
Abstract
Angiostrongylus cantonensis is a parasite endemic in the Southeast Asian and Pacific regions. Humans are incidentally infected either by eating uncooked intermediate hosts or by consuming vegetables containing the living third-stage larvae. Reports on brain magnetic resonance imaging (MRI) findings and how they correlate with clinical features are limited in the literature. In this retrospective study, we investigated the brain MR features of eosinophilic meningitis caused by human infection with A. cantonensis. A detailed clinical study of 26 of these patients was conducted. The brain MRI findings were nonspecific, ranging from normal (n=1), leptomeningeal enhancement (n=21), hyperintense signal lesions (n=11) on T2-weighted MRI and nodular enhancing lesions in gadolinium-enhanced T1W1 (n=1). There was an association between the presence of brain MRI high signal intensities with peripheral eosinophilia (p=0.02), cerebrospinal fluid (CSF), eosinophil count ≥10%, and the presence of CSF antibodies to A. cantonensis (p=0.01). The patients with leptomeningeal enhancement in brain MRI tended to be younger and predominantly men (p=0.03). The time from onset of symptom to spinal tapping or brain MRI studies did not have an effect on the presence of brain MRI abnormalities. The brain MRI findings did not add any additional importance to the clinical evaluation of patients with eosinophilic meningitis in this series. Further studies are required to clarify the role of brain MRI in eosinophilic meningitis.
Introduction
Materials and Methods
All the patients hospitalized for angiostrongyliasis at the Kaohsiung Veterans General Hospital, Kaohsiung, Taiwan, during a period of 20 years (1991–2010), were recruited in this study. The clinical definition of eosinophilic meningitis was presence of recent history of eating or playing with intermediate hosts of A. cantonensis, positive specific antibody, and an acute onset of headache and eosinophilia in the blood or CSF accompanied by at least of one of the following symptoms: fever, ataxia, visual disturbance, photophobia, nuchal rigidity, neck pain, hyperesthesia, or paresthesia (Tsai et al. 2001). Eosinophilic pleocytosis was defined as the presence of ≥10 eosinophils/μL in the CSF or at least 10% eosinophils in the total CSF leukocyte count. Peripheral blood eosinophilia was defined as an increase in the percentage of peripheral blood eosinophils to more than 10% of the total peripheral blood leukocytes.
The incubation period was calculated from the time of ingestion of the putative source to onset of symptoms. Physical examinations included neurologic and ophthalmic assessment. CSF was examined for cells, protein, glucose, and larvae. Laboratory tests included a complete blood cell and differential count, liver and renal function tests, creatinine phosphokinase levels, immunoglobulin E, and an indirect hemagglutination test for amoeba. Stools were examined for parasites and amebic trophozoites. Antibodies to A. cantonensis were detected in serum and CSF by a microenzyme-linked immunosorbent assay using young-adult worm antigen, molecular weight 204 kDa, purified by monoclonal antibody (Chye et al. 2000). Cranial MRI scans were performed with a 1.5-T imager (General Electric, Waukesha, WI). Intravenous administration of gadolinium-diethylenetriamine pentaacetic acid (Berlix Laboratories, Richmond, CA) in a dose of 0.1 mmol/kg on T1 imaging was used to visualize abnormal enhancement of the meninges and cerebrum. The MRI reports were reviewed by two independent radiologists who did not know the clinical status of our patients.
Statistical analysis
Continuous variables are reported as medians and interquartile ranges. Categoric variables are reported as frequencies and percentages. Comparisons of continuous variables between groups were carried out using the Mann-Whitney U test. Comparisons between groups on categoric variables were carried out with the χ 2 (chi-square) or Fisher exact test. A p-value of less than 0.05 was considered statistically significant. Statistical analyses were performed with SPSS 17.0 (SPSS, Inc., Chicago, IL).
