
Abstract
Trypanosoma cruzi connatal transmission was studied in male and female mongrel dogs. Both dogs were experimentally infected, after which on the 20th day, lymphoadenomegaly and fever were found. Four months postinfection, they mated. At this time, Chagas disease was confirmed by two different diagnostic tests. The electrocardiogram and echocardiogram taken at the eight postinoculation month showed data consistent with ischemia, local conduction abnormalities and hypertrophy, as well as a diminished ejection fraction and left ventricular dilation, respectively. Four puppies were born and after weaning had weakness, progressive weight loss, and chronic diarrhea. Necropsy of all four showed digestive alterations and cardiac dilation. Serology in the offspring was positive for Chagas disease. The histopathological study demonstrated a cardiac chronic inflammatory process, although no parasites were found. Clinical data and serological determinations are consistent with death from advanced Chagas disease.
Introduction
T. cruzi is able to reach the fetal circulation as the result of placental inflammation, with the presence of acute and chronic inflammation, necrosis areas, giant cells, as well as parasite presence in trophoblastic cells and macrophages. The parasite in the fetus causes delayed intrauterine growth, hepatosplenomegaly, cardiac and central nervous system compromise, teratogenicity, abortion, prematurity, and stillbirths, but it can also be asymptomatic. There has been reported congenital transmission in successive pregnancies, as well as in twins (Ribeiro et al. 1988, Moreno et al. 2003, 2006, Torrico et al. 2006, Apt et al. 2008, Burgos et al. 2009). There are some contradictory reports in experimental animals, particularly in rat and mice, suggesting that congenital transmission can occur only in the mother's acute phase of the disease and that there is no transmission by way of the maternal milk (Davila et al. 1994, Moreno et al. 2006). The purpose of this study was to determine the connatal transmission of puppies born from the mating of two mongrel dogs with experimental infection and under controlled captivity conditions. We tried to determine whether the puppies born could be infected by a connatal way as well as by the clinical consequences in parents and offspring. Findings give new insights into how the connatal transmission of T. cruzi may be involved in the epidemiology of Chagas disease, which open new lines of investigation to study the congenital and perinatal features in the canine model to suggest more effective preventive measures to avoid this way of transmission.
Materials and Methods
Animals
Two mongrel dogs, male and female, three and 4 months of age, 5 kg and 8 kg in weight, respectively, were used. Before the T. cruzi inoculation, they were dewormed and vaccines against Distemper, Hepatitis, Parvovirus, Leptospira interrogans, Bordetella bronchiseptica, and rabies (Holland® and Intervet®) were given. Before the inoculation, enzyme-linked immunosorbent assay (ELISA) diagnostic chagasic serology was done. Animal handling followed the established guidelines of the International Guiding Principles for Biomedical Research involving Animals and the Norma Oficial Mexicana (NOM-0062-ZOO 1999) Technical Specifications for the Care and Use of Laboratory Animals and the experimental protocol were approved by the Bioethics Committee of the Instituto Nacional de Cardiología “Ignacio Chávez.”
T. cruzi strain
The Ninoa strain is a Mexican isolate obtained from an acute case of American Tripanosomiasis, which was observed in a female child living in Oaxaca, Mexico, in 1979 (Monteón et al. 1987, 1992, 1993). Ninoa strain of T. cruzi was maintained by serial passes in the reduviid vectors.
Experimental infection
The inoculation in dogs was done by intraperitoneal injection with 200,000 metacyclic trypomastigotes of Ninoa strain per animal. The parasites were obtained from urine and feces of triatomes and resuspended in physiologic solution.
Four months after the inoculation, the female child had her first estral cycle (common in big sized breeds); at this time, the dogs were mated in the chronic phase of the illness. The child was clinically monitorized during pregnancy until delivery.
Parasitaemia
The parasitaemia was determined microscopically by examining collected fresh blood from the brachiocephalic vein of infected animals every third day from day 10th postinfection up to the 21st day.
Physical examination
General physical examinations were done, evaluating mental state and respiratory patterns. Vital signs, including rectal temperature, beats per minute, and exploration for enlarged lymph nodes, were recorded. For body temperature evaluation, a digital thermometer (Microlife®) was used; and popliteal, submaxilary, prescapular, axillary, as well as inguinal lymph nodes were palpated, taking the zero value for normal lymph nodes, 1 for slightly swollen nodes, and 2 for very enlarged nodes.
Macroscopical heart evaluation
Cardiomegaly was evaluated by determining the heart index (organ weight/total body weight×100) and also by visual inspection for macroscopic alterations. Cardiomegaly was considered as present in the puppies when the organ index was significantly higher than that observed in healthy and noninfected puppies of the same age.
