay results were comparable to a microagglutination test and Western blotting, which were also utilized to test the serum from the outbreak.
Data analysis
Demographic, clinical, and epidemiologic parameters were assessed using prevalence odds ratios (POR), chi-squared test, and the Fisher's exact test. Associations with p < 0.10 were included in the regression analysis and removed by backward elimination (Epi Info™, version 3.4). Potential interaction terms were evaluated through stratified bivariate analysis. Odds ratios that varied significantly by stratum were further evaluated as interaction terms in the multivariate regression model.
Geospatial analysis
The effect of climatic conditions, including temperature and precipitation, and landscape parameters, including altitude and land cover, were assessed. The geographic information utilized includes (1) country and regional-level administrative boundaries (GADM database); (2) village geographic coordinates (Geographic Names Database); (3) climate parameters including temperature (mean, minimum, and maximum annual temperature; mean temperature of the warmest quarter; mean temperature of the coldest quarter; maximum temperature of the warmest month; minimum temperature of the coldest month; annual temperature range) and precipitation (annual precipitation; precipitation in the driest quarter; precipitation in the wettest quarter). Climate data were obtained from WorldClim Global Climate Database, 1 km spatial resolution; (4) land cover data (GLC2000 Database, 1 km spatial resolution) were evaluated directly and subsequently reclassified by the suitability for tick vectors. Suitable habitats included tree cover (evergreen, deciduous, and mixed) and shrub cover (evergreen, deciduous, and mixed); partially suitable habitats included cultivated areas, and seasonally flooded areas, water, sparse/barren areas, and urban areas were considered unsuitable; (5) altitude (CGIAR SRTM30 Database, 1 km spatial resolution).
Climate, land cover, and altitude parameters significantly associated with village-level tularemia prevalence using bivariate linear regression and not significantly correlated to each other (Spearman rank correlation <0.8) were evaluated by forward stepwise multivariate linear regression. Circular neighborhoods were assigned to each village with a radius of 0.08 to account for the geographic spread of the village and smooth the artifacts encountered with high-resolution environmental data. Geospatial analyses were conducted using the geographical information system DIVA-GIS.
Results
Study population
Respondents included 796 adults from 40 villages in the Guba, Gusar, and Xachmaz regions of Azerbaijan. The average age of the study population was 36.2, and women comprised 56.4% of respondents. The age and gender composition of the volunteers as well as the highest level of education attained was comparable to national rural averages for Azerbaijan (Table 1).
National rural age distribution estimates are based on percentages of the rural adult population [adapted from State Statistical Committee (Azerbaijan) and Macro International, Inc. (2008)].
Age was significantly associated with tularemia seropositivity.
Gender and educational attainment statistics are based on national estimates of the rural population [State Statistical Committee (Azerbaijan) and Macro International, Inc. (2008)].
Ethnicity estimates are based on national census statistics for rural Azerbaijan (State Statistical Committee of the Republic of Azerbaijan 2003).
Population estimates for each region are given in terms of the number of residents in villages with <500 population and percentage of the total population for the region (unpublished data).
Tularemia prevalence
We found a tularemia antibody prevalence of 15.5% (95% confidence interval: 13.1%–18.3%). Seropositive volunteers were significantly older (average age of 48.4) than seronegative volunteers (41.5 years; p < 0.0001). The highest prevalence was found in the 50–64-year-old age group (Table 1). Tularemia seropositivity was slightly more prevalent among women (16.8%), those with a high-school education (18.9%), and residents of the Xachmaz region (17.2%), but the results were not statistically significant. No other demographic characteristics were associated with seropositivity. Few subjects reported a history of lymphadenopathy in this population (8), only 1 of which was serologically positive for tularemia. No clinical symptoms were associated with tularemia seropositivity.
Frequently seeing rodents around the home was a risk factor for seropositivity (POR = 1.6, p = 0.03), controlling for age and gender (Table 2). Always boiling drinking water prior to consumption approached statistical significance. Frequent exposure to ticks or mosquitoes was not associated with seropositivity.
