
Abstract
During febrile surveillance in the western Java City of Bandung, Indonesia, a patient with clinical symptoms consistent with hantavirus infection was found to have elevated titers of hantavirus-specific immunoglobulin M (IgM) and IgG antibodies. A subsequent epizoological investigation demonstrated a higher prevalence of hantavirus IgG antibodies in rodents trapped in the vicinity of the patient's home compared with rodents from a control area (13.2% vs. 4.7%, p = 0.036). The Old World Seoul hantavirus was detected by reverse transcriptase–polymerase chain reaction in the organs of 71% of the seropositive rodents tested. This is the first report of a Seoul virus infection in Indonesia supported by clinical, serological, and epizoological evidences. These findings suggest that hantavirus infection should be on the clinical differential diagnosis when acutely ill febrile patients report for care in western Java.
Introduction
Humans can become infected with hantaviruses through contact with urine, saliva, or feces from infected rodents, and evidence of HTN and Seoul virus infections have been reported in Southeast Asia. In Indonesia, the presence of hantavirus (Ibrahim et al. 1996) and Seoul virus (Plyusnina et al. 2004) antibodies in rodents has been demonstrated. However, reports of hantavirus infections in humans are limited. In 2001, acute sera from 2 of 25 suspected dengue patients from Yogyakarta, central Java, were positive for hantavirus immunoglobulin M (IgM) and IgG as determined by immunofluorescence assay (Praseno and Nirwati 2008). In separate studies, hantavirus IgM antibodies were found in 10 of 94 (Groen et al. 2002) or 20 of 118 (Suharti et al. 2009) suspected dengue patients from Semarang and Yogyakarta, central Java. In this report, we present clinical findings from a patient in western Java with elevated titers of IgM and IgG antibodies against hantavirus and demonstrate evidence of Seoul virus infection in rodents captured near the patient's home. This is the first report of a Seoul virus infection in Indonesia supported by clinical, serological, and epizoological evidences.
Materials and Methods
Patient enrollment
Hospital-based surveillance for hantavirus was conducted at two large hospitals in Bandung, West Java, Indonesia, from September 2004 to August 2005. Patients eligible for enrollment were hospitalized patients >10 years old who met the clinical criteria of suspected HFRS or HPS (acute renal failure with unknown etiology or fever with at least one of the following symptoms: hemorrhagic manifestations, platelet count <100,000/mm3, renal insufficiency, liver dysfunction of unknown etiology, and/or noncardiogenic pulmonary edema). After obtaining informed consent, blood samples were taken during admission and when discharged or at least a week later. Samples were first screened by reverse transcriptase–polymerase chain reaction (RT-PCR) and serology for evidence of acute dengue infection. Patients RT-PCR positive for dengue or with dengue IgM results that increased between acute and convalescent samples were not tested further. This study was reviewed and approved by the Ethical Commission of the National Institute of Health Research and Development, Indonesian Ministry of Health, Jakarta, Indonesia, and by the Institutional Review Board for the ethical conduct of research on human subjects at the U.S. Naval Medical Research Unit No. 2, Jakarta, Indonesia.
Rodent trapping
Rodents were trapped for three consecutive nights at each study site. Domestic area trapping was conducted by placing one Sherman (H.B. Sherman Traps, Inc.) and one Tomahawk (Tomahawk Live Trap Co.) trap inside the house and one Tomahawk trap outside the house. Peridomestic trapping was conducted by placing Tomahawk traps at 5-m intervals in a straight line. All rodents were euthanized, and field identification of the animal species was made by a mammalogist. Blood and tissue samples were collected from the rodents and placed in liquid nitrogen. All aspects of animal use were conducted using protocols approved by the U.S. Naval Medical Research Unit No. 2 Institutional Animal Care and Use Committee and the National Institute of Health Research and Development, Indonesian Ministry of Health.