Electrocardiography
Electrocardiographic evaluations before inoculation and 8 months later were done registering the following leads: bipolar I, II, and III; unipolar AVR, AVL, and AVF; and precordial leads CV5RL, CV6LL, and CV6LU y V10 at standard speeds (Schiller AT-1).
Echocardiography
Resting, color Doppler transthoracic echocardiograpy (Phillips IE33) with a 2.75 MHz probe was performed in parents 18 months after inoculation. Image acquisition was done by means of a long parasternal axis, two- and four-chamber apical view in bidimensional mode. Left ventricular ejection fraction, width of the left ventricular and interventricular septum walls, left atrial diameter, and left ventricular end-diastolic volume were calculated.
T. cruzi anti-immunoglobulin G determination by ELISA
Anti T. cruzi antibody determination in the dogs was done by the ELISA method using as the antigen a total extraction of T. cruzi INC-9 isolate. Serological samples were drawn before and after inoculation. ELISA method was done as follows: in brief, 96 Maxisorb plates (Nunc) were coated with whole T. cruzi isolated extract (1 μg/mL) overnight at 4°C in 200 μL of NaCO3/NaHCO3 pH 9.6 (carbonate buffer). Plates were washed seven times with 215 μL PBS 1X-0.05% Tween-20 (PBS-T) and blocked with 200 μL 0.5% BSA in PBS-T (blocking buffer) for at least 30 min at 37°C. Serum samples were diluted in blocking buffer at a dilution of 1:200 in 200 μL/well and incubated (1 h, 37°C). Plates were then washed seven times, and 200 μL of peroxidase conjugated anti-dog immunoglobulin G (IgG) antibody (Novus Biologicals) was added and incubated (1 h, 37°C). Conjugate was diluted in blocking buffer 1:10,000. Plates were washed seven times, and 150 μL of peroxidase substrate OPD (Sigma) in citrate buffer, pH 4.5–0.03% H2O2, was added. The reaction was stopped 10 min later by addition of 50 μL of 5 N H2SO4. Absorbance values were determined at 495 nm in a Microplate Reader (Bio-Rad). All measurements were done twice, and data presented are the mean of the values for each dog. Offspring sera were obtained 47 days after birth, and determination of T. cruzi IgG antibody was done.
Indirect inmunofluorescence assay
Reactive ELISA sera were processed by indirect inmunofluorescence (IIF) as described next. Briefly, INC-9 T. cruzi epimastigotes suspension was placed on a slide and fixed. A 1:40 dilution of the test serum was made in 1× PBS, incubated in a humidified chamber at room temperature for 1 h, and washed under stirring in PBS thrice (5 min for each wash). The slides were covered with an optimized dilution (1:100) of fluorescein isothiocyanate-labeled goat anti-dog IgG conjugate (Novus Biologicals). The slides were examined with a UV epifluorescence microscope at 3200 and 3400 magnification for specific trypanosomal fluorescence. Positive fluorescence was defined as detection of green fluorescence on parasites and was labeled with +/++++ according to the fluorescence degree watched, using a positive control as reference point.
Necropsy and histology
Corresponding necropsies in the puppies obtaining the necessary tissue samples were done. Paraffin-embedded cardiac tissue sections of approximately 3 cm3 were stained with hematoxylin-eosin and examined under a Nikon light microscope. Three to six digital images from each of the cardiac walls were taken at 10× magnification with a Nikon, HP, or Cannon digital camera.
Results
Electrocardiograms as well as physical and immunological exams from both parents done before the infection demonstrated excellent health and absence of T. cruzi infection. Parasitaemia was not detected during the analysis. At day 20 postinfection, lymphoadenopathy and fever was recorded, and infection by T. cruzi was diagnosed by means of the ELISA method (Fig. 1) and confirmed by IIF (Fig. 2) 8 months postinoculation. Electrocardiograms taken at the 8 month postinfection were suggestive of ischemia, left ventricular hypertrophy, and local bundle block. Echocardiograms done 18 months postinfection revealed a diminished ejection fraction as compared with controls (50% vs. 75%, respectively), left ventricle dilation (35.5 mm compared with 28 mm), and other abnormalities, all focusing in chronic left ventricular dysfunction (Table 1).

Enzyme-linked immunosorbent assay IgG antibody determination in experimental dogs. The results were calculated as the ratio of the absorbance of each serum sample at an optical density of 490 nm (A 490). Values greater than 0.59 were considered reactive.
