
Abstract
Tick-borne encephalitis virus (TBEV) is an important emerging tick-borne viral infection of humans and dogs in Europe. Currently, TBEV surveillance is virtually nonexistent in Belgium, which is considered nonendemic. A commercial enzyme-linked immunosorbent assay (ELISA) was adapted for the detection of TBEV-specific IgG-antibodies in canine sera. Serum samples of Belgian dogs were obtained from three diagnostic laboratories from Northern (n=688) and Southern Belgium (n=192). ELISA-positive and borderline samples were subjected to a TBEV rapid fluorescent focus inhibition confirmation test. One dog was confirmed TBEV seropositive. Several ELISA-positive and borderline sera underwent seroneutralization and hemagglutinin inhibition tests to rule out West Nile and Louping Ill viruses, but tested negative. The clinical history of the seropositive dog could not explain beyond doubt where and when TBEV infection was acquired. Further surveillance is necessary to determine whether this dog remains a single travel-related case or whether it represents an early warning of a possible future emergence of TBEV.
Introduction
TBE is also emerging among Europe's canine population (Leschnik et al. 2002, Beugnet and Marié 2009). Small numbers of cases were described in endemic foci of Austria, Switzerland, Germany, and Sweden (Grešíková et al. 1972a, Tipold et al. 1993, Reiner and Fischer 1998, Weissenböck et al. 1998, Kirtz et al. 2001, Bjöersdorf 2002, Csángó et al. 2004). The distribution of canine TBE is steadily expanding over Western Europe in parallel with human TBE. Consequently, a higher number of canine TBE cases are likely to be diagnosed as awareness increases in the veterinary community (Leschnik et al. 2002, Beugnet and Marié 2009). Although in 50% of dogs seroconversion occurs without any clinical signs (Leschnik et al. 2002, Klimeš et al. 2001), TBEV can cause pyrexia, lethargy, loss of appetite, and multifocal neurological signs (Bjöersdorf 2002). Most dogs develop a strong IgG immune response (Bjöersdorf 2002, Rendi-Wagner 2004), which is detectable for more than 2 months in cerebrospinal fluid to 9 months in serum (Leschnik et al. 2002). In analogy to human medicine (Holzmann 2003, Rendi-Wagner 2004), the best diagnostic tests for dogs are indirect IgG enzyme-linked immunosorbent assay (ELISA), hemagglutination inhibition (HI), seroneutralization assay (SN), rapid fluorescent focus inhibition test (RFFIT), or immunoblotting tests. SN and RFFIT tests are considered to be highly specific confirmation/reference tests (Reiner and Fischer 1998, Vene et al. 1998, Klimeš et al. 2001, Leschnik et al. 2002).
Due to the close relationship between humans and dogs, the latter are a good sentinel species for the spread and risk of TBE. Increased pet travel (Leschnik et al. 2002, Otranto and Wall 2008, Beugnet and Marié 2009) combined with more frequent contact between dogs and I. ricinus often results in higher seroprevalence rates in dogs as compared to humans (Bjöersdorff 2002, Klimeš et al. 2001). Dogs may also carry infected ticks from endemic to nonendemic areas and into close vicinity of humans (Grešíková et al. 1972b, Leschnik et al. 2002). Sentinel studies in Scandinavian dogs revealed geographical areas where TBE was more common than expected, discovered new TBEV foci, and highlighted the need for better TBE(V) surveillance (Bjöersdorff 2002, Csángó et al. 2004, Skarpaas et al. 2004).
In Belgium, TBE is still considered an exotic disease (Süss 2008, Donoso Mantke et al. 2008), and medical and veterinary TBEV surveillance is currently nonexistent (Roelandt et al. 2010). Therefore, we conducted a first serological screening of dogs in Belgium for TBEV.
Materials and Methods
Serum samples of Belgian dogs (n=880) were obtained from two diagnostic laboratories from Northern (n=688) and one from Southern (n=192) Belgium (Fig. 1). This sample size was sufficient to adapt the ELISA kit to canine sera and for the purpose of detecting a design seroprevalence of 0.35% with a confidence level of 95% (n=855), assuming 100% sensitivity and specificity in dogs. All samples were taken by local veterinary surgeons between 15/03/2009 and 22/06/2009 and submitted to the laboratories for a variety of diagnostic tests. Samples were centrifuged, and the sera were stored at 4°C at the laboratories until collected, after which they were frozen and stored at −20°C.
