
Abstract
Clinical cases of hantavirus pulmonary syndrome (HPS) can be challenging to differentiate from other acute respiratory diseases, which can lead to delays in diagnosis, treatment, and disease reporting. Rapid onset of severe disease occurs, at times before diagnostic test results are available. This study's objective was to examine the clinical characteristics of patients that would indicate HPS to aid in detection and reporting. Test results of blood samples from U.S. patients suspected of having HPS submitted to the Centers for Disease Control and Prevention from 1998–2010 were reviewed. Patient information collected by case report forms was compared between HPS-confirmed and test-negative patients. Diagnostic sensitivity, specificity, predictive values, and likelihood ratios were calculated for individual clinical findings and combinations of variables. Of 567 patients included, 36% were HPS-confirmed. Thrombocytopenia, chest x-rays with suggestive signs, and receiving supplemental oxygenation were highly sensitive (>95%), while elevated hematocrit was highly specific (83%) in detecting HPS. Combinations that maximized sensitivity required the presence of thrombocytopenia. Using a national sample of suspect patients, we found that thrombocytopenia was a highly sensitive indicator of HPS and should be included in surveillance definitions for suspected HPS. Using a sensitive suspect case definition to identify potential HPS patients that are confirmed by highly specific diagnostic testing will ensure accurate reporting of this disease.
Introduction
From a clinical standpoint, HPS diagnosis and care presents several difficulties. A non-specific febrile prodrome that includes headache, myalgia, and gastrointestinal symptoms usually precedes the onset of respiratory symptoms (Young et al. 1998), and resembles several other viral illnesses. Rapid progression of respiratory distress, shock, and death often occur within 24 h of hospitalization, before diagnostic results are available. Patients frequently require respiratory support such as supplemental oxygenation or mechanical ventilation, often necessitating transport to a tertiary care facility (Duchin et al. 1994). Because many patients are otherwise healthy before developing HPS, they may not be expected to have such severe disease and may not receive aggressive initial treatment. HPS is treated with supportive therapy, as there is no specific treatment (Mertz et al. 2006). The cardiac index can be depressed in some patients and contributes to disease severity (Hallin et al. 1996); using inotropic agents and extracorporeal membrane oxygenation has been suggested when cardiac values indicate depressed function (Dietl 2008).
Since 1995, laboratory-confirmed cases of HPS are nationally notifiable (Khan et al. 1996). A suspect case of HPS is defined by the Centers for Disease Control and Prevention (CDC) and Council of State and Territorial Epidemiologists (CSTE) as a previously healthy person with an acute febrile respiratory illness, characterized by bilateral diffuse interstitial edema that may radiographically resemble acute respiratory distress syndrome (ARDS), with respiratory compromise requiring supplemental oxygen, and/or an autopsy examination demonstrating noncardiogenic pulmonary edema without an identifiable cause. A confirmed case requires detection of hantavirus-specific IgM, a rising IgG titer, detection of a hantavirus-specific ribonucleic acid sequence by polymerase chain reaction in clinical specimens, or detection of antigen by immunohistochemistry (MacNeil et al. 2011).
Surveillance efforts benefit from rapid identification and reporting of a patient with HPS. When a patient is confirmed, local health departments often carry out environmental investigations to identify where exposure to infected rodents may have occurred, and contact other individuals who may have had a similar exposure. Although rare in North America, household clusters of HPS have been reported previously (Ramos et al. 2000; Webster et al. 2007), and further infections can be prevented through education of household members on safe rodent handling, disinfection, and exclusion methods (Mills et al. 2002). When surveillance identifies increased incidences of HPS, officials at the local, state, or national levels can deploy educational messages notifying at-risk individuals in the area and encouraging proper personal protection (Centers for Disease Control and Prevention 1999, 2006).
Because of the concerns that arise due to the rapid onset of severe disease and difficulty in distinguishing HPS from other viral respiratory illnesses, there is a need to identify potential HPS patients. With the assumption that an accurate suspect case definition will both assist clinicians in determining the likelihood of an HPS diagnosis, and improve reporting to public health authorities, the objective of this study was to examine the clinical characteristics of HPS test-positive and test-negative patients in order to evaluate potential suspect case definitions that would aid in detection and reporting of HPS cases in the United States.