Results
Demographic data
Thirty-five patients were identified as having A. cantonensis eosinophilic meningitis caused by A. cantonensis infection from 1991 to 2010. Nine patients from the 1999 outbreak (Tsai et al. 2003) were excluded because of the presence of unusual brain MRI appearances (high signal intensities in the globus pallidus) not previously reported in the other series. Twenty-six patients were enrolled into the study, median age was 36 years (range, 2–80 years). Eighty percent of the patients were men. The median incubation period was 26 days (range, 3–80 days). Eighty-five percent (22/26) of the patients had identifiable risky behavior such as ingestion of snails and other intermediate hosts before the onset of eosinophilic meningitis. Their detailed clinical features and laboratory findings are shown in Table 1. Some of the clinical manifestations of patients at our hospital in whom eosinophilic meningitis was diagnosed from December 1991 to September 2009 have been reported in a Taiwanese literature (Tseng et al. 2011). The present article mainly focuses on the brain MRI findings.
CSF, cerebrospinal fluid; MRI, magnetic resonance imaging; FLAIR, fluid-attenuated inversion recovery.
The serum antibody to A. cantonensis was positive in all the patients tested. Sixty-one percent (14/23) of the patients had a positive CSF antibody to A. cantonensis. The median duration from the presence of symptoms to lumbar puncture and brain MRI were 10 days (range, 2–30 days) and 16 days (range, 3–39 days), respectively. The median duration of illness (onset of symptoms to the last day of any symptom or medication) was 25 days (range, 1–90 days). Six patients (23%) received mebendazole therapy for a median of 7 days (range, 7–10 days), and seventeen patients (65%) received steroid treatment (0.5–1 mg/kg/day prednisolone equivalent) for a median of 8 days (range, 7–14 days). The brain MRI showed that 81% of the patients (21/26) had leptomeningeal enhancement, and 42% of the patients (11/26) had increased signal intensity at the subcortical white matter of bilateral cerebral or cerebellar hemispheres on T2-weighted and fluid-attenuated inversion recovery (FLAIR) images (Fig. 1). Four percent of the patients had normal MRI findings. Seven patients had a second brain MRI study after a median of 71 days (range, 11–210 days). The brain MRI lesions remained unchanged in three patients, but disappeared in the other four patients.
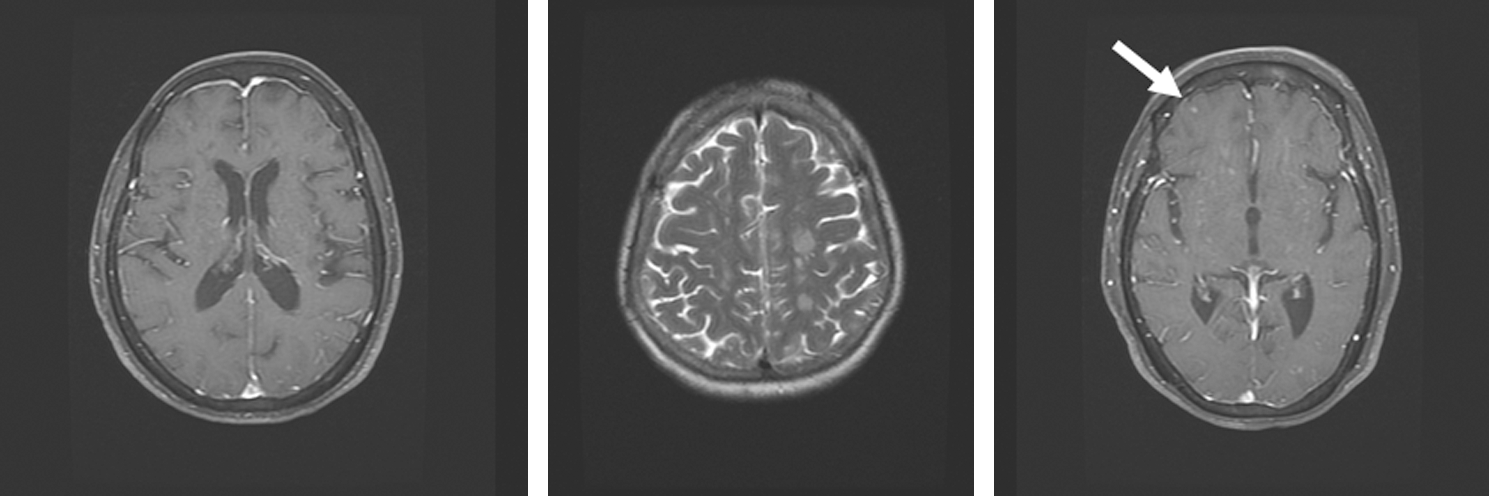
The brain magnetic resonance imaging (MRI) findings showed the presence of leptomeningeal enhancement (left), hyperintense lesions on T2-weighted MR images (middle), and nodular enhancing lesions in the right frontal area in gadolinium-enhanced T1W1 (right, arrow).
