
Abstract
Background:
Dengue viruses (DENV) are endemic in over 100 countries worldwide, and annually 50 to 100 million people are infected by one of the four DENV serotypes, whereas over 2.5 billion people are at risk for infection. West African countries lack the surveillance to determine the true incidence of dengue; hence, this disease is likely significantly underestimated. In Mali, ∼14 million people are potentially at risk of acquiring a dengue infection.
Methods and Findings:
A serosurvey for DENV was conducted on 95 human serum samples obtained from the Institute National de Recherche en Sante Publique in 2006. DENV-specific IgM and IgG enzyme-linked immunosorbent assays were performed on all samples, and a subset was tested using the plaque-reduction neutralization test against the DENV and yellow fever virus (YFV). Samples collected during the acute infection (0–5 days postonset of symptoms) were tested for dengue NS1 antigen and reverse-transcriptase polymerase chain reaction for Flaviviruses, Alphaviruses, and Bunyaviruses RNA. A total of 87 (93%) of samples were positive for anti-DENV IgG antibodies. Of a subset of 13 IgG positive samples, 2 samples neutralized monotypically against DENV-1 and −2, whereas 3 others neutralized broadly against YFV and multiple DENV. Although no polymerase chain reaction positives were found, DENV NS1 was detected in 1 of the 20 acute samples tested.
Conclusions:
Of the 93 human serum samples tested, the dengue prevalence based on dengue IgG enzyme-linked immunosorbent assay results was 93%. Three DENV specific positive samples and two YFV positives were identified by plaque-reduction neutralization test. Finally, one sample tested positive for dengue NS1, thus suggestive of an acute infection within 14 days of obtaining the sample from the patient. Based on these serological data from this study, YFV and DENV appear to be co-circulating in Mali.
Introduction
The annual average number of dengue fever/dengue hemorrhagic fever (DF/DHF) cases reported to the World Health Organization (WHO) continues to grow. In 2001, a record of 69 countries from the regions of South East Asia, Western Pacific, and the Americas reported dengue cases to the WHO. For the first 5 years of the current decade (2000–2005), 925,896 cases have been reported, almost double the number of cases (479,848) for the same period from the previous decade (1990–1999). Recent dengue outbreaks with suspected cases have been recorded in Pakistan, Saudi Arabia, Yemen, Sudan, and Madagascar during 2005–2006, despite the poor surveillance and no official reporting of dengue to WHO from countries in the African and Eastern Mediterranean regions (Report of the Scientific Working Group on Dengue (TDR/SWG/08) 2008).
The emergence and spread of dengue viruses (DENV) in Western Africa has become increasingly apparent over the past few years. DENV was first isolated in Western Africa in 1964 in Nigeria with the isolation of DENV-1 and -2 (Carey et al. 1971). Since then, cases of both urban and sylvatic DENV-1 and -2 transmissions have occurred in multiple countries (Diallo et al. 2003, Vasilakis et al. 2007). More recently, DENV-3 has emerged and caused epidemics in Senegal, Cape Verde, and Côte d'Ivoire (references summarized in Table 1) (Franco et al. 2010). Additionally, in October and November of 2008, Mali experienced an outbreak of over 70 cases of DF with at least 2 suspected DHF deaths. Based on traveler information, the outbreak was believed to be caused by DENV2 (Tarantola et al. 2009). As DENV serotypes continue to emerge in African countries, episodes of DHF may become more common.
This summary represents the cases identified by dengue serotype and the publication reference associated with these reports.
DENV, dengue virus; YFV, yellow fever virus.
Information regarding DENV transmission is very limited in Western Africa, with the most thorough investigations as a result of travel-associated cases imported to Europe (Ninove et al. 2009). In 2006, dengue was designated a reportable disease in France, and within 2 years, 19 imported DF cases were reported in travelers returning from Western Africa (Bulletin Hebdomadaire International 2008, Weekly Epidemiological Record, 2009). Although imported cases are an invaluable source of information, these sporadic cases cannot be used to estimate DENV transmission occurring in the region.
The study presented here provides valuable information on the population susceptibility and exposure to dengue. Our results indicated that 93% of the samples tested had reactive antibodies to dengue; hence, surveillance implementation is necessary in Western Africa to continue to monitor the transmission of DENV. This information is useful to determine when new serotypes are introduced and the possible severity of the outbreak based on the population susceptibility.