Serology
Human serum samples were tested for the presence of dengue-specific IgM using a commercially available kit (Focus Diagnostics) according to the manufacturer's instructions. Human serum samples were tested for the presence of IgM and IgG antibodies against hantavirus using a commercially available ELISA kit (Focus Diagnostics) according to the manufacturer's instructions and by an in-house ELISA using HTN virus antigen from HTN virus-infected Vero E6 cell cultures (kindly provided by Dr. Ross Graham, USAMRID). A capture ELISA was run to detect the presence of IgM from human samples. Briefly, samples diluted 1:100 in serum dilution buffer (phosphate-buffered saline, 0.1% Tween-20, and 5% Bacto skim milk) were added to 96-well microtiter plates (Immulon 2; Dynex Technologies) coated with anti-human IgM antibodies (1:500; Kirkegard and Perry). After incubation and washing, HTN antigen diluted 1:6 in 2% normal human serum was added. After incubation and washing, anti-HTN rabbit IgG (1:2000), horseradish peroxidase-conjugate anti-rabbit IgG (1:2000), and ABTS substrate (Kirkegard and Perry) were used to detect antigen–antibody binding.
An indirect ELISA was used to detect anti-HTN IgG from human and animal samples. Horseradish peroxidase-conjugated anti-human IgG (Fc specific; Axell), anti-mouse IgG, or anti-rat IgG (Kirkegard and Perry) were used depending upon the species tested. A panel of normal sera was used to determine the cutoff. A sample was considered positive if its optical density (OD) value exceeded the mean plus 3 standard deviations of the normal sera. The endpoint ELISA titers were determined by retesting ELISA-positive samples at serial fourfold dilutions beginning at 1:100. The largest dilution giving a positive result was considered the endpoint titer.
Molecular analysis
RNA was extracted from human serum samples using the QIAamp Viral RNA kit (Qiagen) or High Pure RNA Tissue kit (Roche Applied Science) for tissue samples, according to the manufacturer's protocol.
RT-PCRs to detect dengue virus were performed as previously described (Lanciotti et al. 1992). RT-PCRs to detect hantaviruses were performed using primers specific for each genus, HTN, Seoul, Dobrava, Puumala, and Sin Nombre, as previously described (Dekonenko et al. 1997).
A hantavirus real-time quantitative RT-PCR protocol was also performed in separate reactions using hantavirus group-specific primers and probes specific for Dobrava, HTN, Puumala, and Seoul viruses as previously described (Aitichou et al. 2005). Positive results were confirmed by sequencing. Contigs were aligned using Sequencher 4.9, and BLAST was performed against the GenBank database.
Results
Hospital-based surveillance for hantavirus was conducted at two large hospitals in Bandung, West Java, Indonesia (Fig. 1), from September 2004 to August 2005. Patients eligible for enrollment were hospitalized patients >10 years old who met the clinical criteria of suspected HFRS or HPS (acute renal failure with unknown etiology or fever with at least one of the following symptoms: hemorrhagic manifestations, platelet count <100,000/mm3, renal insufficiency, liver dysfunction of unknown etiology, and/or noncardiogenic pulmonary edema). A total of 406 hospitalized febrile cases were enrolled in the study. Patients were first screened for evidence of recent dengue infection using RT-PCR and serology. Patients who were negative for dengue infection were then tested for evidence of hantavirus infection using RT-PCR and serology. The majority of patients (311/76.6%) had evidence of recent dengue infection, and one patient was positive for high titer hantavirus antibodies. Details from the patient with high titer hantavirus antibodies are described below.

Map of study location.
A 25-year-old previously healthy man presented for treatment at a hospital in Bandung, West Java, Indonesia, on January 5, 2005. The patient suffered from a sudden onset of fever of 5 days in duration, headache, nausea, vomiting, and abdominal discomfort and complained of a loss of appetite and malaise. He lived in a rural area near Bandung and reported no history of travel outside the immediate area. The patient was feverish (39°C) and had a positive tourniquet test, but no conjunctivitis. He was eupneic, with a normal blood pressure (120/80 mmHg) and pulse rate (80 min−1). Routine laboratory blood screening showed a normal leukocyte count (9600 mm−3), hematocrit (50%), blood urea nitrogen (25 mg/dL), and creatinine (0.9 mg/dL). The patient's platelet count (42,000 mm−3), blood protein (5.8 g/dL), and albumin levels (3.3 g/dL) were low and his serum transaminases elevated (SGOT: 130 U/L and SGPT: 76 U/L). The following day (day 6 of illness) his temperature decreased (38°C), and his platelet count dropped slightly (38,000 mm−3) while his hematocrit remained stable (51%). On day 7 of illness, the patient had defervescence (37°C), and his platelet count increased to 80,000 mm−3. On day 8 of illness, his platelet count was above 100,000 mm−3, and the patient was discharged from the hospital. Blood chemistry tests repeated on day 17 revealed normal blood urea nitrogen (24 mg/dL), normal creatinine (0.9 mg/dL), decreasing serum transaminases (SGOT: 44 U/L and SGPT: 46 U/L), and normal total protein (6.3 g/dL) and albumin (3.7 g/dL).
