
Abstract
Background:
African tick-bite fever (ATBF) is frequently diagnosed in The Netherlands in travelers returning from South Africa. It is caused by Rickettsia africae and diagnosis is based on travel history and clinical presentation and usually confirmed by detecting serum antibodies against rickettsiae of the spotted fever group. However, these typically occur late in the course of the disease, and a mild clinical course or early antibiotic treatment can diminish antibody production.
Methods and Results:
Four travelers presented with (sub)febrile temperatures and eschar(s), several days after returning from South Africa. R. africae DNA was amplified and sequenced from skin biopsies of the eschars of all patients. Initial immunofluorescence assays yielded no immunoglobulin M (IgM)/IgG antibodies directed against spotted fever group rickettsiae; however, serology in the convalescent phase—several weeks after the patients had fully recovered—was positive.
Conclusions:
ATBF should be considered in travelers returning from South Africa to The Netherlands with febrile illness and (multiple) skin lesions. The diagnosis can be confirmed by (paired) serology; however, polymerase chain reaction and sequencing on skin biopsies could be a (faster and more accurate) confirmatory test. Advantages of molecular methods over serology are species identification and high sensitivity early in the course of the disease.
Introduction
R. africae is the second most frequent cause of systemic febrile illness among travelers returning from sub-Saharan Africa (Freedman et al. 2006). Rickettsia conorii is also prevalent in Africa and has a comparable, but more severe, clinical presentation compared with ATBF. The incidence, however, is lower and infection usually presents with a single eschar (Raoult et al. 1986). Further, the differential diagnosis of multiple eschars comprises serious, but rare, diseases in returning travelers, such as other rickettsial infections or cutaneous anthrax, warranting swift and accurate diagnostic tests. More commonly, insect/spider/arthropod bites or cutaneous infections with staphylococci or streptococci can mimic eschars.
Although ATBF is mainly a clinical diagnosis, it is usually confirmed by detecting antibodies in serum against rickettsiae of the spotted fever group. However, these typically occur late in the course of the disease and early antibiotic treatment or a mild course of the disease can diminish antibody production. In addition, in many countries, including The Netherlands, differentiation between R. conorii and R. africae infection by serology is not possible. The confirmation of the diagnosis of ATBF relies on detection of cross-reactive antibodies against other spotted fever group rickettsiae (e.g., R. conorii and R. rickettsii). In the outpatient clinic of the department of Tropical Medicine of the Academic Medical Center (AMC), from 2008 until 2010, 19 patients presented with fever and one eschar, and 6 patients presented with fever and multiple eschars. Thirteen of these patients had detectable antibodies against spotted fever group rickettsiae (unpublished data). Twenty-one patients had visited South Africa, and four had visited other countries in sub-Saharan Africa. Based on geographical and epidemiological considerations, these patients were probably infected with R. africae. This number is an underestimation, because (telephonic) consultations by colleagues or general practitioners were not recorded. Data collected via Geosentinel, of which the AMC is a surveillance center, showed that 197 patients returned from South Africa to 41 Geosentinel sites with a spotted fever group rickettsiosis from 1998 to 2006 (Jensenius et al. 2009).
In contrast to serology, polymerase chain reaction (PCR) is a rapid, sensitive and specific test to diagnose R. africae infection (Fournier and Raoult 2004; Fenollar and Raoult 2007). In several case reports or series, PCRs of eschar biopsies in patients with clinically confirmed ATBF were all positive (Bouvresse et al. 2008, Oteo et al. 2004, Tsai et al. 2009). In line with these observations, in a study by Raoult et al. (2001), a suicide PCR—in which primers are used only once to avoid contamination—on skin biopsies demonstrated 100% sensitivity; all of 15 patients with serologically confirmed R. africae infections were also positive with PCR. Fournier and Raoult (2004) described lower sensitivities for both regular and suicide PCRs, for example, in 25 of 34 clinically confirmed cases of ATBF (73.5%), DNA of R. africae was amplified using a suicide PCR. It should be noted that several patients were already taking antibiotics. Both regular and suicide PCR were more sensitive than culture.