Geospatial analysis
Tularemia prevalence in each village ranged from 0% to 50% (Fig. 1). Significant geographic clustering was observed. Average annual precipitation, precipitation in the driest quarter, altitude, and tick habitat suitability were significantly associated with village-level tularemia prevalence in a multivariate linear regression model (Fig. 2, Table 3). Tularemia prevalence varied inversely with precipitation in the driest quarter and altitude, but increased with annual precipitation.
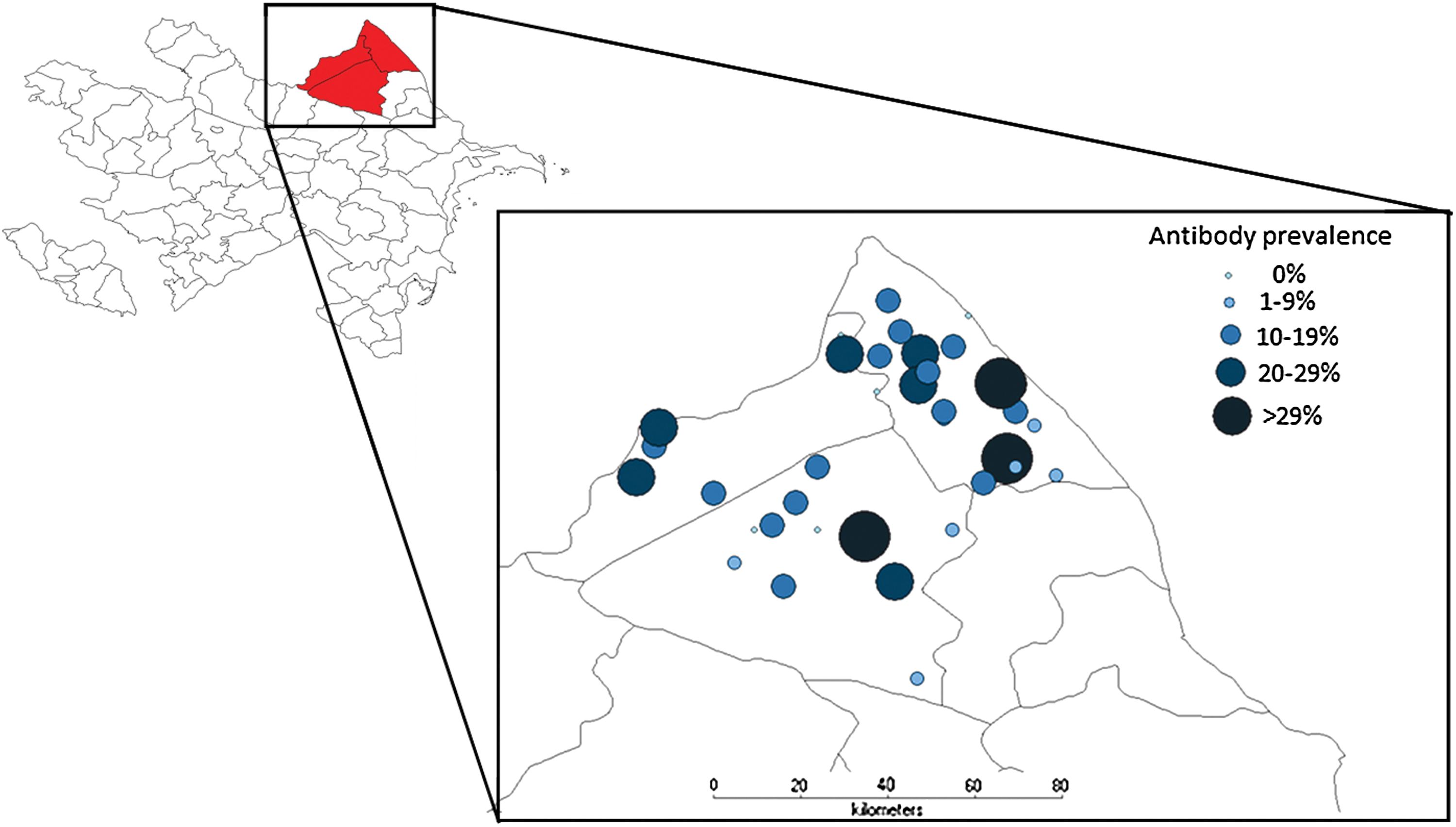
Village-level antibody prevalence. (Color images available online at
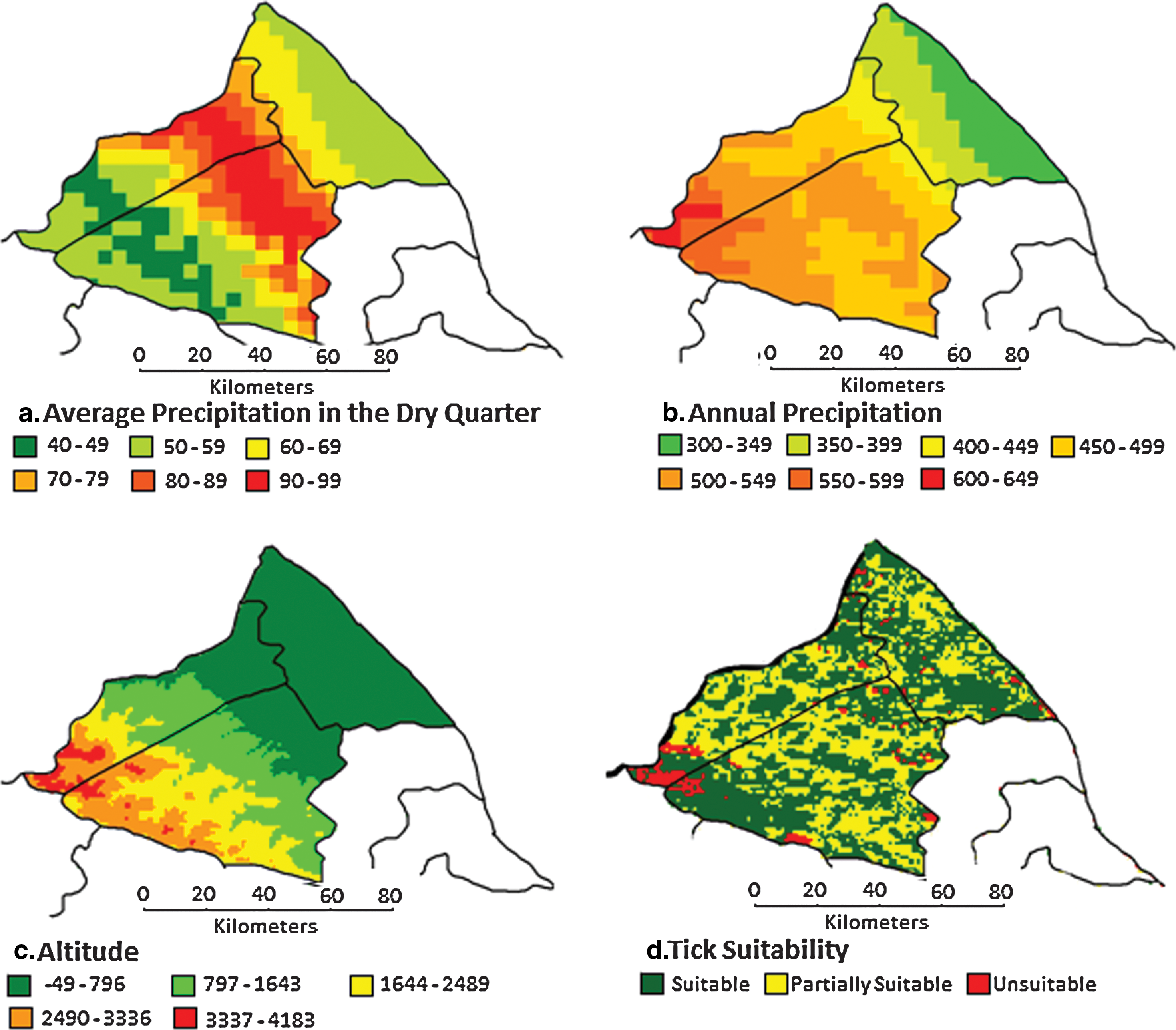
Geographic distribution of environmental parameters associated with village-level antibody prevalence. (Color images available online at
Discussion
This investigation documented a high prevalence of antibodies to F. tularensis in a rural population in Azerbaijan. This observation contrasts with the low number of volunteers reporting significant infections with lymphadenopathy, a symptom that is thought to be present in most forms of tularemia. The results imply that tularemia exposure usually does not lead to severe or significant clinical symptoms. The true proportion of symptomatic-to-asymptomatic cases is not known for tularemia. Other investigations also support the conclusion that symptomatic infections are uncommon even after tularemia exposure and that endemic populations have measurable rates of antibodies to tularemia (Feldman et al. 2003). The biovar of F. tularensis may influence these observations as well, because type A tends to be more virulent than infection with type B (Dennis et al. 2001). Another possibility is that the common routes of exposure in this population may be more likely to produce an asymptomatic infection. A low inocula of organism can cause symptoms when patients are exposed by the aerosol route (Saslaw 1961). Other routes of exposure, such as a contaminated water source, do not have clearly described levels of bacteria that cause an infection.