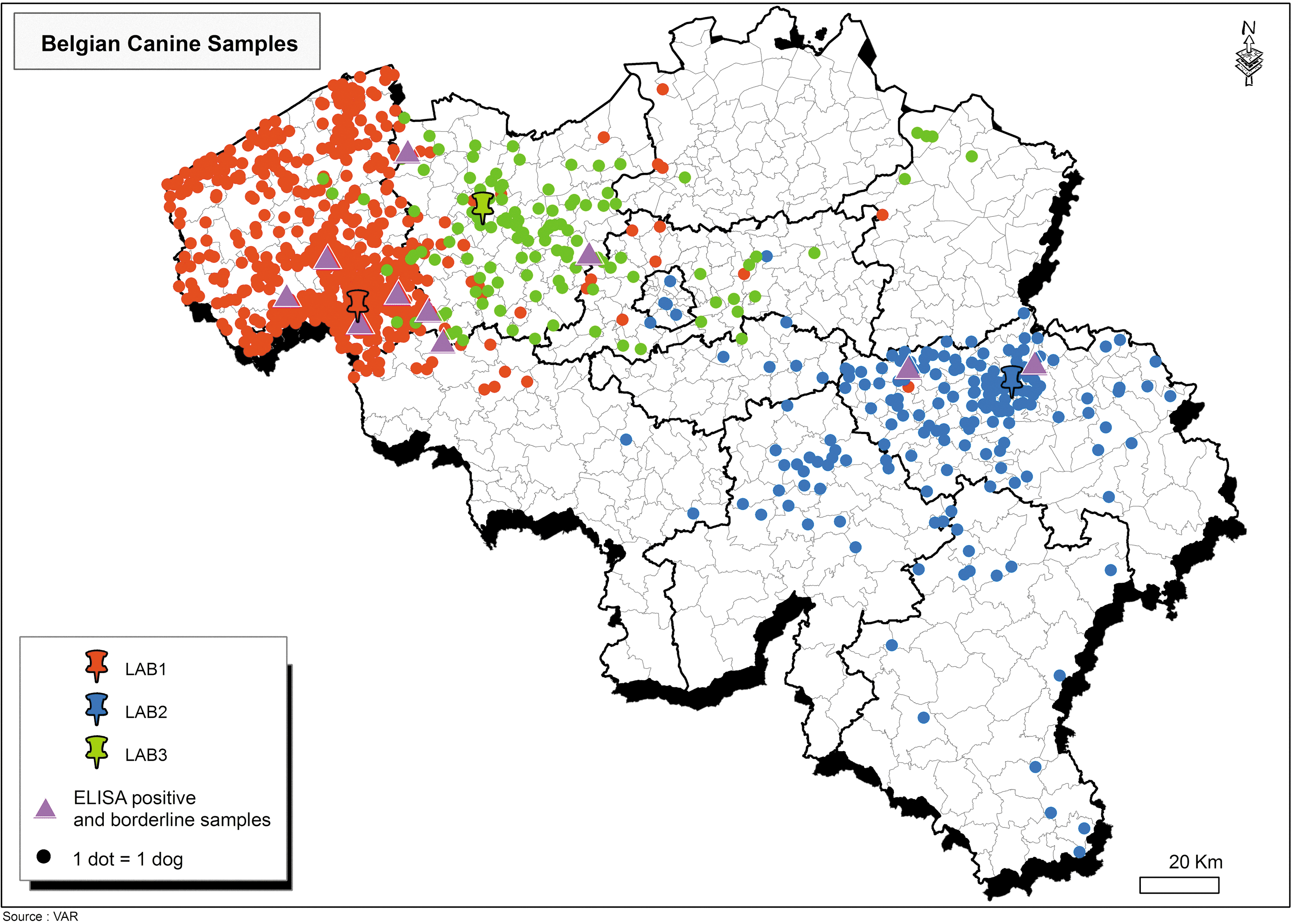
Belgian canine samples (n=880) were used in this study. Three colored pins represent the three participating laboratories. One dot represents one dog. Purple triangles represent enzyme-linked immunosorbent assay (ELISA)-positive and borderline samples.
A commercially available ELISA test kit (Immunozym FSME/TBE IgG All Species-ELISA®; Progen Biotechnik GmbH, Heidelberg, Germany) was used to detect TBEV-specific IgG antibodies in the canine sera. This noncompetitive indirect assay uses horseradish peroxidase–Protein G conjugate to detect IgG against whole TBEV. The kit can theoretically be used for TBEV testing in all species, including humans. In humans, this ELISA has a diagnostic sensitivity of 97% and analytical specificity of 99% for IgG (Progen Biotechnik GmbH 2006) and it was previously used as a TBEV screening test in foxes (Wurm et al. 2000).