We here describe four patients returning from South Africa with fever and skin lesions in which we confirmed the diagnosis of ATBF, that is, R. africae infection, by PCR and sequencing on DNA obtained from skin biopsies of the eschars, a technique, to the best of our knowledge, not routinely applied.
Patients
Patient 1
A 66-year-old man visited our travel clinic at 6 days after returning from a 15-day journey to South Africa. His medical history revealed benign prostate hypertrophy. His vaccination status was adequate. He had not been taking malaria prophylaxis and had not been in direct contact with freshwater bodies. He presented with headache, fever (38°C–39°C), and multiple skin lesions. Symptoms began at 1 week before presentation, which was 1 day after a visit to a private game park nearby Kruger National Park. He had walked through high grass surrounding a small body of water. He had not noticed insect bites or any ticks. On physical examination, six eschars on his legs, chest, and back were found (Fig. 1a). Further, a discrete spotted exanthema was observed on his trunk. His body temperature was 37.6°C aurally (after taking antipyretics). Laboratory investigation revealed a white blood cell count in the low normal range (leukocytes: 4.7×109 cells/L), normal platelet count (thrombocytes: 175×109 cells/L), a slightly elevated C-reactive protein level (15.2 mg/L), and normal liver and renal function. Thus, our patient was suspected of ATBF and treatment with doxycycline 100 mg twice daily orally for 1 week was initiated. To confirm our diagnosis, we took biopsies from the eschars for histological examination and PCR and performed serology (upon presentation and after convalescence). PCR was also performed on blood.
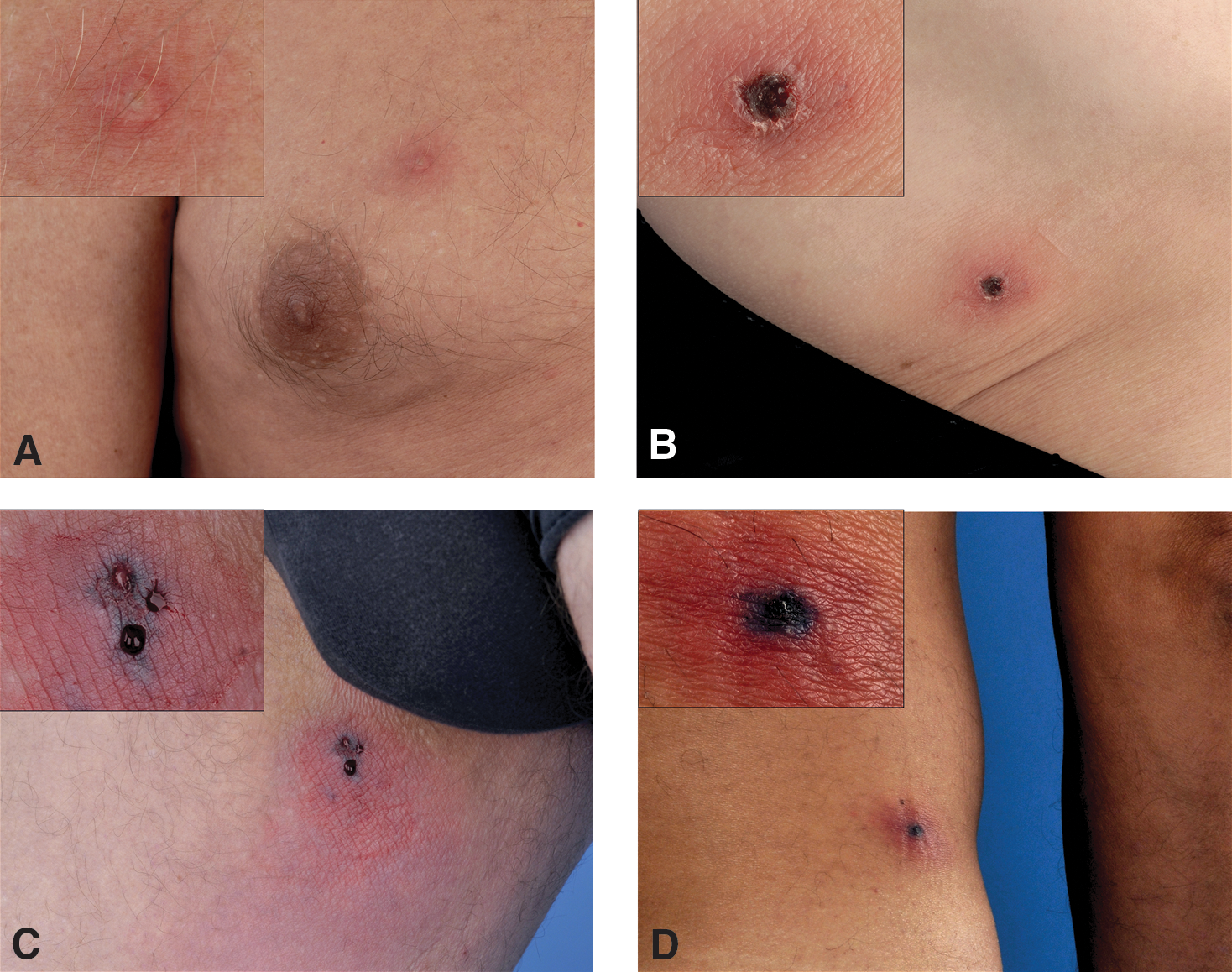
Eschars of all four patients.
The first patient has been described in detail. The other three patients had similar presentations (Table 1 and Fig. 1a–d).
