
Abstract
In this article, a case of Crimean-Congo hemorrhagic fever (CCHF) and visceral leishmaniasis coinfection in a 14-month-old girl is reported. The case has been evaluated according to two different points of view based on the coexistence of CCHF and visceral leishmaniasis and a strongly suggested horizontal transmission of CCHF from her father. To the best of our knowledge, this coinfection has not been previously reported in literature.
Introduction
Visceral Leishmaniasis (VL) should be considered in patients with prolonged fever, hepatosplenomegaly, and cytopenia, who live in an endemic region. Leishmania tropica and Leishmania infantum are primarily responsible for cutaneous and VL, respectively, in Turkey (Toz et al. 2009). VL is sporadically seen mainly in the Aegean, Mediterranean, and Central Anatolia Regions, but cutaneous leishmaniasis (CL) is endemic especially in the Southeastern and Mediterranean Regions (Ok et al. 2002). Mean number of annual VL and CL cases reported to Turkish Ministry of Health are 102 and 6909, respectively, in the last 4 years (Ok et al. 2002, Turkish Ministry of Health, 2009). These data suggest that both VL and CL represent an important public health problem throughout Turkey.
Here, a case of CCHF and VL coinfection in a 14-month-old girl from Turkey is reported. First, she was diagnosed as having CCHF, as her father was deceased because of CCHF and the infection had passed on to her most likely through horizontal transmission. She was treated with ribavirin for 10 days. As her fever and thrombocytopenia persisted, bone marrow aspiration was performed and thus she was diagnosed as having VL. To the best of our knowledge, this clinical picture of CCHF and VL coinfection has not been previously reported in English literature. The case has been evaluated according to two different points of view based on the coexistence of CCHF and VL and a strongly suggested horizontal transmission of CCHF from her father to the patient.
Case Report
A 14-month-old previously healthy girl was referred from an endemic region for CCHF with a history of high fever and diarrhea and with progressively worsening neutropenia, thrombocytopenia, and elevated liver enzymes. It was found that her father had fever, vomiting, cough, and fecal bleeding after he had a history of tick bite. He had been diagnosed as having CCHF. He died within 5 days after the onset of symptoms. The patient had cutaneous contact with his secretions and vomits during this time. On admission to our hospital, her physical examination was normal except tonsillar hypertrophy and fever (38.2°C). Laboratory studies revealed that her hemoglobin (Hb) was 7.3 g/dL; hematocrit, 24.7%; white blood cell count, 5.1 × 109/L (20% neutrophils, 70% lymphocytes, and 10% monocytes); platelet count, 87 × 109/L; aspartate aminotransferase, 110 U/L; alanine aminotransferase, 111 U/L; lactate dehydrogenase (LDH), 530 IU/L; C-reactive protein, 9.8 mg/dL; activated partial thromboplastin time, 25.3 s; prothrombin time, 17.4 s; and international normalization ratio, 1.43. Serological studies for toxoplasmosis, Epstein-Barr virus, cytomegalovirus, rubella, hepatitis A, B, and C, parvovirus, and herpesvirus type 1 and 2 were all negative. Further, screening for Salmonella and Brucella antibodies were also negative. As her clinical and laboratory findings were suggestive of CCHF and her father died with confirmed diagnosis of CCHF, her serum samples and DNA were studied for CCHF. Serum samples of the patient were negative for anti-CCHF IgM and IgG, whereas real time (RT)–polymerase chain reaction showed positive result for CCHFV. Segment S sequence analysis of CCHFVs detected in the father (KSTM_HS_59009) and his daughter (KSTM_BS_65209) was performed to investigate the similarity of the individual viruses. A total of 374 and 366 nucleotides were sequenced from the father and his daughter, respectively. The sequences were submitted to GenBank and assigned with GU084161 and GU084162 accession numbers. The analysis of the sequences revealed that both sequences were identical (100% identity for overlapping sequences and 98.7% identity for whole sequences) to each other and phylogenetically closely related to local CCHFVs (data not shown) previously reported (Burt et al. 1997). This finding is strongly suggestive of horizontal transmission of CCHF from the father to the patient.