Materials and Methods
Sample collection
To assess the prevalence of dengue, 95 human serum samples were obtained from the Institut National de Recherche en Sante Publique in Bamako, Mali. Retrospective sera was acquired either by sample submissions from 28 different sentinel sites such as regional health centers or through direct collection by the Institut National de Recherche en Sante Publique team. Samples were from patients presenting with a febrile illness of unknown origin and confirmed not malaria. Of the samples with available information, 21 samples were acute (days post-onset of illness (DPO)=0–5), 30 samples had unknown DPO, and 44 samples were convalescent (DPO > 6). Samples were collected from 28 districts. Of the 95 samples submitted for testing, 2 samples had insufficient volume for any tests. This study was approved by the Institutional Review Board of the University of Bamako IRB No. BP-1805.
IgG enzyme-linked immunosorbent assay
Serum samples were aliquoted and inactivated at 56°C for 30 min before testing for all serological assays used in this study. All samples were tested using a dengue IgG antibody capture enzyme-linked immunosorbent assay (ELISA) as previously described (Miagostovich et al. 1999). Briefly, 96-well plates were coated with mouse hyperimmune ascetic fluid (CDC) to DENV 1–4 and incubated at 4°C overnight. A mixture of DENV 1–4 antigen was diluted and incubated onto the plate. Serum samples were diluted 1:100 and tested in duplicate. The final optical density (OD) value was the average obtained from the duplicates. Duplicate samples with >0.2 OD difference were re-tested. A horse-radish peroxidase (HRP) conjugated secondary anti-IgG antibody (Jackson Laboratories) was inoculated onto the plate, followed by ABTS solutions A and B (KPL). After color development at room temperature for 1 h, the plate was read using a BioTek KC4 plate reader at 405–410 nm. Samples were interpreted using the OD of the sample as follows: OD=0.15–0.49: low positive; OD=0.5–0.99: medium positive; OD=≥1.0: high positive.
IgM antibody capture-ELISA
All samples were tested using IgM antibody capture ELISA. Plates were sensitized using an anti-IgM capture antibody and incubated overnight at 4°C (Kirkegaard and Perry Laboratories). Samples were diluted 1:400 and tested in duplicate. A mixture of DENV 1–4 recombinant antigen (CDC) was diluted and incubated overnight. An HRP-conjugated flavivirus group specific antibody 6B6C-1 (CDC) was added. After incubation for 10 min at room temperature with a 3,3′,5,5′-Tetramethylbenzidine substrate (KPL), the plate was read at 450 nm. Samples were interpreted by dividing the mean OD of the samples by the mean OD of the negative control (Positive/Negative ratio). P/N values ≥2.0 were considered positive (Martin et al. 2000).
Plaque-reduction neutralization test
The plaque-reduction neutralization test (PRNT)90 was performed as previously described (Russell et al. 1967). ChimeriVax viral strains of DENV 1–4, WNV and SLEV were donated by Acambis (Pugachev et al. 2004). The yellow fever virus (YFV) vaccine strain 17D was used to test samples against YFV. Serial twofold dilutions of serum starting with 1:20 to 1:640 were used. Plates were incubated at 37°C with 10% CO2 for 3 days (for WNV), 4 days (for SLEV), and 5 days for DENV1–4. PRNT90 titer was reported as the reciprocal of the serum dilution required to reduce the number of plaques by 90% compared with the working dilution of the virus controls. When two or more viruses are reactive in the assay, a four-fold increase in titer between the viruses is used to determine the infecting virus. PRNT90 titers were used in this study because of their increased specificity compared with PRNT50. Not all samples were tested in this assay due to insufficient volume.
NS1 antigen capture ELISA
Bio-Rad Platelia Dengue NS1 Antigen Capture ELISA (Bio-Rad Laboratories) was used according to the manufacturer's instructions. Briefly, serum was diluted 1:1 in sample diluent and mixed with HRP-labeled anti-NS1 monoclonal antibody. The sample-conjugate mixture was inoculated onto plates precoated with a capture anti-NS1 antibody and incubated for 90 min at 37°C. 3,3′,5,5′-Tetramethylbenzidine substrate was added to each well and incubated for 30 min at room temperature. Plates were read at 450 nm. A sample ratio was determined for each sample by dividing the OD of the sample by the cut-off control. Sample ratios of <0.5, 0.5 to <1.0, and ≥1.0 were considered negative, equivocal, and positive, respectively.
Cell culture inoculation and reverse transcriptase polymerase chain reaction
Acute sera were inoculated onto C6/36 mosquito cell line derived from Aedes albopictus and incubated at 37°C for 5 days. After incubation, RNA was extracted from supernatant samples and analyzed by reverse-transcriptase polymerase chain reaction (RT-PCR). Since these samples were obtained from patients with febrile illness as their only clinical selection criterion, all samples were analyzed for Flaviviruses, Alphaviruses (Togaviridae family), and Bunyaviruses (of the genus Orthobunyavirus) (Kuno 1998, Lambert et al. 2009).