Rickettsiosis diagnosed and treated elsewhere.
On presentation.
Materials and Methods
Skin biopsies and histological examination
Two-millimeter punch biopsies were taken from the “tache noir” of the eschars after disinfection and local injection of 2% lidocaine. After fixation in buffered formalin and paraffin embedding, 4-μm-thick sections were stained with hematoxylin and eosin for histomorphological analysis and with Gram stain, Grocott's methenamine silver stain, periodic acid Schiff-diastase, and Ziehl-Nielsen's stain, respectively, for detection of microorganisms. In addition, transmission electron microscopy (EM) was performed on glutaraldehyde-fixed skin biopsies.
Serology
Blood was drawn upon presentation of patients (acute phase) and several weeks after presentation (convalescent phase). In both samples, immunoglobulin G (IgG) and IgM antibodies against R. conorii and R. rickettsii (spotted fever group) and Rickettsia typhi (typhus group) were tested as part of the routine diagnostic setting (Erasmus Medical Center, Rotterdam), using a commercially available immunofluorescence assay (IFA) (Focus Diagnostics, Inc., Cypress, CA). Routine diagnostic testing does not include testing for R. africae-specific antibodies. Tests were performed according to the manufacturer's instructions. All samples were screened with dilutions of 1:64 and 1:256. Positive samples were titrated to end-point fluorescence in twofold dilutions. The positive cutoff value for IgG and IgM was set at ≥1:64. As there was no specific R. africae IFA available, serologic confirmation of the diagnosis of ATBF relied on the detection of antibodies against R. conorii (or R. rickettsii), as there is cross-reactivity among spotted fever group rickettsiae, to which also R. africae belongs. Cross-adsorption assays were not performed.