After the diagnosis of CCHF, ribavirin treatment was started with a dosage of 30 mg/kg/day and continued with a dosage of 15 mg/kg/day for 10 days. Although ribavirin treatment and intensive supportive therapy were given, her clinical condition was not very well and pancytopenia and elevated liver enzymes persisted on her laboratory studies. On her physical examination, mild hepatosplenomegaly was still continuing, and both liver and spleen were 2 cm below the costal margin. On the 26th day of hospitalization, her Hb was 7.4 g/dL; white blood cell count, 3.3 × 109/L; and platelet count, 116 × 109/L. Additionally, her triglyceride was 254 mg/dL (range: 0–200); total protein, 8.2 g/dL (range: 6.6–8.7); albumin, 2.6 g/dL (range: 3.4–4.8); fibrinogen, 458 mg/dL (range: 175–400); aspartate aminotransferase, 137 U/L; alanine aminotransferase, 143 U/L; LDH, 667 U/L; and ferritin, 70 ng/dL (range: 5–148). Other biochemical parameters were all normal. Fever, pancytopenia, hypertriglyceridemia, elevated liver enzymes, and LDH levels suggested that hemophagocytic syndrome might have been developed secondary to infection. Hemophagocytosis was not seen on her bone marrow aspiration smears, whereas surprisingly a large number of intracellular and extracellular Leishmania amastigotes were observed on her smears (Fig. 1). The diagnosis of VL was confirmed with serological studies and the infection was successfully treated with liposomal amphotericin B. One month after discharge, on her first follow-up visit, she was in good clinical condition and her pancytopenia and elevated liver enzymes were finally recovered.
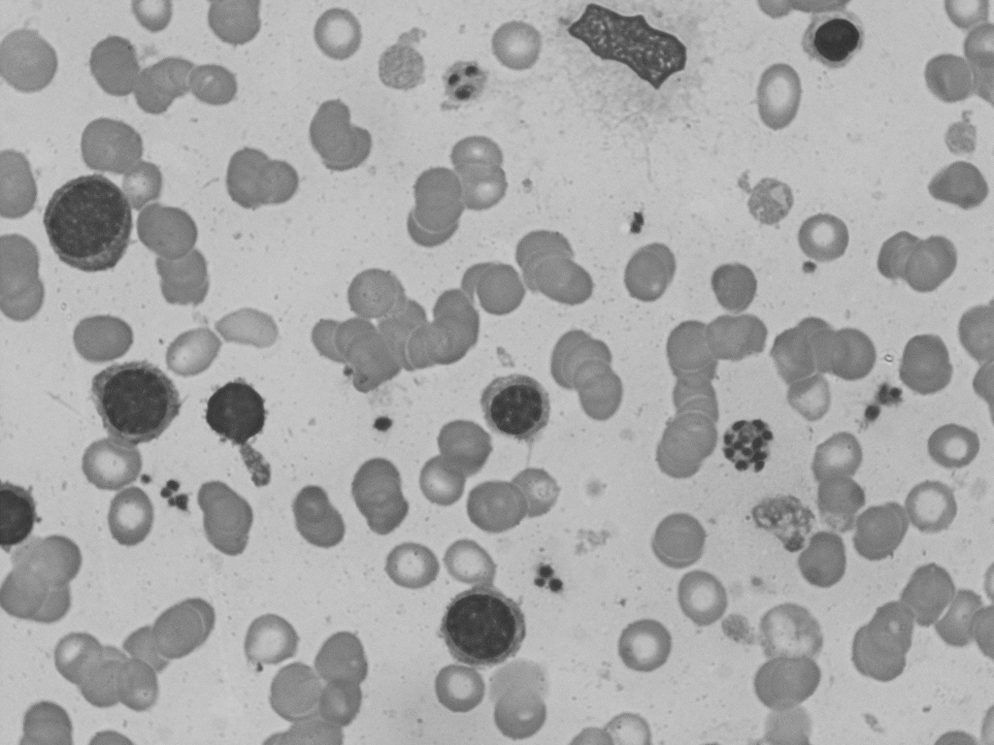
Intracellular and extracellular leishmania amastigotes on bone marrow aspiration smears.