The kit was adapted using a known positive canine serum from a clinical case (kindly provided by the In Vitro Labor für Veterinärmedizinische Diagnostik und Hygiene GmbH, Vienna, Austria) and a mixture of five TBEV-negative sera (SPF laboratory beagles; Janssen Pharmaceutica N.V., Beerse, Belgium) alongside human calibrator and control samples of the kit. The manufacturer's instructions were followed, sera were diluted 1:50, and optical densities were read at 450/620 nm (reference 620–690 nm). For each plate, a standard curve was generated using the five human calibrator samples. Sample concentrations were read from these curves in Vienna units per mL (VIEU/mL). Sera with <53 VIEU/mL were negative, sera with >126 VIEU/mL were positive, and those between 53 and 126 VIEU/mL were classified as borderline. Since the true diagnostic sensitivity and specificity of this kit are unknown for dogs, we lowered the cut-off by 15% compared with the kit cut-off (63→53 VIEU/mL).
A serum panel consisting of all ELISA-positive, all borderline, and a number of negative sera was sent for confirmation testing, and these sera were used as long as a sufficient volume was available. At the Swedish Institute for Infectious Disease Control (Solna, Sweden), the rapid fluorescent focus inhibition test (RFFIT) was used, essentially as described by Vene et al. (1998): a mouse monoclonal TBEV-antibody, kindly provided by M. Niedrig, followed by FITC-labeled goat-anti-mouse conjugate (Jackson ImmunoResearch, West Grove, PA) was used to visualize foci. Human control samples were used, and antibody titers were calculated as the reciprocal of the serum dilution that reduced the virus to one FFD50 (50% focus-forming dose). The lowest detectable reciprocal titer is 5. The remaining sera were then subjected to an SN test for West Nile virus (WNV) at the Veterinary and Agrochemical Research Centre (VAR, Brussels, Belgium). Briefly, serum dilutions were incubated in a 96-well plate with 100 TCID50 of WNV (IS 98 strain) for 1 h at 37°C. Chicken control sera (negative/positive) were tested at the same time. After 1 h, Vero cells were added to each well, and the plate was incubated for 3 days at 37°C with 5% CO2. After 3 days, the cytopathic effect of virus grown was read by microscopy. A HI test for Louping Ill virus (LIV) was performed at Moredun Scientific Research Institute (Penicuik, Midlothian, Scotland, United Kingdom) as described by Clarke and Casals (1958), but modified to a microtiter plate version, using ovine control samples and a cut off titer of 1:20. Samples were prepared by heat inactivation for 1 h at 65°C, and nonspecific inhibitors and goose erythrocyte agglutinins were removed by kaolin and goose erythrocyte absorption. The LIV HI test was used, because the LIV SN test was not available at the time. A retrospective descriptive epidemiological investigation was performed for confirmed TBEV ELISA- and RFFIT-seropositive dogs and consisted of telephonic contact with the owners and the veterinary practitioners, with the completion of a questionnaire.
Results
Based on the VIEU/mL cut-offs we just specified, two dog sera were found to be ELISA-positive (0.22%) and eight were borderline (0.91%). These 10 samples came from all three of the included diagnostic laboratories and from Northern and Southern Belgium (Fig. 1). Five ELISA-negative samples were included in the panel of samples for confirmation testing (n=15) and were first sent for RFFIT testing. Among these, two borderline serum samples belonging to the same dog were found positive by RFFIT at a low titer (1:5). Hereafter, these two sera are considered as one RFFIT-positive sample or dog. Nine samples giving a borderline or positive ELISA result (including the RFFIT-positive sample) and two of the negative samples were further screened for WNV antibodies by SN test at our laboratory, and all sera (n=11) were found negative for WNV antibodies. Five samples (3 borderlines, including the RFFIT seropositive sample, and two negative sera) for which sufficient serum remained, were then additionally tested by HI for LIV at Moredun Scientific Research Institute. Four of the five samples were LIV HI test negative, including that from the RFFIT-positive dog. One borderline sample tested LIV antibody positive (titer 1:160).