PCR and sequencing
The primers used for PCR have been previously described (Christova et al. 2003, Tijsse-Klasen et al. 2010). The 16S rRNA gene of Rickettsia species (360 bp) was amplified using the HotStarTaq master mix (Qiagen, Hilden, Germany) under the following conditions: 15 min at 94°C; then cycles of 20 s at 94°C, 30 s at 72°C, and 30 s at 72°C, lowering the annealing temperature by 1°C in each cycle until reaching 62°C; and then 40 cycles at this annealing temperature, followed by a final elongation step for 7 min at 72°C. All samples were analyzed on agarose gels. Positive samples were subjected to PCR of an independent marker. The citrate synthase gene (glt), 850 bp in length, was amplified using primers CS409d and Rp1258n (Roux et al. 1997), using HotStarTaq master mix under the following conditions: 15 min at 95°C, then 40 cycles of 30 s at 94°C, 30 s at 54°C, and 55 s at 72°C, followed by a final elongation step for 7 min at 72°C. PCR products were sequenced by dideoxy-dye termination sequencing of both strands at the RIVM sequencing facilities using the ABI 3100 automated sequencer (Applied Biosystems, Foster City, CA) and compared with sequences in GenBank (
Results
Histological examination of skin biopsies showed extensive superficial ulceration and angiocentric inflammatory infiltrates in the underlying dermis and subcutis, which were composed of mononuclear cells, granulocytes, and large amounts of nuclear fragments. Affected vessels showed fibrinoid necrosis of the vessel wall, endothelial swelling, and focal thrombus formation, representing a severe type of leukocytoclastic vasculitis (Fig. 2a). All histochemical staining tests for bacteria were negative. With the use of transmission EM, no viable bacteria could be detected. However, many macrophages and endothelial cells contained large amounts of myelin figures (condensed concentric lamellar remnants of lipoprotein layers), which can be interpreted as degenerate or necrotic cells from the lesion or as remnants of bacteria (Fig. 2b). No viable microorganisms were visualized, presumably because biopsies were taken after treatment had been initiated.

Histological examination.
Two to 3 weeks after initiation of treatment, several days after the patients had completely recovered, serologic tests on acute phase sera proved to be negative for spotted fever group rickettsiae. In convalescent sera, antibodies against spotted fever rickettsiae (i.e., R. conorii) were detected in all four (4/4) patients (Table 2).
Positive serologic results are indicated in boldface.
Sequencing of 16S rRNA DNA was compared with R. africae sequences present in GenBank (L36098 and CP001612). Sequencing of gltA was compared with the gltA gene of R. africae from GenBank (CP001612).
PCR, polymerase chain reaction.
In skin biopsies of all patients, only several days after initiation of treatment, the 16S rRNA gene of the Rickettsia species was detected by amplification of the 16S rRNA gene using a PCR with generic rickettsia-specific primers. After removal of the primer sites, sequences were obtained from all samples over a length of at least 339 bp and were 100% homologous to the R. africae sequences present in GenBank (L36098 and CP001612). In addition, the presence of R. africae was confirmed by amplification and sequencing of gltA in three of four patients. After removal of primer sites, high-quality sequences were between 688 and 727 bp in length and showed 100% similarity to the gltA gene of R. africae from GenBank (CP001612). Neither the 16S rRNA gene nor the gltA gene was detected in blood (cases 1 and 4). In Table 2, the diagnostic results of all four patients are presented.
Discussion
We describe four travelers returning from South Africa who were found to have ATBF with (multiple) eschars. In all patients, the presence of R. africae was readily demonstrated by PCR and sequencing, a technique that it is not widely used, especially not in The Netherlands, for confirmation of the diagnosis. These patients were treated with doxycycline and promptly recovered. One patient was also presumptively treated with flucloxacillin, as the eschar had an atypical presentation and Staphylococcus aureus infection was suspected.
People who travel the countryside in areas where R. africae is endemic and have contact with ticks, e.g., hunters such as our second patient (Table 1), are at risk of acquiring ATBF (Raoult et al. 2001, Jensenius et al. 2003). Amblyomma ticks mainly feed on cattle and wild ungulates (Norval 1979), but also on humans. As opposed to the Rhipicephalus species, the vector of R. conorii, Amblyomma ticks, aggressively seek their host and respond to stimuli such as CO2 concentration, NH3, and body temperature (Norval et al. 1989). This may explain the multiple eschars and the appearance of ATBF in groups of returning travelers, as demonstrated by our second case, in which two of the patients' travel companions, all were hunters, also had symptoms consistent with ATBF (Table 1).
