
Abstract
Lyme disease (LD) is rare in British Columbia (BC) and, despite being a reportable condition since 1994, may be underreported. Here we review all provincial laboratory and clinical databases to determine the number of LD cases reported in BC from 1997 to 2008. We analyzed demographic characteristics of LD cases and used capture–recapture methodology to estimate the true number of cases in BC for this period. From 1997 to 2008, 93 confirmed cases of LD were reported in BC. Conservative capture–recapture estimates place the true number of LD cases in BC during this period at 142 (95% confidence interval: 111–224), indicating up to 40% underreporting of this rare disease. Despite this underreporting, BC continues to have low endemic risk of LD. Strategies are needed to increase both physician awareness and the use of preventive measures in the BC population, including for those traveling to other endemic areas.
Introduction
Difference in incidence between eastern and western North America may arise because I. pacificus is a less competent vector of LD than is I. scapularis (Steere 2001, Steere et al. 2004). Alternatively, significant under diagnosis and underreporting of LD by physicians, perhaps because of low awareness of disease risk, may be driving these low rates. Although such underreporting has been previously identified in other jurisdictions (Meek et al. 1996) and is common for passive surveillance systems (Doyle et al. 2002, Perry et al. 2007), Lyme advocacy groups claim that LD incidence rates in BC are actually much higher than reported because physicians are not told of the risk and miss cases, cases are not counted by public health, and laboratory testing is inadequate. They also claim that cases have increased dramatically in the past 10 years.
The objectives of this study are to (1) use capture–recapture (CR) methodology, in combination with a review of BC's three sources of passive surveillance, to provide more accurate estimates of the potential number of LD cases in BC from 1997 to 2008, and (2) to provide coarse comparisons of the burden of illness caused by LD in BC to both low incidence areas such as Washington State and California, and to highly endemic areas in the eastern United States such as Connecticut. We also aim to better understand the demographics of LD cases in the same 12-year period.
Methodology
Both clinical (physician-diagnosed erythema migrans with or without laboratory confirmation) and laboratory-confirmed cases of LD have been reportable to public health authorities in BC since 1994. Information on provincial LD cases is collected in three separate databases: (1) Integrated Public Health Information System (iPHIS)—the provincial reportable disease data and case management system; (2) Laboratory database—a central database of all microbiological tests for LD conducted by the public health laboratory, the sole site where testing for LD is performed in the province; and (3) LD-enhanced surveillance database—a repository of detailed epidemiological information (e.g., exposure location) captured during public health interviews of probable or confirmed cases. Cases from these sources were included in our review if they were reported between January 1, 1997, and December 31, 2008. Ethics approval was received from the Simon Fraser University research ethics board.
We reviewed the provincial Laboratory database to identify all individuals with a positive enzyme immuno assay (EIA) test for B. burgdorferi antibodies and subsequent confirmatory Western blot (WB) testing. These individuals were initially included in a combined database with cases reported exclusively in the iPHIS or Enhanced databases. Standard diagnostic criteria set out by the Canadian Public Health Agency (Canadian Public Health Laboratory Network 2007) were then applied to all individuals in the combined database, resulting in the exclusion of individuals without (1) an appropriate clinical diagnosis (e.g., erythema migrans) or (2) positive two-step serological testing including a positive EIA and confirmatory positive WB test. The BC Centre for Disease Control Public Health Reference Laboratories adhere strictly to Centers for Disease Control and Prevention and Canadian Public Health Level 3 network guidelines (Centers for Disease Control 1995, Canadian Public Health Laboratory Network 2007). Briefly, all samples were initially screened using VIDAS EIA (bioMerieux Vitek, Hazelwood, MO), with positive or indeterminate EIA samples subsequently tested using WB IgM and IgG. For IgM and IgG, 1 out of 3 and 5 out of 10 designated bands, respectively, must be reactive to qualify as positive. Multiple tests were reconciled to specific individuals, and any individual not meeting these stringent criteria was removed from the database. Six cases with an unclear diagnosis (e.g., multiple positive WB IgG tests followed by a negative result) were referred to a team of experts comprised of a physician epidemiologist and a medical microbiologist for case determination. Again, all individuals not meeting the inclusion criteria were removed. Individuals with a positive IgM WB persisting for >10 weeks with persistent negative IgG WB were excluded.
Age and sex distributions were calculated for the entire sample. Travel information is only recorded in the Enhanced and iPHIS databases, and travel-related demographic analyses were therefore limited to cases found in either of these two databases. Cases were assumed to have acquired their infection within BC if no explicit information was provided regarding travel or travel-related exposures. Observed incidence rates for the province were calculated using population data obtained from BC Stats (BC Stats 2009). These annual rates were compared to annual incidence rates reported by Washington State, California, and Connecticut to put BC's rates in context.