The TBEV (RFFIT) seropositive dog was an 8-year-old neutered female West Highland White Terrier cross, born in 2001 and living in West Flanders (Northern Belgium; Fig. 1). The owners obtained it as a 6-week-old puppy, and it had been regularly vaccinated for Canine Distemper, Canine Hepatitis, Parvovirus, Parainfluenza, Leptospirosis (DHPPiL or PiL), and Rabies. It was treated against parasites with preventive pyrantel/praziquantel (twice a year) and fipronil (once a year in June). It was never offered unpasteurized dairy products.
Though the dog was diagnosed with hypo-adrenocorticism in 2005, this condition was well controlled by standard treatment with prednisolone and fludrocortisone. The blood samples tested in this study were taken to monitor the animal's status with regard to this condition. According to the owners, this dog never showed any neurological signs or appeared ill, and apart from the Addison's disease episode there was no other disease history. There were no other pets in the household.
This dog had traveled abroad to the German Mosel region in 2002 and to the French Alsace region in 2003. On both occasions, it spent a few weeks in the area, though no forested areas were visited and no ticks were observed at the time. The dog also visited the Ardennes region in Southern Belgium on four occasions during weekend trips in autumn (November). After the end of 2004, the dog had not left the North of Belgium.
At home, this dog has access to the back garden and to the local forested countryside in West Flanders. In the summer of 2008, before the positive blood sample was taken, the owners removed a small red tick from the dog, at home in the garden. Apart from a small crust at the attachment site, the animal remained asymptomatic after the tick bite. Another tick was observed during the summer of 2009, after the diagnostic blood samples included in our study had been taken. None of the family members in this household ever showed clinical signs compatible with TBE.
Discussion
Our sample of the Belgian canine population has to be considered as a convenience sample. The sera came from all provinces in Northern and Southern Belgium, though they were mainly obtained from four of the ten provinces (Fig. 1). Further, the serum samples were taken either to diagnose illness, to monitor treatment or as preanesthetic screening. Therefore, they may not necessarily be representative of the entire canine population in Belgium. Nonetheless, the available sample was of sufficient size to adapt the ELISA kit and to detect a design seroprevalence of 0.35% with a confidence level of 95% (n=855 needed).
In the case of TBEV testing, all samples found positive or borderline by ELISA need to be confirmed with a reference test such as RFFIT or SN, as nonspecific reactions as well as cross-reactions of TBEV antibodies with other flavivirus antibodies are well known. The same applies for LIV and our results confirm this, as several false positive samples were observed for TBEV and likely also one for LIV, despite adequate sample preparation. It was also clear that the canine cut-off of this ELISA kit needs further evaluation, to improve sensitivity and to avoid false negatives.
In humans, cross reactions often occur with Yellow Fever virus, Dengue virus, and WNV antibodies (Holzmann 2003). A cross-reaction between anti-TBEV and anti-WNV antibodies was observed in a dog in the Czech Republic (Klimeš et al. 2001). Therefore, we included WNV as a differential diagnosis for ELISA-positive/borderline but RFFIT-negative samples.
TBEV is phylogenetically very closely related to LIV, and both viruses share I. ricinus as vector. LIV can cause sheep or goat encephalitis and has so far been reported in Scotland, Wales, England, Ireland, Norway, Denmark, Spain, Greece, Turkey, and Bulgaria (Gritsun et al. 2003, Grard et al. 2007, Dobler 2010). Although few cases have been reported, LIV can occasionally cause encephalitis much similar to TBE in dogs and humans (Dobler 2010). The dog that tested positive for LIV HI and negative for TBEV RFFIT and WNV SN was lost to follow-up and since LIV SN was not available, a final conclusion with regard to LIV could not be made. The travel and vaccination history of this animal might have shed some light on the high titre obtained despite the standard sample preparation just described.
Other flaviviruses than the ones we considered are either not known to infect dogs, or only occur outside Europe, or depend on maintenance hosts and/or vectors currently not present in Belgium. It concerns viruses of the TBEV-serocomplex (i.e., the mammalian group of tick-borne flaviviruses: Langat virus, Powassan virus, Kyasanur forest disease virus, Omsk haemorrhagic fever virus, Royal Farm virus, Karshi virus, Gadgets Gully virus and Alkhumra virus), as well as Dengue virus and Yellow fever virus (Gritsun et al. 2003, Grard et al. 2007, Gubler et al. 2007, Dobler 2010). These flaviviruses were considered less relevant in our differential list and were, therefore, not included in the differentiation test panel.