Correlation of brain MRI findings with clinical characteristics
The association between clinical presentations and MRI abnormalities are shown in Tables 2 and 3. Leptomeningeal enhancement was more frequently found in male patients (p=0.03). The patients with altered sensorium were more likely to have no meningeal enhancement (p=0.01). The detailed mechanism is unknown, and this result was probably biased by the small case number in the present series. However, there was no significant difference in the percentage of high signal intensities on brain MRI in patients with and without altered state of consciousness. The time from the presence of symptoms to lumbar puncture or brain MRI did not have an influence on the brain MRI abnormalities. This indicates that brain MRI studies can be arranged flexibly in the management of patients with eosinophilic meningitis caused by A. cantonensis. Eleven patients (42%) had an increased signal intensity in brain MRI on T2-weighted and FLAIR images. High signal intensities on brain MRI were more frequently found in patients with peripheral eosinophilia (p=0.02), CSF eosinophil count ≥10%, and patients with positive CSF antibody to A. cantonensis (p=0.01). Clinical signs and symptoms could not predict which patients were likely to have high signal intensities abnormalities in brain MRI.
IgE, immunogloulin E.
p<0.05.
p<0.05.
Discussion
The MRI findings in eosinophilic meningitis caused by A. cantonensis included leptomeningeal enhancement (Kanpittaya et al. 2000, Tsai et al. 2003, Jin et al. 2005, 2008), ventriculomegaly (Sawanyawisuth et al. 2006), prominence of the Virchow-Robin spaces (Kanpittaya et al. 2000), subcortical enhancing lesions (Kanpittaya et al. 2000, Jin et al. 2005, 2008), abnormal high T2 and FLAIR signal lesions in the periventricular and subcortical regions (Kanpittaya et al. 2000, Tsai et al. 2003, Jin et al. 2005, 2008), and high signal intensities in the globus pallidus and cerebral peduncle on T1-weighted images (Tsai et al. 2003). Three MRI abnormalities were found in this series. The presence of brain MRI high signal intensities correlated with the peripheral eosinophilia (p=0.02), CSF eosinophil count ≥10%, and presence of CSF antibodies to A. cantonensis (p=0.01), thus supporting that eosinophils play a role in pathogenic changes in the brain during eosinophilic meningitis caused by A. cantonensis. In an animal study by Sugaya et al. (2001), CSF eosinophils, shifting to hypodense status through an accumulation from peripheral blood, were resistant to apoptosis. These changes may explain the long-lasting, helminthotoxic, and neurotoxic actions of CSF eosinophils in A. cantonensis infection. Ablation of eosinophils with anti-IL-5 antibody has been shown to enhance the survival of intracranial A. cantonensis worms in mice (Sasaki et al. 1993).