CR methodologies were used to estimate the true number of LD cases in BC between 1997 and 2008, thereby providing an indirect estimate of the level of underreporting in BC. This approach estimates the true number of cases in a population based on the overlap between multiple data sources (Hook and Regal 1995). CR methodologies were first used in animal ecology to estimate wildlife counts based on successive trapping periods. The method has since been applied in the health field to estimate the completeness of cancer registries (Robles et al. 1988) and to estimate the population size of hard-to-reach groups (Aaron et al. 2003). All CR estimates presented here are calculated using the CARE-1 SPLUS package, which is designed specifically for the application of CR methodologies to epidemiological setting (Chao et al. 2001). Two primary estimation methods are used as part of this package: log-linear modeling and the sample coverage approach. Both approaches inherently take into account potential dependence between datasets (Chao et al. 2001). Deviance estimates are used to select the best fitting log-linear models, whereas the best sample coverage estimate is determined by evaluating the sample coverage parameter (Chao et al. 2001).
Results
After applying the diagnostic criteria, 1144 individuals were excluded from the original 1218 in the Laboratory testing database for failing to meet the LD case definition of a positive EIA followed by a confirmatory WB. Two individuals were excluded from the 66 cases in the iPHIS database, and 3 individuals were excluded from the 51 cases in the Enhanced surveillance database (Fig. 1). Of the three cases removed from the Enhanced database and two cases removed from the iPHIS database, three had a tick bite but had no symptoms, one cross-reacted with syphilis, and one was not a resident of BC. Considerable overlap exists between databases (Fig. 2) with 68.8% of cases (n = 64) reported in the iPHIS database, 51.6% of cases (n = 48) reported in the enhanced surveillance database, and 79.5% of cases (n = 74) in the laboratory database (Fig. 2). Reconciling the three databases and removing duplicates leaves a total of 93 confirmed cases of LD reported in BC between 1997 and 2008.
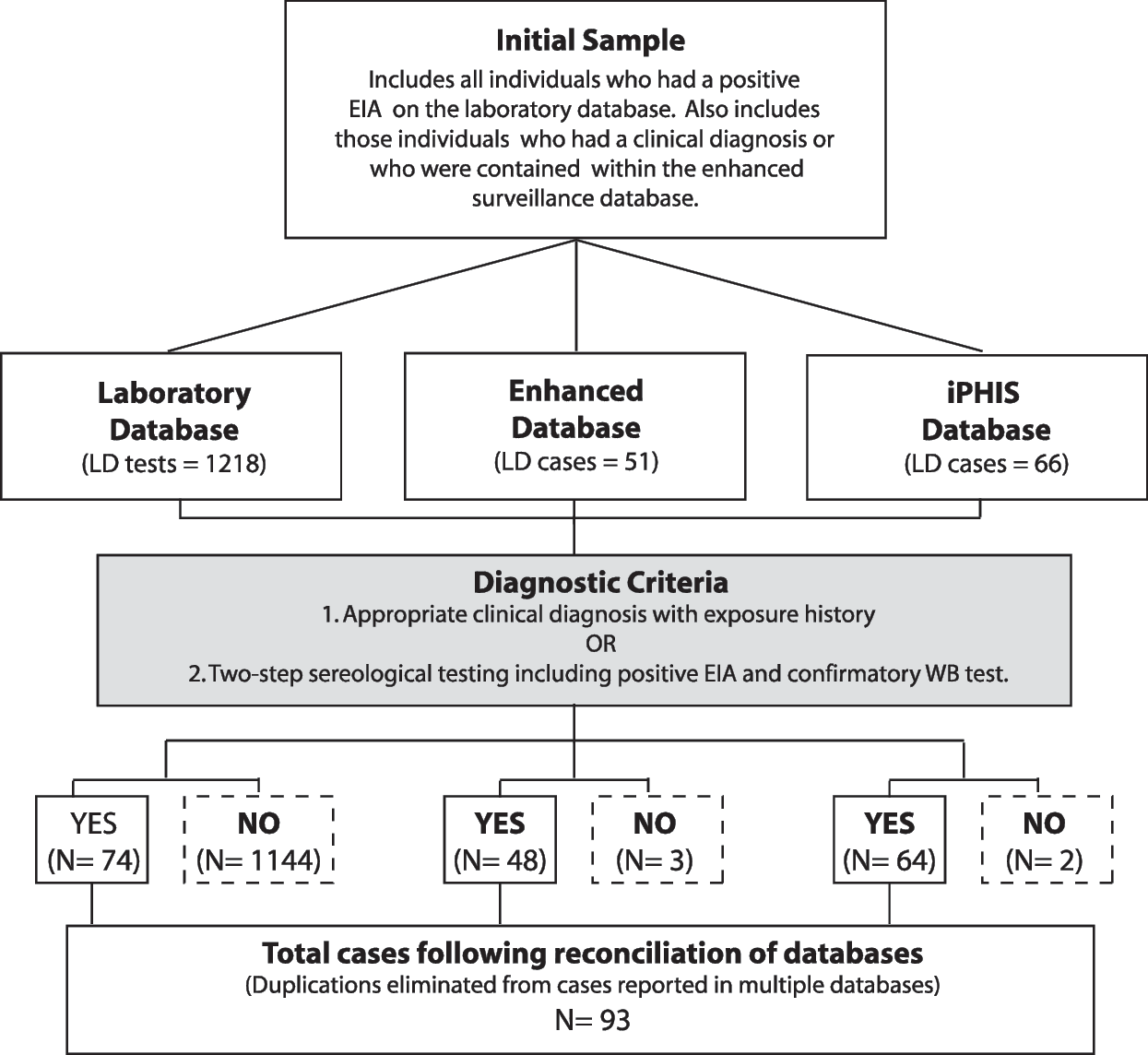
Inclusion/exclusion tree for all confirmed Lyme disease cases in British Columbia as identified from the three primary provincial databases between 1997 and 2008.
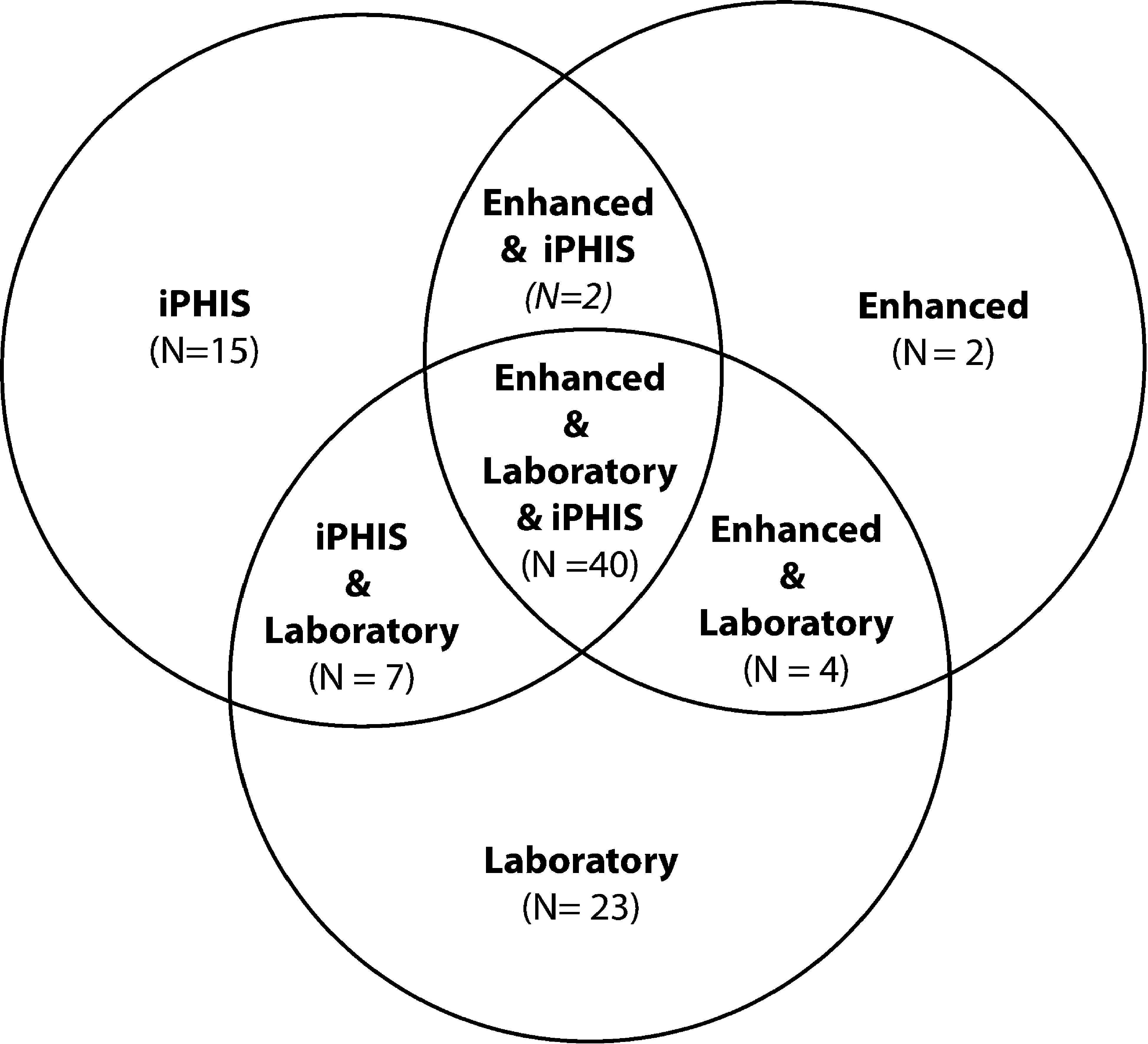
Venn diagram outlining the distribution of Lyme disease cases between the three provincial databases for the period of 1997–2006.