Sera were collected on illness days 8 and 17 for diagnostic tests. A commercially available ELISA kit (Focus Technologies) detected high and increasing levels of anti-hantavirus IgM (index >1.1 = positive; day 8 sample index = 18.5 and day 17 sample index = 20.6) and high levels of anti-hantavirus IgG (index >1.1 = positive; day 8 and 17 sample index = 23.2). An in-house ELISA also detected high and increasing titers of anti-hantavirus IgM (day 8, 1:1600; day 17, 1:6400) and IgG (day 8, 1:1600; day 17, 1:6400). A diagnosis of hantavirus infection was reported to hospital officials.
To follow-up on the suspected case and determine the prevalence of disease among rodents in the area, a field study was conducted at 10 months after the patient presented to the hospital. Rodents were trapped around the patient's home, which was also his working space (case area), and around a nonhantavirus patient's home (control area) ∼4 km away. A total of 245 rodents were trapped, 159 from the case area and 86 from the control area. R. norvegicus was the most predominant in both areas (74.8% and 69.8%), followed by Rattus tanezumi (22.6% and 22.1%) and Mus musculus (2.5% and 8.1%) (Table 1). Sera from trapped rodents in the case area and the control area were tested for anti-hantavirus IgG. A higher percentage of rodents positive for hantavirus-specific IgG was detected from the case area when compared with the control area (13.2% vs. 4.7%; chi-square test, p = 0.036). Twenty-four of the positive rodents were R. norvegicus (24/179 = 13.4%), whereas one was R. tanezumi (1/55 = 1.8%) (Table 1). Within the case area, there was a difference in the mean distance from seropositive rats to the patient's home compared with the mean distance from seronegative rats to the patient's home (49.9 vs. 77.5 m; chi-square test, p = 0.043) (Fig. 2).
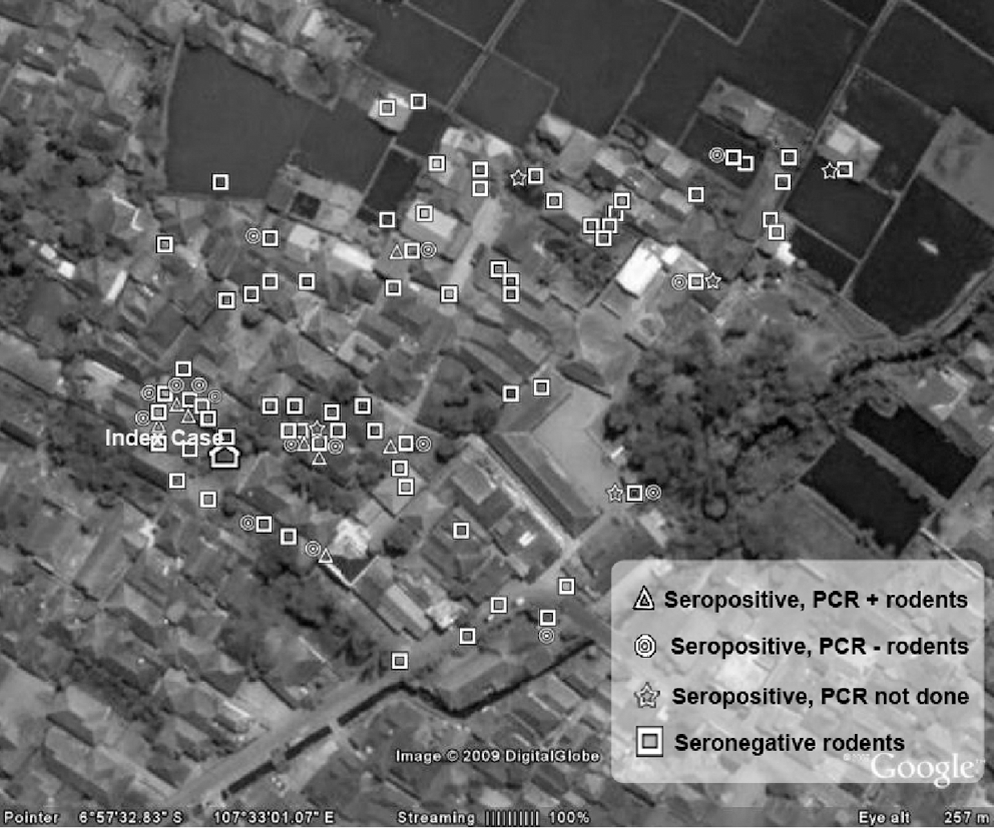
Map of patient's home and distribution of trapped rodents.