Materials and Methods
Patients who had diagnostic samples submitted to the Viral Special Pathogens Branch, CDC, for HPS testing from June 10, 1998 to May 27, 2010 were evaluated. Clinical and epidemiologic data on all patients were collected using a standard case report form (Centers for Disease Control and Prevention, Hantavirus Pulmonary Syndrome Case Report Form:
Serum samples were tested for HPS using IgG enzyme-linked immunosorbent assay (ELISA) and IgM capture ELISA as previously described (Ksiazek et al. 1999; Bostik et al. 2000). Briefly, the antigen used for IgG testing was an E. coli-expressed complete SNV nucleoprotein, while IgM antigen was a whole-virus preparation of SNV from cell culture. Sera were tested against SNV antigen and control antigen using fourfold dilutions of sera, from 1:100 to 1:6400. A sample was positive with a titer ≥1:400, and adjusted sum OD ≥0.91 for IgG or ≥0.45 for IgM. Patients were considered confirmed HPS cases as defined by CDC/CSTE criteria.
All diagnostic test results and case report forms were stored in a Microsoft Access database, and calculations were performed with statistical analysis software (SAS; SAS Institute, Cary, NC). Test results were compared with case report information on the basis of symptoms, clinical findings, patient demographics, U.S. region of residence, and illness outcome. Simple frequencies, risk ratios with 95% confidence intervals (CI), diagnostic sensitivity and specificity, and positive- and negative-predictive values (PPV and NPV) were determined for the following: fever, elevated white blood cell count, thrombocytopenia, elevated hematocrit, elevated serum creatinine, chest x-rays with unexplained bilateral interstitial infiltrates, and receiving supplemental oxygenation. Additionally, the positive-likelihood ratio (PLR), calculated as sensitivity/(1 – specificity), and negative-likelihood ratio (NLR), calculated as (1 – sensitivity)/specificity (Deeks et al. 2004), were calculated. For ease of comparison and interpretation, NLR−1 was reported. Eighteen combinations of the above single variables were evaluated as potential surveillance case definitions, using the same calculations.
Results
Single variables
Among 567 patients who met the inclusion criteria, 206 (36%) were confirmed as having HPS, and 361 were negative. There was no association between age, sex, race, or ethnicity, and ELISA results (results not shown). Fever, thrombocytopenia, elevated hematocrit, chest x-rays suggestive of HPS, and receiving supplemental oxygen were significantly associated with a positive test result. HPS was also more likely in patients who died or who resided in states west of the Mississippi River (Table 1).
95% confidence interval of the risk ratio.
>38.3°C.
<150,000/mm3.
>10,800/mm3.
Western states were classified relative to the Mississippi River.
For single variables, the presence of thrombocytopenia and supplemental oxygenation were the most sensitive indicators of HPS, each occurring in 97% of positive cases. Positive chest x-ray findings had a similarly high sensitivity of 96%, while fever occurred in 87% of HPS-confirmed patients (Fig. 1). Elevated hematocrit had the highest specificity at 83%, while all other variables had specificities ≤50% (Fig. 2). Elevated hematocrit had the highest PPV of 70%, followed by thrombocytopenia at 53% (Table 2). The clinical finding with the highest NPV was thrombocytopenia at 97%, while chest x-rays suggestive of HPS (see definition in materials and methods section) had a NPV of 88%, supplemental oxygenation was 87%, and elevated hematocrit was 83% (Table 2).