The TBEV seropositive dog's history revealed international travel and tick exposure, though these factors did not seem to occur simultaneously. The specific areas visited in Germany and France are not currently listed as endemic areas, though in both cases endemic areas are nearby (RKI 2003, ISW-TBE 2009) and the visits took place during the tick season (Heinz 2008). Belgium is currently considered to be nonendemic for TBEV (Donoso Mantke et al. 2008), and since the visits to Southern Belgium occurred at the very end of the tick season (November) (Heinz 2008), it seems less likely that the infection would have occurred there. Since the dog had never been offered unpasteurized food items, the oral route of infection can be excluded.
According to the history of this dog, two possible sources of infection with TBEV can be considered. The dog could have become infected by an unnoticed tick during its travels in Europe, 5 to 7 years ago. Alternatively, it may have been infected from 2005 onward, much closer to or even at home in West Flanders, where ticks were actually observed on the animal during the last two summers. The fipronil administration she received once a year in June is severely inadequate to ensure continuous tick protection throughout the whole tick season.
According to the available literature, “TBEV seroneutralizing antibodies provide a lifelong protection” in both humans (Mickiené et al. 2002) and dogs (Bjöersdorf 2002) and since the dog had traveled near to endemic areas, a travel-related infection seems plausible. However, according to Leschnik et al. (2002), canine anti-TBEV-IgG are detectable in serum until “up to 9 months postinfection,” so it is possible that we detected an ELISA-borderline and RFFIT-positive animal that was recently infected (Summer 2008) at home in Belgium. In both scenarios, further surveillance is strongly recommended as an early warning system for possible future emergence or incursions of TBEV in Belgium.
In view of these findings, it would be prudent to further validate and standardize an ELISA test for estimating prevalence of infection or exposure to TBEV in several species. Such a test would be needed to enable a data-based risk analysis for TBE in Belgium. Continued serological screening of TBEV in dogs and other domestic and wild sentinel species in all Belgian provinces is, therefore, advisable to gain more insight into the current situation. Such targeted veterinary serological screening of sentinel animals could contribute in a cost-effective way to a continuous public health epidemiosurveillance program for TBE(V) (Roelandt et al. 2010), in parallel with ongoing Belgian initiatives to improve epidemiosurveillance of vector-borne emerging threats to public health (Bottieau et al. 2009, Lizroth and Quoilin 2009).
Conclusion
During the first serological screening for TBEV in Belgian sentinel dogs, a TBEV-seropositive dog was discovered. A commercial ELISA test was adapted for use in dogs and was followed by a confirmation RFFIT test. Belgium is traditionally considered as nonendemic for this emerging vector-borne flavivirus. The seropositive dog had traveled to areas near to known endemic areas in 2001–2004. However, ticks were only observed on the dog in the period from 2005 onward, when it stayed in at home in Northern Belgium. The animal has been asymptomatic throughout. Neither a travel-related infection nor the emergence of an autochthonous endemic focus can be excluded with certainty. Therefore, it is recommended to continue the screening of sentinel animals in Belgium to determine whether this dog is an isolated “case” in veterinary travel medicine, or whether it represents the proverbial “tip of the iceberg.”
Footnotes
Acknowledgments
This work was funded by a grant from the Belgian Federal Government, Department of Public Health, Safety of the Food Chain and Environment, as a part of the Wildsurv Project (contract RT 07/5). The authors thank the participating Belgian diagnostic laboratories (Medisch Labo Bruyland, Mediclab Ghent, Laboratoire Dr. Jean Collard Liège) for supplying canine serum samples and the owners of the seropositive dog for their cooperation in the epidemiological investigation. We are most grateful to the In Vitro Labor für Veterinärmedizinische Diagnostik und Hygiene GmbH (Austria) and to Sandra De Jonghe at Janssen Pharmaceutica N.V. (Belgium) for supplying us with the necessary positive and negative control samples, as well as to Kim Willoughby, who organized the LIV HI test at Moredun Scientific Research Institute (Scotland, UK). Special thanks also go to Pieter De Bleser at the VIB, Ghent University (Belgium), who assisted in analyzing the standard curve equations, to the laboratory technicians at the VAR (Belgium), to Flavien Riocreux (VAR) who created the artwork for this article, to the Department of Virology of the Swedish Institute for Infectious Disease Control (Sweden), and to Moredun Scientific Research Institute (Scotland, UK) for the skilful diagnostic testing.
Disclosure Statement
No competing financial interests exist.