
Abstract
Cystic echinococcosis (CE) has represented a leading parasitic disease in Romania since 1862 when the first case was detected. Following the extremely high number of human and animal cases registered in 1995, Romania was framed in the forefront of Europe and among the first countries worldwide. This review aims to overview and analyze important data concerning CE in Romania from a pediatric point of view. To fulfill these goals, we focused on information provided by major epidemiological studies and rare/unusual case presentations. CE represents a serious concern for both public health services and the society, mainly because of prolonged hospitalization and convalescence periods. Moreover, the situation is much more problematic in children because physical, psychical, or intellectual impairments may impact negatively on their developmental and educational progress. The management of the disease consumes considerable healthcare resources estimated at about 1500–2000 United States Dollar (USD) for each uncomplicated case and approximately double for the complicated ones. A systematic analysis of data framed important epidemiological characteristics that may be useful when assessing individuals at risk: children (0–19 years old) represented 22.1% of the total number of cases, patients aged 13 years were most frequently affected (p < 0.0001), male patients and rural inhabitants predominated (p = 0.01 and p < 0.0001, respectively), and pulmonary involvement was detected most frequently (p < 0.0001). Considering the immense burden of this disease in Romania, emphasis should be given to the wide-scale implementation of effective prophylactic measures toward its eradication. Among them, education of the population plays an important role and should begin in early childhood.
Introduction
In Romania, CE has represented a leading parasitic disease since 1862 when the first case was detected. Besides disastrous consequences for human and veterinary medicine, the disease causes an immense economic burden (Neghina et al. 2010). Following the extremely high number of human and animal cases of CE registered in 1995, Romania was framed in the forefront of Europe and among the first countries worldwide (Iacobiciu et al. 2005).
The aim of this review was to overview and analyze important data concerning CE in Romania from a pediatric point of view.
Methods
We focused on information provided by major Romanian epidemiological studies and rare/unusual case presentations, which were published in different national books, Ph.D. thesis, and journals, most of them unavailable in international databases. Additionally, a literature search was performed in PubMed, Embase, and ISI Web of Knowledge databases using as keywords the association of the following terms: “cystic echinococcosis,” or “hydatidosis,” or “hydatid” and “Romania,” with the selection of the papers dealing with pediatric cases. Bibliographies of related works were assessed for relevant studies.
Statistical analysis was performed using the software package SPSS version 17.0 for Windows (SPSS, Chicago, IL). Descriptive statistics were calculated for each variable as appropriate. Differences in proportions were estimated by standard binomial tests. A p-value of <0.05 was regarded as statistically significant.
Epidemiological, Clinical, and Surgical Aspects
Relevant epidemiological studies regarding CE in Romania with explicit data on pediatric cases are overviewed in Table 1. The most complex studies and some details of particular interest are presented below.
Number, %, or incidence (as specified by the original source).
% represents the percentage of patients belonging to the specified group.
?, unknown; A, abdominal involvement; C, cerebral involvement; CE, cystic echinococcosis; F, female; H, hepatic involvement; M, male; NA, not available; no., number; NS, not significant; P, pulmonary involvement; R, rural regions; Re, renal involvement; S, splenic involvement; U, urban regions; y, years old.
Early information regarding cases of children who underwent surgery for pulmonary hydatid cysts were given by Juvara et al. (1958). Data provided by the Centre of Sanitary Calculation and Statistics in Bucharest for a 10-year period (1979–1988) (Iacobiciu et al. 2005) showed that children aged between 5 and 14 years predominated among the pediatric cases with CE in the entire country (p < 0.0001). Other data collected from all Romanian surgical sections (Olteanu et al. 1999, Iacobiciu et al. 2005) indicated that 371 of 3072 patients who underwent surgery for CE were children (12.1%). The distribution of the pediatric cases according to Romania's counties is shown in Figure 1, which may be used to identify the location of places referred to throughout the text. Most of the patients in the age group of 11–15 years had pulmonary involvement (57.3%, p = 0.01).