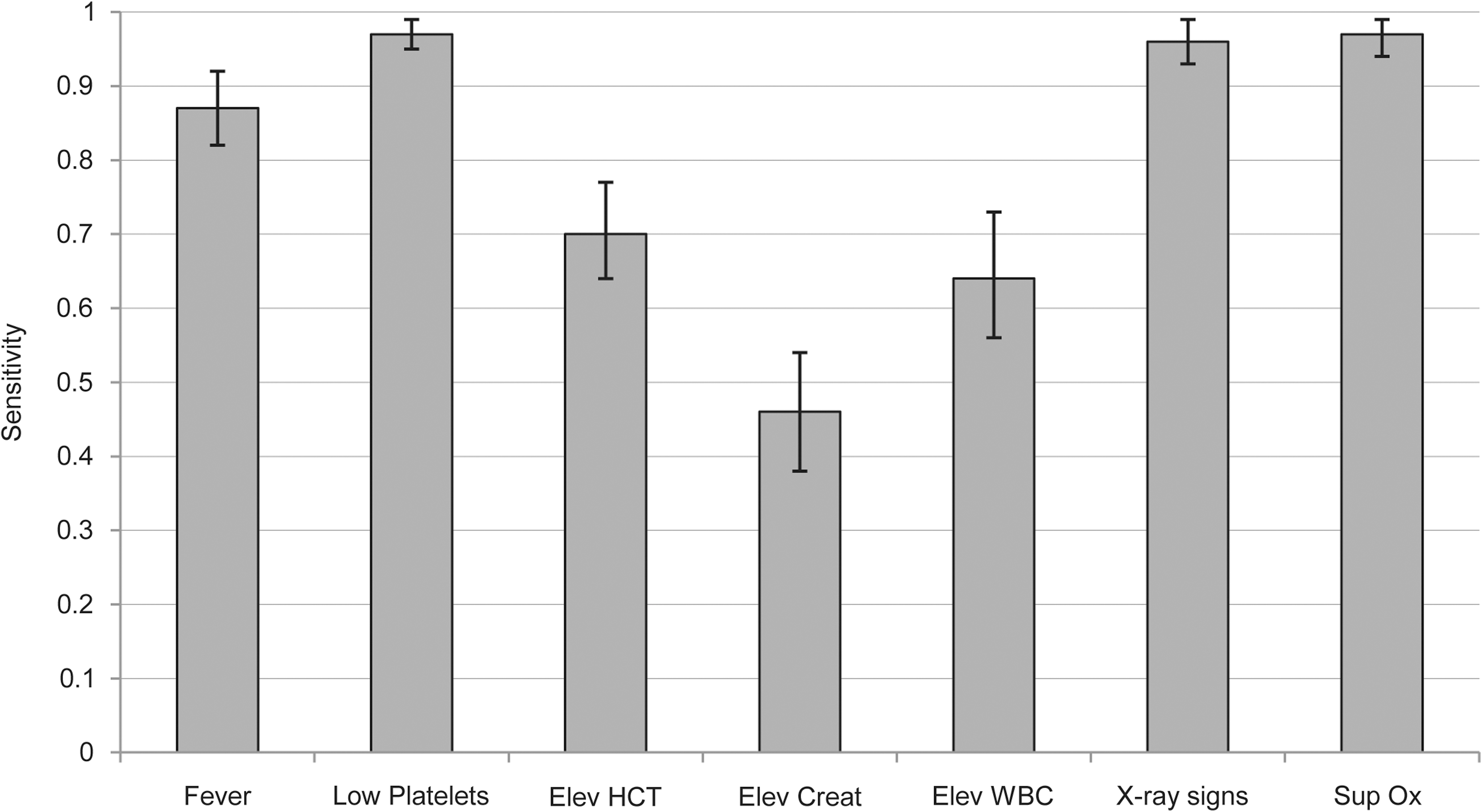
Calculated diagnostic sensitivity and 95% confidence intervals (error bars) of clinical findings indicating HPS. See Table 1 for reference ranges (Elev, elevated; HCT, hematocrit; Creat, creatinine; WBC, white blood cells; Sup Ox, supplemental oxygen; HPS, hantavirus pulmonary syndrome).
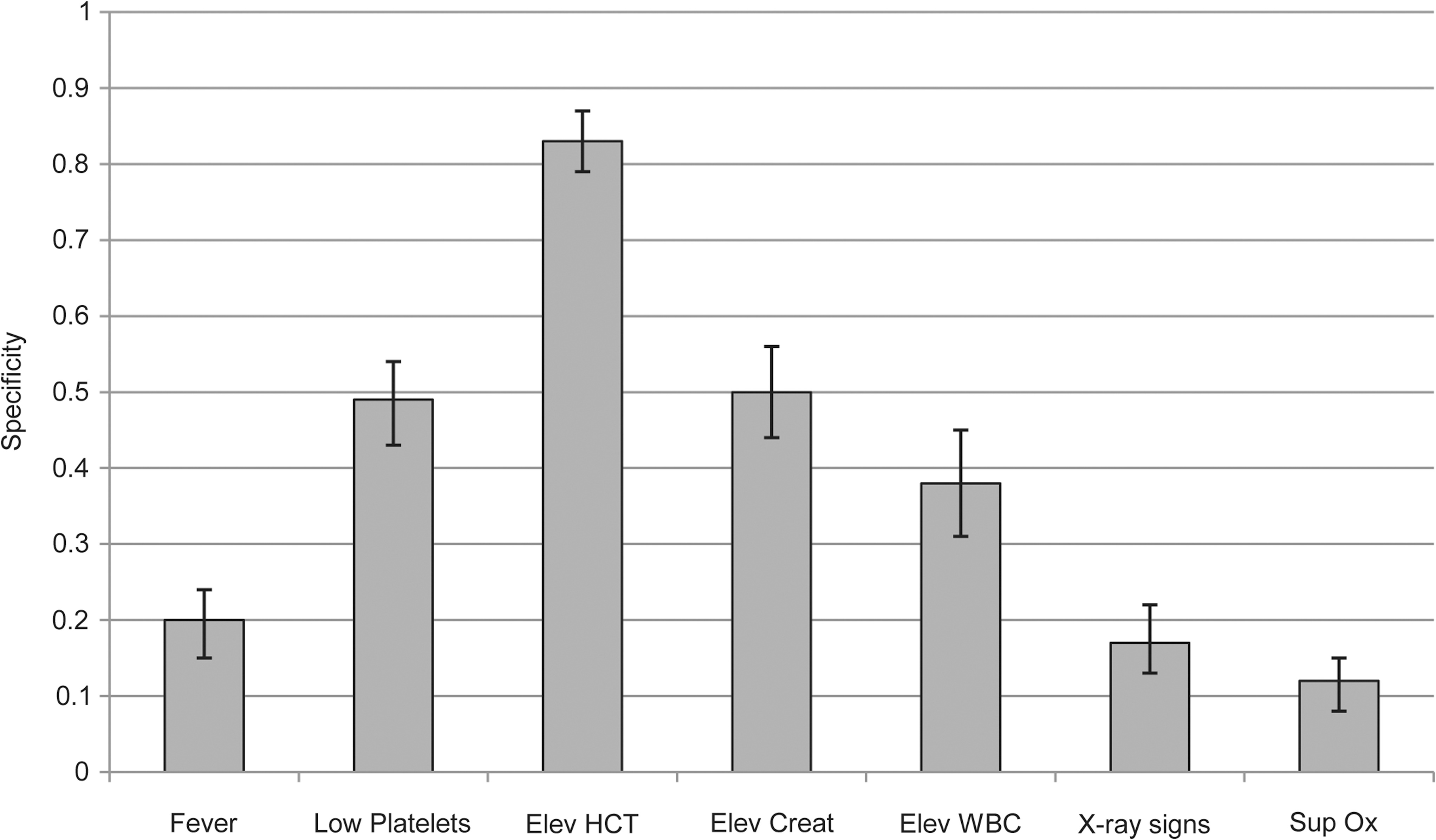
Calculated diagnostic specificity and 95% confidence intervals (error bars) of clinical findings indicating HPS. See Table 1 for reference ranges (Elev, elevated; HCT, hematocrit; Creat, creatinine; WBC, white blood cells; Sup Ox, supplemental oxygen; HPS, hantavirus pulmonary syndrome).
For PLR and NLR−1 calculations, please see the materials and methods section.
Elevated hematocrit had the highest PLR of 4.1, indicating a small increase in likelihood of HPS, while thrombocytopenia had a value of 1.9 (Table 2). All other parameters had likelihood ratios close to the null value of 1. Thrombocytopenia had a NLR−1 of 16.3, indicating a large decrease in the likelihood of HPS if this finding was absent, while elevated hematocrit was 2.8, and positive chest x-ray was 4.3.
Combinations of clinical findings
Eighteen combinations of six clinical findings (fever, thrombocytopenia, elevated hematocrit, elevated white blood cells, chest x-rays suggestive of HPS, or receiving supplemental oxygenation) were evaluated as potential case definitions (Table 3). Because elevated serum creatinine had no association with HPS-confirmed patients, it was not included in the combinations. Combination A included the presence of fever and thrombocytopenia with at least one additional clinical finding (elevated white blood cells, elevated hematocrit, abnormal chest x-ray, or supplemental oxygenation). This combination most closely matched the current CDC/CSTE surveillance case definition, and 57% of all patients in the study met the criteria. Sensitivity was 84% while specificity was 58%. The criteria for combination B, which required the presence of thrombocytopenia and at least one additional finding of fever, elevated white blood cells, elevated hematocrit, chest x-ray suggestive of HPS, or receiving supplemental oxygenation, was met by 68% of all patients tested and had the highest sensitivity of all combinations at 97% while specificity was 49%. Combination C, which required the presence of fever, thrombocytopenia, elevated white blood cells, elevated hematocrit, positive chest x-rays, and supplemental oxygenation, had the highest specificity of 96%, while sensitivity was 49%. Eighteen percent of patients tested fit the criteria for combination C. Combination D included both thrombocytopenia and elevated hematocrit, and had a moderate sensitivity of 69% and a high specificity of 91%. Thirty-one percent of patients tested fit combination D criteria.