Of the 93 confirmed cases, 45 (48.4%) were male and 48 (51.6%) female. The majority of cases were between 41 and 70 years of age (mean = 43.7 years, standard deviation [SD] = 17.8, and median = 46.9 years) with a range of 77 years (3.5–80.6). Males were on average older (mean = 46.6, SD = 16.9, and median = 49.6) than females (mean = 41.0, SD = 18.9, and median = 43.9). Thirty-three percent (n = 23) of cases from the Enhanced and iPHIS databases likely acquired their disease while traveling outside of BC (Fig. 3). Of the 23 travel-related cases, 10 were potentially exposed in Europe (including France, Germany, Switzerland, Sweden, and Yugoslavia) and 12 traveled to areas in the United States or other Canadian provinces with known LD activity (including Ontario, New Jersey, New York, New Hampshire, and Connecticut). The mean age of travel-related cases was 40.4 years (SD = 17.9) with a median age of 42.4 years. Endemically acquired LD cases were on average slightly older, with a mean age of 44.8 years (SD = 17.8) and median age of 49.2 years.

Number of endemic and travel-related cases of Lyme disease in British Columbia between 1997 and 2008 as found in reconciled database. Travel-related cases include those individuals with exposure histories in countries with endemic Lyme disease.
The annual reported incidence of LD in BC over the 12-year period ranges from 0.1/100,000 to 0.3/100,000 population. This is comparable to LD incidence in western states such as Washington (Washington State Department of Health 2010) and California (California Department of Public Health 2010) during the same period, but is much lower than eastern states such as Connecticut (Connecticut Department of Public Health 2010) (Table 1). The true number of LD cases in BC as estimated by the CR analyses is greater than the number of reported cases, however, indicating that underreporting does occur in BC. The best fitting log-linear model, which accounts for dependencies between the iPHIS database and the Enhanced database, and between the Laboratory database and the Enhanced database, places the true number of LD cases in BC between 1997 and 2008 at 142 (95% confidence interval [CI]: 111–224). Those models that accounted for heterogeneity in individual capture probabilities had extremely large standard errors indicating a poor model fit, and are not provided in Table 2. The sample coverage CR analysis reveals high sample coverage (81%), and hence the population estimate for sufficiently high sample coverage cases is used (Chao et al. 2001). The sample coverage method provides a lower estimate of the total number of LD cases in BC of 111 (95% CI: 100–137). The sample coverage method confirms the database dependencies indicated by the best fitting log-linear model. The estimated coefficient of covariation, which quantifies the degree of dependence between two lists (Chao et al. 2001), is 0.5 for iPHIS and the Enhanced database, and 0.4 for the Laboratory database and the Enhanced database. The iPHIS database and the Laboratory database show limited overlap, with a coefficient of covariation of 0.1. Based on the most conservative upper CI of the log-linear estimate, the average yearly estimated incidence of LD in BC between 1997 and 2008 is 0.45/100,000 persons. The log-linear estimate suggests that the current existing databases in BC captured 65.5% of LD cases between 1997 and 2008, whereas the sample coverage suggests a capture rate of 83.7%.
All rates are per 100,000 population.
For sample coverage approach, M is the number of individuals in at least one database, D is the average number of individuals in a combination of two databases and not the third, and C^ is the sample coverage estimates (Chao et al. 2001).
CI, confidence interval; iPHIS, Integrated Public Health Information System; SE, standard error.