ATBF is usually confirmed by detecting antibodies in serum against rickettsiae of the spotted fever group with IFA using glass slides. Other serologic tests include latex agglutination, enzyme immunoassay (ELISA), western blot, or complement fixation. Antibodies against R. africae typically occur late in the course of the disease (Fournier et al. 2002). Also, early antibiotic treatment or a mild course of the disease can diminish antibody production. Indeed, previous studies have described ATBF patients of which a fairly large proportion was PCR positive, but no antibodies against rickettsiae could be detected (Raoult et al. 2001, Stephany et al. 2009, Althaus et al. 2010). In all our cases (4/4), initial serologic assays, performed early after onset of symptoms, were negative. In convalescent sera, antibodies against spotted fever group rickettsiae (i.e., R. conorii) were detected in all (4/4) patients. In contrast, a preliminary analysis of serology performed in the Erasmus Medical Center on sera of approximately 150 travelers returning from South Africa and clinically suspected of having contracted a rickettsiosis (and thus most likely ATBF) showed that only approximately one third could be confirmed by serology (data not shown).
In The Netherlands, serologic tests specific for R. africae are not available and cross-adsorption tests, previously described as highly specific, are not routinely used (Raoult et al. 2001). The combination of a clinical presentation with multiple eschars and positive R. conorii serology is considered sufficient for diagnosis. Thus, R. conorii infections with multiple eschars, R. africae infections with a single eschar (as our third patient), or R. africae infections with multiple eschars but an absent antibody response may be missed or remain unconfirmed. The therapeutical consequences of exact identification of the rickettsial species might be limited. However, there have been reports of R. conorii associated with severe complications such as meningo-encephalitis, septic shock, and multiorgan failure and mortality can be as high as 20% (DeMeester et al. 2010). Generally, R. africae has been described as a benign disease with a quick recovery following tetracycline therapy (Raoult et al. 2001), although Roch and collaborators (2008) have described a severe clinical course and slow recovery of ATBF in elderly patients. Additionally, from an epidemiological point of view it might be useful to identify the exact rickettsial species by PCR.
A major advantage of PCR and sequencing over serology is that it can be applied to detect microorganisms in skin biopsies in the acute phase, allowing for a quick diagnosis, differentiation between all Rickettsia species, and then additional testing to confirm or exclude differential diagnoses or additional therapy unnecessary. The PCR and sequencing techniques described here allowed for a diagnosis within several days, whereas novel molecular diagnostics, such as multiplex real time PCR, could result in even faster diagnosis or confirmation.
PCR assays on blood samples may be considered in patients without skin lesions returning from an area where ATBF is endemic. However, sensitivity and specificity are much lower compared with PCR on eschar biopsies (Raoult et al. 2001, Jensenius et al. 2004). Finally, culture of skin biopsies can also be used to identify rickettsia but sensitivity is low (Raoult et al. 2001) and should only be performed in specialized laboratories routinely working with intracellular bacteria (Norval et al. 1989).
In conclusion, we here demonstrate molecular evidence of R. africae infection causing ATBF with (multiple) eschars in four patients returning from South Africa to The Netherlands. PCR on skin biopsies and subsequent sequencing is only minimally invasive and should be considered as an important alternative or additional diagnostic method for ATBF, leading to quick diagnosis, initiation of treatment, and identification of the rickettsial species.
Footnotes
Acknowledgments
The authors express thanks to M.A. van den Bergh Weerman of the Department of Pathology in the Academic Medical Center, Amsterdam, for assistance with transmission EM and to Dr. H. Zaaijer, virologist of the Academic Medical Center, Amsterdam, for providing serological data obtained in the AMC. Also, the authors thank Dr. A.M. Nijhof of the Institute for Parasitology and Tropical Veterinary Medicine, Freie Universität Berlin, Germany, for his valuable comments on this manuscript.
Disclosure Statement
The authors declare that they have no conflict of interest.