Results
Seroprevalence of dengue by IgG ELISA
Ninety-five human serum samples were retrospectively collected from febrile patients in a hospital in Bamako, Mali, in July 2006 from 28 different public health districts. The median age of the individuals was 23 years old, and the ages ranged from 1 to 80 years old. Twenty-five patients (26%) had previous YFV vaccination, 68 (72%) had unknown YFV vaccination status, and 2 (2%) had no previous YFV vaccination. Of the 95 samples submitted for testing, 2 samples had insufficient volume for any serological tests. Ninety-three samples were tested using the dengue IgM antibody capture-ELISA and IgG ELISA (Table 2). None of the samples tested were positive for anti-dengue IgM, and 87 (93%) samples were positive for anti-dengue IgG. Of the 87 human serum samples with positive anti-dengue IgG, 41 (44%) of these positive samples had high levels of IgG (OD=≥1.0), which is suggestive of a recent infection (Table 3) (Miagostovich et al. 1999).
Patient serum results for IgM antibody capture ELISA, IgG ELISA, NS1 ELISA, and RT-PCR based on the public health district in Mali. The results describe the distribution of samples from each region as well as the percent positive. Some samples could not be tested due to insufficient quantity of serum.
Flaviviruses/Alphaviruses/Bunyviruses.
QNS.
NT, not tested; QNS, quantity not sufficient.
ELISA, enzyme-linked immunosorbent assay; RT-PCR, reverse-transcriptase polymerase chain reaction.
A total of 93 patients were tested for anti-dengue IgG antibodies. Samples were interpreted using the optical density (OD) of the sample as follows: OD=0.15–0.49: low positive; OD=0.5–0.99: medium positive; OD=≥1.0: high positive.
Identification of infecting flavivirus by PRNT 90
The 87 patients whose serum was positive for anti-dengue IgG represented 28 public health districts in Mali. Positive IgG samples per district with sufficient volume were tested by PRNT90 against DENV 1–4 and YFV to identify the previous infecting virus. Ideally, one representative sample per public health district was assigned to be tested; however, due to low sample volume, every district with a positive IgG ELISA result could not be tested. Despite this limitation, 10 different public health districts were tested. Additionally, since a large number of the samples collected (36 patients representing 37% of the samples) were from Yanfolila, 4 samples were tested from this region.
Of the 13 samples tested, 6 (46%) did not neutralize against DENV 1–4 or YFV. Three samples (23%) produced a monotypic response against YFV with PRNT90 titers of 1:80 and 1:20, respectively. All three of these samples had an unknown YFV vaccination history. One sample from Yanfolila neutralized equally with titers of 1:20 against DENV-2, DENV-3, and YFV. Two samples from Kolokani and Macina neutralized against multiple viruses with a dominant response to DENV-2, and one samples from Bourem produced a dominant response against DENV-1. Although vaccine history was unavailable for 72% of these patients, one patient had never received YFV vaccine. The PRNT90 data are summarized in Table 4. A map of the regions where flavivirus positive serum samples were identified is shown in Figure 1.