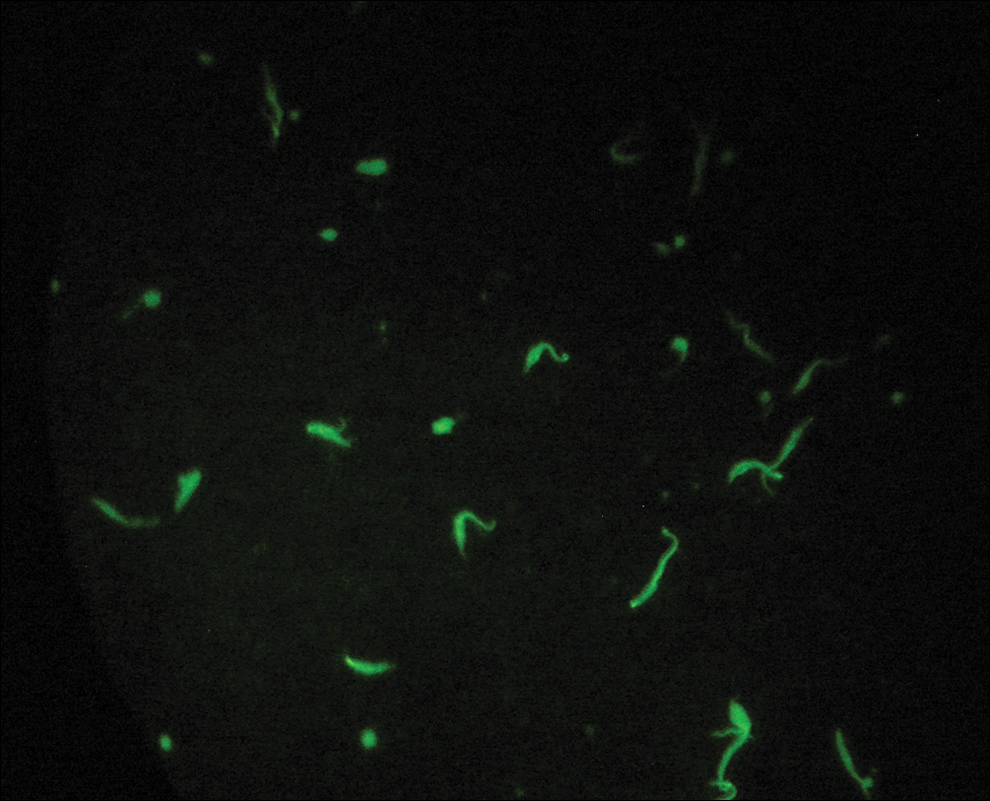
Confirmatory indirect inmunofluorescence assay for positive diagnosis of Chagas disease done in the female parent at 8 months postinfection. Color images available online at
Reference values (Tilley 1992).
Control values (healthy dogs).
Four apparently healthy puppies were born and breastfed during 45 days. Two days after weaning, Chagas disease serological exams were done, being positive in ELISA and IIF. During this period, they began to manifest clinical data, such as debility, permanent fever exceeding 40°C, slow capillary refill time, and diarrhea. They all died at 3 months of age. Puppy necropsy revealed cardiac and digestive abnormalities; with the findings of positive serology in both tests, the presence of cardiomegaly evaluated by heart index (Fig. 3), and inflammatory cell infiltration in cardiac myocytes, Chagas disease was confirmed, even though no parasites were observed.