The epidemiologic associations with tularemia antibody presence are plausible, as the presence of rodents in the household could predispose persons to aerosolization of infected urine, and the protective effects of boiling water may reduce the risk of water-borne transmission of infection. With the plethora of potential routes of transmission, it is difficult to precisely define the exposure risk in this population. It is possible that multiple routes of exposure are responsible for the prevalence of antibodies in this population. Because of the multiple potential routes of exposure, targeting a specific public health intervention for implementation is difficult. One useful intervention is increased understanding of the infection among health-care providers in the community, thus improving the potential for early detection, treatment, and public health response.
GIS techniques have provided interesting descriptions of the impact of ecology on infectious diseases epidemiology. Utilizing these tools, our research provides further elucidation of the ecologic association with tularemia infection. Our results suggest that climates with low rainfall in the dry quarter, low altitude, and high annual precipitation are conducive to tularemia transmission. Areas of increased precipitation may be more predisposed to a number of different mechanisms of transmission. These areas may have different types of water supply, may have a greater likelihood of forestation, or may be a more suitable habitat for the rodent species that serve as reservoirs. The significant correlation of favorable tick habitats with tularemia seropositivity suggests that tick bites may be an important mode of transmission. The exact explanation of these associations is speculative at this point. As there are multiple potential routes of tularemia transmission, it is unclear which mode predominates in northern Azerbaijan. These data provide the foundation for further investigation in this region for the relationship between ecology and epidemiology of this infection.
Our results should be evaluated with consideration of certain limitations. Because of the longevity of the tularemia antibody response, seropositive individuals may have been exposed for multiple years prior to this study. Tularemia serology is a highly specific diagnostic modality; however, false-positive results are possible as tularemia assays may cross react with other infectious diseases such as brucellosis and yersiniosis at low serologic titers (Tärnvik and Chu 2007). We selected a cutoff of 4 standard deviations above the mean result for normal serum to exclude low-level cross reactive responses, even though some of the persons may have had a tularemia infection, particularly in the distant past. The geospatial analysis is limited by the mobility of a human population; exposure could have occurred in a different location for some volunteers. Even with these limitations, the initial data presented provide significant information about exposure to this infection in Azerbaijan.
The results of this investigation add to the growing understanding of the geographic distribution of tularemia. These data also provide additional information about climatic and landscape conditions that increased the likelihood of exposure in northern Azerbaijan. Further investigation should focus on the asymptomatic case rate, with our initial impression suggesting that symptomatic infection is not common. The application of these results is that public health personnel should encourage health-care providers in these areas to suspect tularemia as a potential cause of compatible clinical syndromes and prepare for occasional outbreaks.
Footnotes
Acknowledgments
Funding for this project was provided by the U.S. Department of Defense Cooperative Threat Reduction Program, implemented by the U.S. Defense Threat Reduction Agency.
Disclosure Statement
No competing financial interests exist. The views of the authors do not purport to reflect the positions of the U.S. Army or the U.S. Department of Defense.