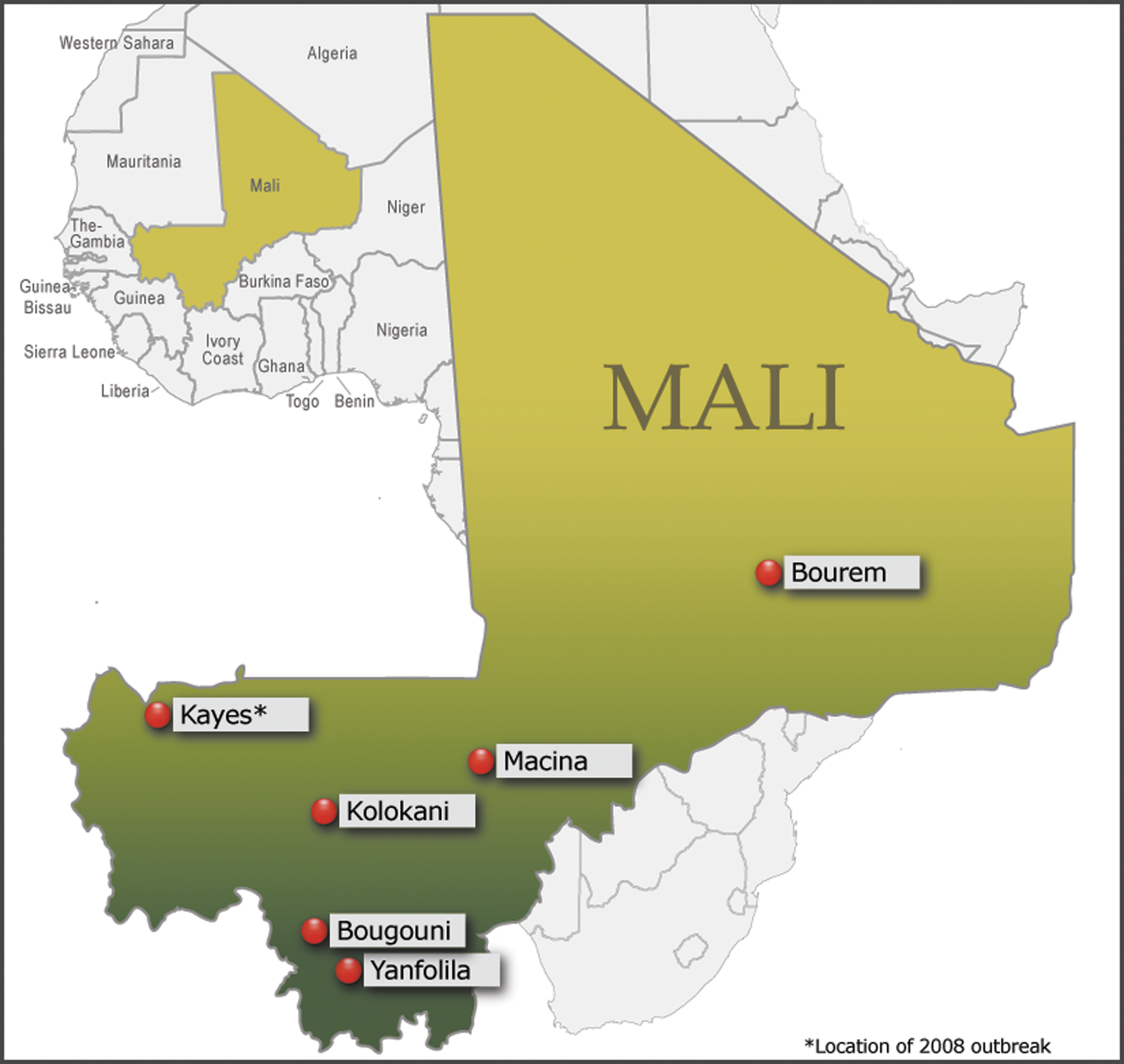
Dengue positive regions of Mali. Geographical location of the dengue positive samples identified by plaque-reduction neutralization test in the 2006 serosurvey compared with the location of 2008 dengue outbreak in coal miners in Kayes*.
All samples were convalescent defined as DPO ≥ 6.
Each value represents the end-point titer in which the serum sample neutralized against each virus. Samples with titers <20 were under the detection limit of the assay and were considered negative. The interpretation of the infecting virus was based on a ≥4-fold increase compared with the other serotypes or a negative result for the other viruses and a positive result for the infecting virus. The sample with no previous YFV vaccine was noted in the table.
DPO, days post-onset of illness; PRNT, plaque-reduction neutralization test.
Evidence of an acute dengue infection by NS1
All acute serum samples were tested using a DENV NS1 antigen ELISA. Of the 21 acute serum samples available, 20 had sufficient sample volume to perform the assay, and 1 sample was positive for DENV using the NS1 ELISA. All acute sera were also inoculated in C6/36 cells, and the cell supernatant from these samples was analyzed using nested PCR (Lanciotti et al. 1992). For positive controls, DENV-1 (Hawaii), Highland J, and LaCrosse viruses were used with the pan-flavivirus, pan-alphavirus, and Orthobunyavirus primer sets, respectively. No Flaviviruses, Alphaviruses, or Bunyaviruses were detected in the 20 samples tested.
Discussion
This study estimated the prevalence of dengue with retrospectively collected samples from patients who had febrile illness of unknown origin and confirmed not malaria from the 28 Mali health districts. The results from this study indicated that the health districts sampled in Mali had a dengue seroprevalence of 93% by anti-dengue IgG ELISA. Of the subset of these samples tested by PRNT90, 3 were DENV, 3 were YFV positive, and one was cross reactive to both DENV and YFV. However, 6 (46%) of this subset tested for PRNT90 was negative for DENV and YFV, suggesting that other flaviviruses are circulating in Mali that cross-react in the dengue IgG ELISA. Nevertheless, one sample was positive by dengue NS1 antigen, indicating an acute infection within the last 10 days of the collection of the sample during the study period, suggesting active transmission of dengue in Mali. Based on the serological data from this study, YFV and DENV appear to be co-circulating in Mali.