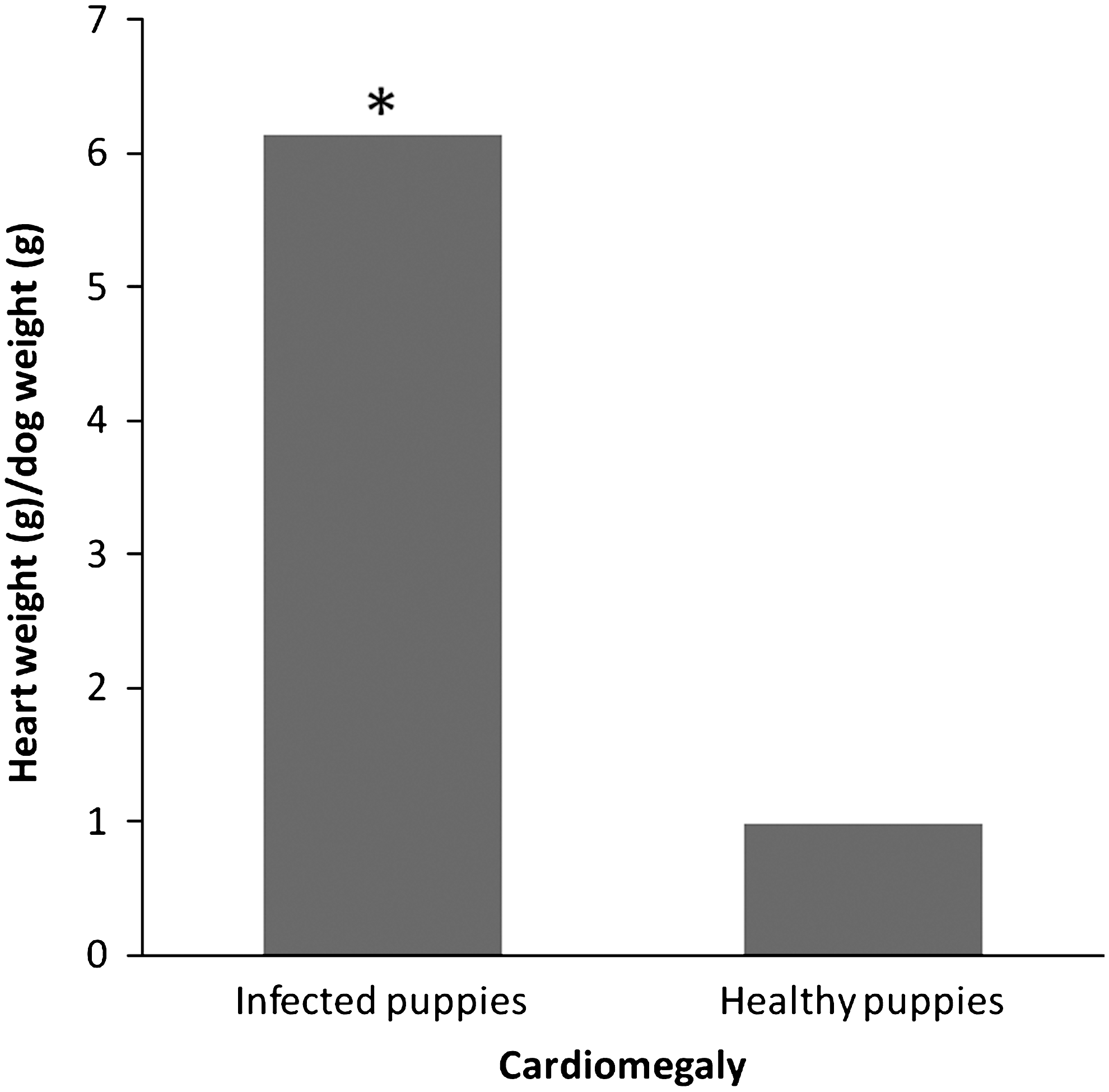
Cardiomegaly in newborn puppies born from Trypanosoma cruzi experimentally infected parents. *Statistical significance (p<0.02, Mann–Whitney test) when comparing infected puppies with noninfected animals.
Discussion
Lymphoadenopathy and fever around the 20th postinoculation day are classic signs in the acute stage of Chagas disease, supported by the positivity of ELISA and IIF done 8 months later, which are consistent with the chronic stage of the disease. These data are in accordance to those reported by Ramírez (2006), stating that in dogs after 120 days postinoculation during the chronic stage of the disease is already present.
Since the parents had the classic signs of acute stage of Chagas disease, we looked for blood parasites. These analyses were done every third day beginning at the 10th postinfection day, up to the 21st day, using thick drop microscopy. During this period, there was no parasite observation; so, the decision to terminate the analysis was taken. This is in accordance with several other publications, as it has been reported that the parasite levels in dogs tend to be so low that they are impossible to be quantified. The time extension of the parasite search was based in published literature (Machado et al. 2001, Guedes et al. 2002), where it was mentioned that the parasitaemia was evident from day 5 with a peak at days 10–12. Nonetheless, there are also reports depicting the wide time variability to obtain parasites in fresh blood. These discrepancies are due to the type of strain employed and the infection inoculum, with even further variation if the parasites are administered by different ways, if it is a reinfection, or if different parasite sources are used (blood or metacyclic trypomastigotes) (Machado et al. 2001, Bahia et al. 2002, Veloso et al. 2008).
We used the Ninoa strain, because we were looking for a well-characterized Mexican strain. This strain has been employed as an antigen source in several publications seeking to standardize diagnostic techniques, and it has been reported that there are no antigenic differences with the Y strain, which is used as a reference Brazilian strain (Monteón et al. 1987, 1992, 1993, Ramos et al. 1993).