Se, diagnostic sensitivity; Sp, diagnostic specificity;
For PLR and NLR calculations, please see methods section.
Combinations with the highest numeric value for the given calculation are shown in bold.
Discussion
This study evaluated an extensive national sample of suspect HPS patients, calculating the diagnostic sensitivity and specificity of routinely observed symptoms and clinical findings that could serve as potential indicators of HPS in the United States. The single clinical finding with the greatest sensitivity for HPS was thrombocytopenia, which was present in 97% of HPS-confirmed patients. The clinical finding with greatest specificity was elevated hematocrit, which was absent in 83% of HPS test-negative patients. Both thrombocytopenia and elevated hematocrit were found to be significant predictors of HPS in this study and in a previous study (Chapman et al. 2002). Chest x-rays with findings suggestive of HPS or receiving supplemental oxygenation had high diagnostic sensitivity, but both variables also had very low specificity (17% and 12%, respectively), which reduced their value in differentiating HPS from other respiratory diseases.
Of interest was the moderate sensitivity of fever (81%). It is likely that all patients with HPS indeed have febrile illness, but perhaps not necessarily at the time of presentation. Fever was a reported symptom in all 17 HPS-positive patients in the initial 1993 outbreak, although observed temperatures greater than 38.1°C were only reported in 75% of these patients (Duchin et al. 1994). Other studies have shown that a large proportion (>90%) of HPS patients had fever (Hallin et al. 1996; Khan et al. 1996; MacNeil et al. 2011). Because fever, particularly during prodromal illness, is a common symptom of HPS, we do not suggest to alter the current suspect case definition, but rather to modify it slightly, to indicate that the presence of fever at any time during the illness would meet this criterion.
In order to detect trends and tailor public health messages, we believe it is important for surveillance to accurately capture a high proportion of HPS patients. Having a suspect case definition with maximum diagnostic sensitivity will serve to detect nearly all potential cases, which can then be confirmed by highly specific diagnostic testing. The current suspect case definition as described by combination A correctly classified 84% of HPS-positive patients, mainly because a fever >38.3°C was not always noted in positive cases. Combination B, which removed the requirement of fever but required thrombocytopenia and at least one additional clinical sign, increased sensitivity by 13%, so that 97% of the HPS-positive patients would fit this definition. The specificity for combinations A and B was fairly low (58% and 49%, respectively), which limited the clinical value to rule out other potential etiologies. However, it is expected that all patients suspected of HPS would be confirmed through the use of diagnostic testing, which would provide adequate specificity. Although only a small proportion of patients fit the criteria described in combination C, this combination had high diagnostic specificity and positive-predictive value, meaning that most patients with this combination of symptoms had HPS. Combination D, which combined the highly sensitive indicator of thrombocytopenia with the highly specific indicator of increased hematocrit, had the benefit of moderate sensitivity and high specificity. However, the application of combination D in a clinical setting would be suboptimal, because nearly one-third of HPS-positive patients would not meet the criteria and be missed due to lower sensitivity.
A likelihood ratio (LR) is defined as the likelihood that a patient with disease has (or does not have) a particular symptom or test result compared to a patient without (or with) disease (Deeks and Altman 2004). Similarly to other ratios, LR can be interpreted as follows: a result <1.0 would indicate a lesser likelihood, and a result >1.0 indicates a greater likelihood. In this analysis, the PLR is interpreted as the probability a patient with HPS has the symptom or clinical finding of interest, as compared with a patient without HPS having the same symptom or clinical finding. Similarly, the NLR−1 is the likelihood that a patient does not have HPS when the symptom or clinical finding of interest is absent, as compared with the likelihood that a patient with HPS would also not have that symptom or clinical finding. LRs have the benefit of being applicable in a clinical setting, where a clinician can use the result to consider the probability of HPS based on the clinical signs observed: a LR of 2 increases the probability by 15% (minimal increase), 4 by 25% (small increase), and 10 by 45% (large increase) (Grimes and Schulz 2005). While both combinations A and B had PLRs of approximately 2, combination D had a PLR of 7 (moderate increase in the likelihood of HPS), and C of >10 (large increase in the likelihood of HPS). Clinicians with patients who fit the criteria outlined by combination A or B may then wish to perform additional clinical evaluations (described below) while awaiting diagnostic test results, while a patient whose clinical findings fit combination C may be considered more likely to have HPS, and could receive more aggressive empirical treatment in the period when diagnostic tests are pending. Perhaps even more relevant to clinical practice, a patient whose symptoms do not fit those described by combination B has a NLR−1 of 16, indicating that HPS is unlikely and other diagnoses should be considered.