There were several limitations presented by using archived samples from febrile illness of unknown origin and confirmed not malaria cases that included: travel and vaccination history for patients from whom serum samples were collected; inadequate storage conditions of the samples; and insufficient volume of the samples. Additionally, there were no recent infections detected by anti-dengue IgM antibodies, and PRNT90 results indicated that the anti-dengue IgG ELISA had a lower specificity than previously measured. Thus, the representation of a 93% DENV prevalence in Mali determined by the presence of anti-dengue IgG antibodies may be an overestimate due to either YFV vaccination campaigns or natural YFV infections.
The presence of dengue-specific NS1 antigen indicated that there was current circulation in the population during the study period. NS1 antigen can be detected in patient serum during the first three to 10 days postinfection and is suggestive of an acute dengue infection. Multiple evaluations of the NS1 ELISA have reported good specificity for dengue virus ranging from 98.4% to 100% (Bessoff et al. 2008). Although DENV and YFV have been shown to cross-react in the PRNT, 2 of the samples produced a dominant response to one virus, whereas three samples did not cross-react (Houghton-Trivino et al. 2008). Further, one sample from the region of Macina came from a YFV-unvaccinated individual; this sample neutralized against DENV-1, -2, and -3, but had the highest titer against DENV-2 with no neutralizing activity against YFV. As shown in Figure 1, samples that were positive for flaviviruses were obtained from patients throughout southern Mali, but due to unequal sampling from each region, it is difficult to conclusively ascertain what regions are at highest risk for DENV transmission based on these results.
The transportation of the samples within Mali and to Puerto Rico may have contributed to the negative results obtained from RT-PCR. Multiple freeze-thaw cycles and storage of samples at −20°C in Mali may have compromised and degraded viral RNA, making detection of virus by PCR unlikely. The high seroprevalence of dengue virus antibodies in Mali determined by this study emphasizes the need to build laboratory and surveillance capacity to perform RT-PCR and viral isolation in-country. The incorporation of viral isolation capacity in Mali would allow for sequencing of these viral isolates to characterize the current circulating DENV and identify potential re-introduction of dengue via other regions versus sylvatic dengue introductions in the population (Diallo et al. 2005).
These data, in conjunction with DENV and other flavivirus outbreaks in Western Africa, indicated the need for ongoing flavivirus surveillance and more extensive prevalence information for this region. Although very limited information about flaviviruses exists for West Africa, several countries have recorded cases of DENV in the past, including Côte d'Ivoire, Senegal, Burkina Faso, and Benin (summarized in Table 1). Several reports have noted that although all four serotypes of dengue have been isolated from various West African countries in recent years, the lack of surveillance systems in many countries implies that the incidence of dengue is likely significantly underestimated. There are many obstacles that account for paucity of surveillance for dengue in Africa including the population's limited access to health care and lack of resources and laboratory capacity for serological and molecular diagnosis of the disease.
Additionally, during October and November of 2008, Mali experienced an outbreak of over 70 cases of DF with at least 2 deaths that were suspected due to DHF (ProMed-mail 2008). Although serotype analysis was not performed for most of these cases, DENV-2 was diagnosed in a French traveler returning from Mali. The authors from the Pasteur Institute who investigated the outbreak noted that in light of the recent identification of dengue in Mali, as well as the “emergence of dengue [virus] in Côte d'Ivoire, efforts are needed to better evaluate the risks of a huge dengue epidemic in western Africa.” (Tarantola et al. 2009) The serosurvey presented here was performed in 2006, 2 years before the 2008 outbreak.
Future investigations should continue to examine local mosquito populations for flaviviruses, especially in the Kayes region, the location of the 2008 dengue outbreak. In addition, a serosurvey of residents in southern Mali to estimate the impact of DENV in these regions should be conducted. This information will be important to monitor dengue transmission in Mali to identify in real-time dengue outbreaks or re-introductions. A great need exists for the transfer of dengue diagnostic technology to healthcare providers in Mali. Increased dengue diagnostic capabilities in-country will allow for determination of high-risk DENV transmission areas on a regional basis in addition to an increased ability to treat patients presenting with DF/DHF in the acute phase of the disease. Long-term goals of this study, in collaboration with the Malaria Research and Training Center in Bamako, Mali, include strengthening the local arbovirology surveillance system and assisting in the training for differential flavivirus diagnostics.
Footnotes
Disclosure Statement
No competing financial interests exist.