Discussion
Over the 12-year period under study (1997–2008), 93 clinically and/or laboratory diagnosed cases of LD were reported to public health authorities in BC. Slightly over half were women and the median age was 46.9 years. The proportion of female cases and median age of our cases is higher than that seen in the 10 high endemic states of the United States (median 7 years; 53% male) but in keeping with the age and percent seen in low endemic states (median 44 years; 49.4% male) (Bacon et al. 2008). One-third of these cases likely acquired their illness while traveling outside of BC, including to Europe and the eastern United States where endemic rates of LD are known to be high (Centers for Disease Control and Prevention 2007). The yearly LD incidence in BC is comparable to Washington State and California, with all three western jurisdictions having incidence rates of ≤0.5/100,000 population even when travel-related cases are included; these rates have remained stable in the last 8–12 years. In contrast, the incidence of LD in the 10 highly endemic reference states in the United States is ∼29.2/100,000 people (Centers for Disease Control and Prevention 2007), indicating that there are important differences in both disease risk and burden of illness. While the frequency of disease reporting in highly endemic states may be elevated due to increased awareness of LD, such an influence is unlikely to be the sole factor accounting for the observed variation in disease incidence. We believe that this difference is driven primarily by differences in the ecology of this disease in these regions. The 10 states with the highest U.S. incidence of LD all have I. scapularis as the primary vector rather than I. pacificus, as found in the Pacific Northwest and California (Steere et al. 2004). It is very likely that a portion of the observed risk difference is related to the greater vector competency and higher infection rates in ticks in the eastern United States (Steere 2001, Steere et al. 2004). There is also some evidence that I. pacificus ticks prefer to feed on the Western fence lizard, and that this lizard species contains a protein that effectively kills Borrelia, thereby preventing the lizard from becoming a reservoir for the infectious agent (Doggett et al. 2008).
CR analysis revealed that LD is potentially underreported by as much as 40% in this province, although the low sample size means that care must be taken when interpreting this estimate. Underreporting is common for rare diseases when passive reportable disease surveillance systems are used (Doyle et al. 2002, Perry et al. 2007). It is not known whether this underreporting in BC results from clinical cases being treated without testing and not reported or whether the cases are truly not diagnosed. Further investigation is needed into the awareness levels of physicians of the risk, clinical presentation and testing requirements for LD in BC. However, even the maximum incidence estimates using the most conservative CR results are well below those found in highly endemic areas in the eastern United States, confirming the low endemic risk in BC in contrast to claims made by some advocacy groups.
This analysis does, however, reveal the need for improved reconciliation between databases. Twenty-seven cases are recorded in the Enhanced and/or Laboratory database, but not in iPHIS database: 23 of these cases are found only in the laboratory database (Fig. 2). Currently, provincial physicians, public health experts, and laboratories use different case depositories. The discrepancies identified here are concerning given that iPHIS is the provincial reportable disease database, and indicates that improvements are needed in translating laboratory results to Public Health Agencies.
There are several important limitations to this study. First, there is the potential misclassification of the large numbers of individuals who were tested for LD but who were negative on confirmatory WB testing. Neither the specificity nor sensitivity of the tests is 100%. As a result, a small percentage of the EIA-positive/WB-negative cases likely do have LD. However, false-positives are of greater concern as the potential for false-positive EIA tests increases with the rarity of the condition (Bunikis and Barbour 2002, Doyle et al. 2002). This potential misclassification of disease status, coupled with the comparative rarity of LD in BC, means that we must interpret the result of the CR analysis with caution. Finally, CR methodology assumes a closed population, a characteristic that is not met here and may lead to underestimation of the missing data. However, the population size for most epidemiological studies remain approximately constant within a fixed period (Chao et al. 2001). Further, given the rarity of this condition in BC, the changes in population size observed over the period of study are unlikely to strongly affect these estimates.
In summary, this study suggests that while important underreporting of LD does exist in BC, the endemic risk remains low. These findings have important public health implications and will help address public concern regarding the true incidence of the disease in BC. There is concern that global warming could lead to expansion of the ecological niche for the vector and a resultant increase in the exposure of the population to infected ticks in BC (Brownstein et al. 2005, Mak et al. 2010). Concerns about increasing risk with increasing climate warming further bolster the need for both improved surveillance and strategies to ensure both awareness of LD in treating physicians, as well as increased awareness and use of prevention measures in the population, including those traveling to areas where LD is more highly endemic than in BC.
Authors' Contribution
B.H. designed the study, reviewed all data, and played a significant role in the writing of article. D.R. carried out the data analysis, figure creation, and helped with article writing. R.R. helped create the database, and helped with data analysis and article writing. L.M. and S.M. helped with study design and data analysis. M.L. carried out the data extraction for each of the three databases. M.M. managed the analysis of all LD testing and helped with article editing. All authors reviewed and edited the article.
Footnotes
Disclosure Statement
None of the authors have a conflict of interest with respect to this research.