Romania's map showing counties and the capital city, Bucharest. The numbers on the map show the distribution of the pediatric cases of cystic echinococcosis (n = 371) registered during the period 1987–1991 in all Romania's surgical clinics.
A major epidemiological study was based on data extracted from the medical records of 149 children (of 1004 patients) who underwent surgery for CE in three southwestern Romanian counties (Timis, Arad, and Caras-Severin) during a 13-year period (1985–1997) (Iacobiciu 1999). The average yearly morbidity in children was 2.6 cases per 100,000 inhabitants for the studied period. Children aged between 13 and 19 years and inhabitants of rural regions were most frequently affected (p < 0.001 and p = 0.03, respectively). Lung and liver were involved in a similar percentage (46.3% and 45.6%, respectively). Pre- and postoperative complications occurred in 25 children (16.8%). Hepatic complications were found in 11.8% of cases and pulmonary complications were found in 24.6% of cases. No cases of secondary CE were detected in children.
Studies performed in Dolj County (southern Romania) (Iacobiciu et al. 2005) showed that the yearly morbidity in children ranged between 1.1 and 5.5 cases per 100,000 inhabitants during the period 1994–2000.
Studies focused on cerebral CE brought valuable information on cases managed in neurosurgical sections (Arseni et al. 1981, Ciurea et al. 1995, 2006a). Ciurea et al. (1995) reported on 27 pediatric cases in which the clinical picture was characterized mainly by headache and vomiting (96.2%), hemiparesis (70.3%), visual disturbance (44.4%), and seizures (22.2%). Papilledema was found in 88.8% of cases. Involvement of two cerebral lobes was often noticed (40.7%). The total removal of the cyst without rupture was achieved in 63% of cases and relapses occurred in 40.7% of patients.
Interesting Cases Reported in the Literature