The pathological findings in the central nervous system (CNS) include the following: (1) meningitis with a predominance of eosinophils and plasma cells; (2) tortuous tracks of various sizes in the brain and spinal cord surrounded by an inflammatory reaction and degenerating neurons; (3) granulomatous response to the dead parasites; and (4) nonspecific vascular reactions including thrombosis, rupture of vessels, arteritis, and aneurysm formation (Nye et al. 1970). We compared the MRI findings with the brain pathology in the literature (Nye et al. 1970), and hypothesized that the hyperintense signal intensity at the subcortical white matter in the T2-weighted and FLAIR imaging was probably caused by nonspecific vascular or inflammatory reactions. Jin et al. (2008) noted that the lesions represented focal parenchymal edema or demyelination caused by allergic or immunological reaction after invasion, death, and protein dissolution of the nematode larvae. Similar imaging findings in acute disseminated encephalomyelitis and some physiopathological conditions such as viral infection, vaccination, and insect bites can be found in the literature (Murthy et al. 1999). The enhancing nodular lesions visualized after intravenous administration of Gd-DTPA were similar to the previous findings, but were only found in one of our 26 patients. Crescent enhancement on gadolinium-enhanced T1W1, which was considered a characteristic sign of this disease by Jin et al. (2008), was not found in our patients. Formation of granulomatous nodules after the death of the worms in the brain might be the pathologic basis of the abnormal enhancement of the brain parenchyma in the present study, as in the study of Jin et al. (2008).
The current study also showed that patients with leptomeningeal enhancement in brain MRI were predominantly men (p=0.03) and tended to be younger, although the difference was not statistically significant (31 vs. 72 y/o, p=0.19). In contrast to a previous report in Taiwan (Yii 1976) where most of the patients were children and predominantly women, the current series revealed a male predominance in their third or fourth decade. This is similar to a report from Thailand (Punyagupta et al. 1975) where 70% of cases were in their third or fourth decade, and the disease was more common in men than in women in almost all age groups. It is likely that young adults are more immunocompetent and, therefore, have a stronger immune response than elderly people. It is also likely that the ingested larvae were different, thus contributing to the differences in brain leptomeningeal enhancement. In our previous study (Tsai et al. 2001), we found that the severity of illness and eosinophilia correlated with the number of ingested snails. Further studies are needed to verify this phenomenon.
We did not find an association between the brain MRI abnormalities and time from the onset of signs and symptoms to CSF study or brain MRI examination. The disease appears to be the result of a vigorous host response to larvae in the central nervous system. It spontaneously resolves presumably because the larvae do not survive in human hosts. A delay in arranging a lumbar puncture or brain MRI study did not have an effect on the abnormalities of brain MRI, supporting the theory of immune response related brain injury and the larvae being unable to survival in the central nervous system. If this was not the case, the migrating larvae would result in more severe brain pathology in the patients with delayed CSF and imaging studies.
The median incubation period in our study was 26 days (range, 3–80 days), and the time from the presence of symptoms to brain MRI was 16 days (range, 3–39 days). Therefore, it would take 6 to 119 days to see the brain MRI abnormalities from the onset of infection. This is similar to a study in rabbits, where MRI hyperintense lesions on T2-weighted MRI were first observed on day 22 postinfection (PI), and the hallmarks of abnormality were noted on day 35 PI, and remained up to day 207 PI (Wang et al. 2005).
There are some limitations to our study. First, this is a retrospective study with considerable variations in reporting and patients were limited to those who were hospitalized. However, we minimized the biases by using a standardized data-collecting form. Second, our findings were from one medical center, and they may not be applicable to other settings without brain MRI capability. Third, we did not control the use of steroids or anti-parasitic agents, and those agents might have affected the appearances of brain MRI in our series. Fourth, we did not perform follow-up brain MRI in most of the patients. However, all of the patients recovered well.
In summary, the brain MRI findings were nonspecific, ranging from normal, leptomeningeal enhancement, hyperintense signal lesions on T2-weighted MR images and nodular enhancing lesions on gadolinium-enhanced T1W1. There was an association between the presence of brain MRI high signal intensities with peripheral eosinophilia (p=0.02), CSF eosinophil count ≥10%, and presence of CSF antibodies to A. cantonensis (p=0.01). The time from symptom onset to spinal tapping or brain MRI studies did not have an effect on the presence of brain MRI abnormalities. The role of brain MRI in patients with eosinophilic meningitis needed to be further clarified.
Footnotes
Disclosure Statement
No competing financial interests exist.