IgG, immunoglobulin G.
RT-PCR was conducted on lung, kidney, spleen, and liver samples from 13 randomly chosen, IgG-positive rodents from the case area, and the 4 IgG-positive rodents from the control area. Seoul virus was amplified in 9 of the 13 rodents selected from the case area and in all 4 of the rodents selected from the control area. Seoul virus was most commonly detected in the lungs (9/17, 52.9%), followed by the spleen (6/17, 35.3%) and kidney (6/17, 35.3%), and no rodents had RT-PCR–positive livers (Table 2). Sequence analysis of a 225-bp region of the S segment from two specimens collected in the case area demonstrated 99% identity with the S segment of a Seoul virus isolated from an R. norvegicus in Singapore (GQ 274945 Seoul virus isolate Singapore/06).
Discussion
Hantavirus surveillance was conducted in hospitalized patients in West Java, Indonesia, between September 2004 and August 2005. During this time, the majority of enrolled patients had evidence of recent dengue infection, and one patient had serological evidence of hantavirus infection. In this patient, high and increasing titers of antibodies against hantavirus were detected; however, direct determination of the specific hantavirus serotype was not possible as the patient's PCR results were negative and the facilities required to perform the necessary neutralization assays were not available. To further investigate this case, an epizoological investigation was conducted. Results of this investigation demonstrated a higher seroprevalence of hantavirus-specific antibodies in rodents trapped near the patient's home/work compared with rodents trapped in a control area, and Seoul virus was detected in most of the seropositive rodents. Although previous molecular evidence had demonstrated the presence of Seoul virus in rodents collected from central Jakarta (Plyusnina et al. 2004), this is the first report of its presence in Bandung, West Java. Clinical data also support the diagnosis of Seoul virus infection, as Seoul virus infection is milder than HTN virus infection, and is frequently accompanied by hepatic involvement (Chan et al. 1987, Hart and Bennett 1999) with no or minimal renal disease (Peters et al. 1999, Chandy et al. 2009).
Clinically mild hantavirus infection is undifferentiated from other viral or bacterial infections, especially dengue, which is endemic in Indonesia. Because many suspected dengue cases are not laboratory confirmed, hantavirus may represent the true etiology of some of these cases. In central Java, hantavirus IgM has been previously reported in up to 17% of suspected dengue cases (Groen et al. 2002, Praseno and Nirwati 2008, Suharti et al. 2009); however, this work in western Java detected evidence of hantavirus infection in <1% of the patients tested. The differences in the reported prevalences between these two locations could be due to differences in methodology or a true difference in prevalence between these two locations. Thus, to determine the prevalence of this disease among febrile patients throughout Indonesia, additional systematic studies should be conducted.
Footnotes
Acknowledgment
This study was supported by the U.S. Army Medical Research Institute for Infectious Diseases.
Disclaimer
The opinions or assertions expressed herein are the private views of the authors and are not to be construed as representing those of the U.S. Navy, the Department of Defense, or the Indonesian Ministry of Health.
Disclosure Statement
No competing financial interests exist.