A case of cranial CE was detected in 1957 in a 14-year-old child from a rural region who developed hydrocephalia after birth (Arseni and Sandor 1959, Arseni et al. 1981). The patient presented symptoms of brain involvement consequently to the phenomena of compression with increased intracranial pressure. These manifestations finally led to secondary papillary decoloration. The radiography of the skull evidenced a well-differentiated multicystic tumor of about 12 cm situated in the parietal region (Fig. 2a, b). The surgical intervention revealed multiple hydatid cysts (over 80) localized in the diploic space. As regards the outcome, 12 h after the intervention, the patient developed right hemiplegia accompanied by aphasic disturbances. Only a mild right hemiparesis persisted after 1 month, and the child recovered after another 4 months. The papillary decoloration was still present but no signs of recrudescence were evidenced by radiography (Fig. 2c).
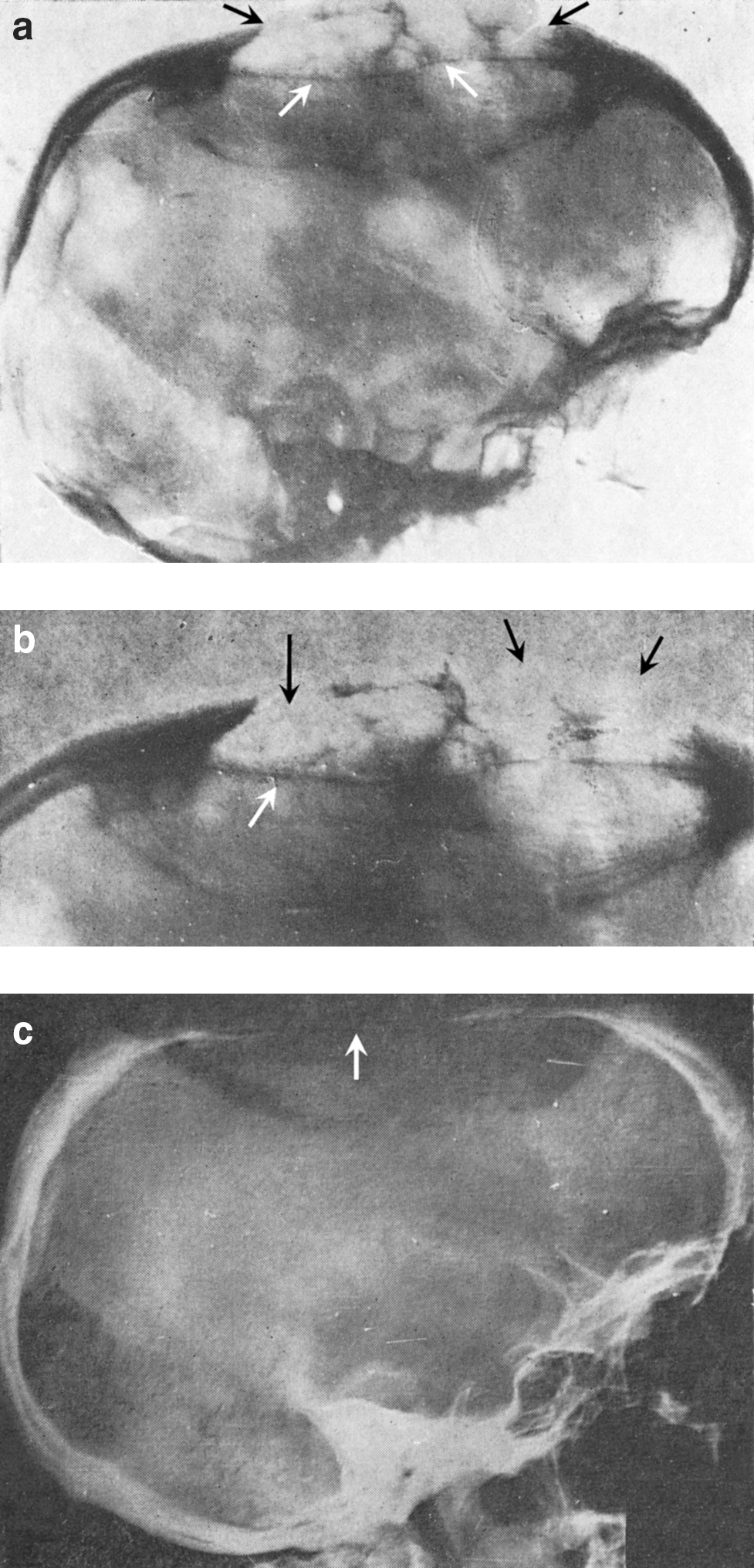
Cranial cystic echinococcosis in a 13-year-old child. (
Of interest is also the case of a patient with cerebral involvement who presented epileptic manifestations with late onset (Arseni et al. 1981). A 13-year-old child was surgically managed in 1959 for a temporoparietal tumor that consisted of one large and two smaller hydatid cysts. The outcome was favorable at about 9 years after the surgical removal. Afterward, the patient suddenly presented epileptic crisis.
Ciurea et al. (2006b) described two cases of intraorbital CE in children aged 4 and 15 years. Symptomatology consisted of nontender and nonpulsatile proptosis. Although in one of the cases the cyst ruptured accidentally during the intraoperatory intervention, the outcome was favorable (no relapses were evidenced) for both patients after surgical resection.
Recently, Tarnovetchi and Aprodu (2010) reported a case with multiple abdominal involvement. The patient, an 11-year-old boy who presented hepatic, splenic, and peritoneal hydatid cysts, had a positive history of trauma in the right hypochondrium at 7 months before hospital admission, which probably caused the rupture and dissemination of a hydatid cyst located in the liver. After an uneventful surgical intervention consisting of pericystectomy, splenectomy, and omentectomy, the outcome was favorable.