Discussion
This case of CCHF and VL coinfection had a favorable outcome despite the fact that both infections can be potentially fatal, especially when they were not diagnosed early and/or appropriately treated. As far as we know, CCHF and VL coinfection has not been previously reported in English literature. In Turkey, both CCHF and VL are not rare with respect to other countries; therefore, these two infections might have incidentally occurred in our patient, or CCHF was the first infection and it might have altered the immunity of the patient, making her susceptible to another infection. Knowledge about CCHF pathogenesis is still limited and there is no information about the specific target cells of CCHFV. Immunohistochemistry and in situ hybridization analyses showed that the mononuclear phagocytes, endothelial cells, and hepatocytes are main targets of CCHF infection. Infection of these cell types may play a critical role in the pathogenesis of CCHF (Ergonul et al. 2004).
In our patient, the result of viral segment S partial sequence analysis was same as that for the CCHFV of the father. This finding is strongly suggestive of horizontal transmission of CCHF from the father to the patient. It is also an extremely rare event, because the transmission of CCHF between family members has been previously reported in only one case and our patient is the second in this respect (Saijo et al. 2004).
In a study performed by Izadi et al. (2008), a total of 79 serum samples from 57 close relatives of 12 newly diagnosed, serologically confirmed CCHF cases were tested and only 1 of these samples was found to be positive for anti-CCHF IgG (1.8%). This sample was taken from a brother of an index case. As a result, the transmission risk of CCHF via common routine contacts between patients and their family members and close relatives appears to be very low. In most reports regarding human-to-human transmission of the disease, transmission has occurred mostly by piercing injuries with infected objects or by mucous membrane contact with infected fluids (Centers for Disease Control and Prevention 1985, Athar et al. 2003).
The differential diagnosis of CCHF shows differences according to geographic location and includes bacterial, viral, and noninfectious etiology. Particularly, differential diagnosis at the prehemorrhagic stage is more difficult. As the disease progresses, the clinical features becomes more clearer for the diagnosis. Some disease entities could be ruled out easily in the differential diagnosis of CCHF, such as “fever of unknown origin,” because the clinical picture of CCHF starts and ends within a 2-week period. Low Hb level at the initial phase of infection is not expected, but Hb level decreases because of bleeding. Panctopenia is very unlikely. However, pancytopenia is more prominent in brucellosis and vitamin B12 deficiency (Ergönül 2007). Some infections were reported to be found together, such as brucellosis and Q fever (Gozalan et al. 2004).
Ribavirin is the recommended antiviral agent for patients with CCHF, although its mechanism of action is not clear (Watts et al. 1989). For treatment, severe cases should be defined and selected (Ergonul et al. 2004). Hemolytic anemia, hypocalcemia, and hypomagnesemia were reported in patients treated with ribavirin for severe acute respiratory syndrome (Knowles et al. 2003, Chiou et al. 2005). None of these side effects were observed in our patients under ribavirin therapy.
In conclusion, this case is very interesting in two different points. One of them is coexistence of CCHF and VL and the other is horizontal transmission of CCHF from the father to the patient. Coinfection of CCHF with VL may occur in the leishmania-endemic countries of the developing world. In an endemic area, one should have a high index of suspicion for these types of coinfections. Prompt recognition of the infections and their treatments can be lifesaving.
Footnotes
Disclosure Statement
No competing financial interests exist.