Previous studies have produced criteria that can be applied to HPS-suspect patients to raise or lower suspicions of HPS. An algorithm was developed (Moolenaar et al. 1995) that found that myalgias, nausea, and vomiting were initial complaints significantly more often in HPS patients than in patients with influenza, bronchopneumonia, and unexplained ARDS. Such findings were supported by Chapman and associates (Chapman et al. 2002). Koster and colleagues (Koster et al. 2001) evaluated blood smear findings in suspected HPS patients once the onset of pulmonary symptoms had commenced, and found a highly sensitive and specific (96% and 99%, respectively) indication of HPS with the combination of at least four of the five following findings: (1) elevated hematocrit, (2) thrombocytopenia, (3) myelocytosis, (4) without toxic changes in the myelocytes, and (5) >10% immunoblasts and plasma cells in lymphoid cells. Such tests can serve to aid physicians in determining the likelihood of HPS and when to engage in necessary empiric therapy while confirmatory diagnostic tests are pending, which may take several days.
The predominantly western distribution of U.S. HPS illnesses has long been observed, and is most likely related to the distribution of P. maniculatus, the primary reservoir for SNV (Douglass et al. 2005). To date, >95% of all reported cases have occurred west of the Mississippi River (Centers for Disease Control and Prevention 2011), which was also reflected in the dataset used for this report, and we had only 9 patients who resided east of the Mississippi River out of 205 total HPS-confirmed patients. While HPS rarely occurs in the eastern U.S., several well-documented illnesses, both with SNV and other closely related hantavirus species, necessitate its consideration and testing in patients whose clinical picture is consistent with HPS (Mills et al. 2009).
This study was limited by the following factors. While using case report forms allowed us to capture standardized patient information—essential to a study of this scope—clinical information was less detailed than medical records, and may not capture the full range of signs and symptoms experienced by patients. However, considering that a high proportion of HPS-suspect patients had respiratory manifestations reported in the case report forms (chest x-rays with diffuse pulmonary infiltrates and/or receiving supplemental oxygenation), it is likely that most patients were already in the acute pulmonary phase of disease at the time the information was provided. Data were collected through passive surveillance of diagnostic tests submitted to the CDC, and may not be representative of all HPS-suspect patients.
Laboratory testing was based on in-house serologic assays developed at the CDC. These assays have been extensively validated and demonstrated to broadly cross-react against New World Hantaviruses (Terajima et al. 1999). Comparisons of serology with immunohistochemistry and RT-PCR have shown high concordance using this test (91%) (Khan et al. 1996), indicating that antibodies are reliably present and detectable in confirmed HPS cases caused by SNV. Importantly, IgM is detectable in all patients as soon as 0–3 days post-pulmonary symptom onset (Bostik et al. 2000; MacNeil et al. 2010), therefore these assays are effective for diagnostic rule-out, regardless of the timing of sample collection.
In conclusion, this study evaluated symptoms and clinical findings for a nationwide set of patients suspected of HPS over 12 years of data collection. As a result of this analysis, we found that a suspect case definition which includes thrombocytopenia and the presence of fever at any time during illness in a patient with symptoms of acute respiratory distress had the maximum sensitivity in detecting HPS-confirmed patients. Maintaining a sensitive suspect case definition that is confirmed by highly specific diagnostic testing will best serve the goal of identifying every HPS case that occurs with great accuracy.
Footnotes
Acknowledgments
The authors would like to thank Thomas G. Ksiazek, Stuart T. Nichol, James A. Comer, and Kent D. Wagoner, for their assistance in the creation and maintenance of the national HPS surveillance system. Additional thanks are due to personnel at state and local departments of health. This study was funded by the Centers for Disease Control and Prevention. The findings and conclusions detailed in this manuscript are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention.
Author Disclosure Statement
No competing financial interests exist.