T. cruzi Ninoa strain-infected dogs did not present a clinical state so severe that it would lead to death. This is in accordance with other reports that also use the canine model for Chagas disease, where no mortality or body weight alterations are described, and only an oligosymptomatic acute phase is observed (Machado et al. 2001, Barbabosa-Pliego et al. 2009). It is clear, however, that the disease manifestations include sudden death in acute phase or an asymptomatic form, all this depending mainly on the strain used (Barr et al. 1992).
Ischemia, conduction abnormalities, and left ventricular hypertrophy are signs of the acute phase, with progression until cardiac damage was established. These electrocardiographic signs are consistent with those found in more than 66% of human patients with chronic Chagas disease, namely conduction abnormalities found in patients who are seropositive (Montenegro et al. 1998, Sosa-Jurado et al. 2003), ischemia, and conduction abnormalities in vectorial-infected dogs (Barbabosa-Pliego et al. 2009) as well as the bundle blocks, premature ventricular contractions, and tachycardia reported in experimentally infected dogs (Barr et al. 1992). Echocardiographic findings previously described in Beagle dogs infected with T. cruzi parasite isolates obtained from wild animals (Barr et al. 1992) consist in left ventricular dysfunction, where the ejection fraction and fractional shortening diminished to 63% and 52% of control values, respectively. The same data have been shown in T. cruzi-infected monkeys (Espinola et al. 2003).
Even though human serological tests are not able to discriminate between infected and not infected newborns because of maternal IgG and IgA antibody production, which are able to cross the placenta and be present in breastfed milk (Flores-Chávez et al. 2008), the puppies had ELISA and IIF positive results 47 days after birth, confirming T. cruzi infection. It is important to remember that placenta in dogs and cats is of the endotheliocorial type, which permits only small amounts of maternal IgG to be delivered to the offspring. Approximately 90% of maternal IgG is transmitted via colostrums if the puppies are breastfed during the first 6 to 48 hrs after birth. Maternal IgG half life is approximately 8.4 days in the offspring, after which blood titles vanish (Tizard 2004, Vandeputte 2004). We found, in this study, high levels of specific IgG antibodies in the offspring and even higher in the parents, with the highest determination in the female parent. These IgG antibodies in the puppies were detected far beyond the expected mean time after birth, which allows us to state that they were offspring produced and not maternally transmitted.
Clinical and laboratory data as well as necropsy findings in all the groups of puppies we studied aimed toward the development of the acute disease (Ramírez 2006). The parasitaemia study in the puppies was done on day 47 after they were born, and the fresh blood examination was negative. Simultaneously, an ELISA was done, which turned out positive. At this time, they were in the acute phase of the disease. It should be cleared that the amount of blood obtained was limited and scarce owing to the critical status of the puppies. In the future, more sensitive parasite quantification methods in blood should be considered, such as the Polymerase Chain Reaction, which is able to detect small parasitaemia differences during the course of the infection, or between different experimental groups; likewise, the parasitoscopic concentration methods, such as the Strout or the microhematocrit tests, can enhance the sensibility up to 95% (Salazar and Marín 2006).
Inflammatory cell infiltration in cardiac tissue is a common histopathological finding in dogs during the acute stage of the infection (Caliari et al. 2002a, 2002b, Barbabosa-Pliego et al. 2009, Cruz-Chan et al. 2009) as we did find, and there have been some reports demonstrating the presence of the parasite in cardiac tissue of the dog after 10 weeks of the inoculation (Barbabosa-Pliego et al. 2009); this finding is not supported by our study, which may be explained in different ways: first, there is the possibility of the parasites absence in cardiac tissue because of different parasite concentrations in the blood, or the tissue sample obtained by us could not correspond with the portion of the heart obtained by others (Barbabosa-Pliego et al. 2009) who did not specify the portion of the heart studied, a finding reported by others (Cruz-Chan et al. 2009).
In summary, we demonstrated that death of all four puppies was from advanced Chagas disease, as proved by clinical data, serological confirmation, and histopathological study. No previous report of this experimental connatal transmission in dogs was found in the literature, giving new insights into this particular way of transmission. This far, we were not able to determine whether transmission was in the uterus, during birth, or by way of milk during breast feeding, opening new experimental lines to be done in the future.
Footnotes
Acknowledgments
We thank the staff of the Department of Echocardiography for echocardiogram recordings and data analysis; Dr. Alberto Aranda Fraustro from the Department of Pathological Anatomy for the histopathological analysis. This work was funded by the Consejo Nacional de Ciencia y Tecnología (CONACyT), Mexico, grant No. 69081 FONSEC SSA/IMSS/ISSSTE. We thank to Dr. Felipe Santibáñez Escobar for providing language help.
Disclosure Statement
No conflicting financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.