Medicosocial and Economic Implications
CE is a disease with an extremely extended clinical course. During the growth of the hydatid cyst and long time afterward, the parasitized organ is strongly affected and, sometimes, finally compromised (Olteanu et al. 1999, Iacobiciu et al. 2005). As it has been already shown (Iacobiciu 1999, Iacobiciu et al. 2005), in Romania, this malady represents a serious concern for both the public health services and the society, mainly because of prolonged hospitalization and convalescence periods. The situation is much more problematic in children because physical, psychical, or intellectual impairments may impact negatively on their developmental and educational progress (kindergarten/school absenteeism and poor performance) (Olteanu et al. 1999). An extensive study performed in southwestern Romania (Iacobiciu 1999) showed that the average hospital stay in case of the young population was 24.6 days (26.5 days in cases with hepatic involvement and 22.6 days in those with pulmonary involvement). Uncomplicated cases required 22.7 days of hospitalization (25.5 days, hepatic involvement; 18.6 days, pulmonary involvement) and complicated cases required 30.6 days (32.5 days, hepatic involvement; 29.8 days, pulmonary involvement). Of the studied group, 93.3% of children required a single hospitalization, 5.4% required two hospitalizations, and 1.3% required three hospitalizations.
According to data provided by Stefanoiu (Olteanu et al. 1999), during the years 1978–1990, 458 hospital admissions for 407 children with CE and 51 readmissions for 22 children, all aged <15 years, have been registered.
Data collected from all the surgical sections (1987–1991) (Iacobiciu et al. 2005) showed that 371 children who underwent surgery for CE required a total of 11,246 hospitalization days (average 31.3 days per child), which represented 10.52% of the total number of hospitalization days for CE in Romania.
Other studies indicated an average hospitalization period of 37.5 days per child. Three to four readmissions or surgical reinterventions and a maximum of 215 days of hospital stay have been noticed (Olteanu et al. 1999).
Further, the disease consumes considerable healthcare resources (hospitalization, surgical intervention, and drug therapy). The estimated cost for the management of an uncomplicated case of CE was about 1500–2000 USD and approximately double for a complicated case—3000 USD (Iacobiciu 1999).
Discussion and Conclusions
A systematic analysis of the data provided in Table 1 framed important epidemiological characteristics of CE in Romanian children, which may be further used as predictive factors when assessing individuals at risk.
Thus, based on appropriate information from 17 studies including 15,951 cases, children represented 22.1% of the total number of patients with CE. By overlapping the most affected age groups in 10 studies that included 1699 pediatric cases, it was shown that children aged 13 years were most frequently affected (p < 0.0001) followed by those aged 14 years (p = 0.002) and 7–12 years (p = 0.02). The pooled analysis of six studies including 332 pediatric cases demonstrated male predominance (54.9%, p = 0.01). Rural inhabitants acquired the infection in most of the cases (57.7%, p < 0.0001) as stated by two extensive studies that included 520 pediatric cases. Finally, pulmonary involvement was detected more frequently than any other complication (46.1%, p < 0.0001), followed by hepatic (32.1%, p < 0.0001) and cerebral (9.4%, p < 0.0001) involvement, as shown by eight studies that included 735 pediatric cases (studies that focused only on cerebral or pulmonary involvement were excluded).
Considering the immense burden of CE in Romania, emphasis should be given to the wide-scale implementation of effective prophylactic measures toward the eradication of this severe illness. Among them, education of the population plays an important role and should begin in early childhood. Short documentary videos/animations focused on the lifecycle of the parasite, definitive host (dog)'s role in the transmission of the disease, spread of the disease through “dirty hands” and contaminated vegetables, and the various localizations as well as the pathogenesis of the larval form in the human body should be screened in schools. Least but not last, the economic damages and medicosocial consequences of the malady must be clearly pointed out (Arseni et al. 1981).
To sum up, this review demonstrates the problematic nature of CE in Romania's young population (0–19 years old). The extremely high costs (either computable or not calculated) required for the management of each patient in conjunction with the economic loss clearly exceed the expenses of an efficient social awareness campaign intended to control and eradicate the disease. Public awareness should be heightened regarding the suffering of the diseased children and the overall impact on population health status and nation's wellness.
Disclosure Statement
No competing financial interests exist.