
Abstract
Toscana virus (TOSv) is a neurotropic arthropod-borne virus that causes meningitis in the Mediterranean basin during the summer months. A total of 120 patients suffering from acute aseptic meningitis between July 1 and October 31, 2010 in northern Italy were evaluated. Eighteen of them (15%) were in the acute stage of TOSv disease.
Introduction
Since 1983, TOSv has been recognized as causing aseptic meningitis in the Mediterranean basin during the vector season (late spring through early fall) (Schwarz et al. 1995; Cusi et al. 2010).
TOSv infections are clinically heterogeneous, remaining self-limiting without affecting the central nervous system (CNS). Certain cases of TOSv infection do not require hospitalization, and consequently the diagnosis is rarely confirmed by laboratory data; there is no defined surveillance system for TOSv in Italy (Dionisio et al. 2003). These properties are likely to account for the few TOSv infections that are detected, whereas the West Nile virus surveillance system that is active during mosquito season in Emilia Romagna yields a defined epidemiological picture (Pugliese et al. 2007; Angelini et al. 2009).
Most cases of TOSv have been reported in residents of or travelers to central Italy and Spain, but its incidence is rising in other countries of the Mediterranean basin, including France, Portugal, Cyprus, and Greece (Nicoletti et al. 1991; Peyrefitte et al. 2005; Cusi et al. 2010).
The epidemiology of TOSv is well known in central (Braito et al. 1997; Valassina et al. 2003; Terrosi et al. 2009; Cusi et al. 2010) and southern Italy (Di Nicuolo et al. 2005), but few epidemiological data are available for north of the Appenini Mountains, where the few cases that have been described have always developed in travelers who returned from endemic areas (Portolani et al. 2002).
This study examined TOSv infections in the Emilia Romagna region (in the northern area of Tuscany, Italy), where the first surveillance system for acute TOSv meningoencephalitis was activated from July 1 to October 31, 2010.
Material and Methods
One-hundred twenty patients living in various areas of the Emilia Romagna region (Fig. 1), with signs and symptoms that were attributable to acute CNS infection, particularly aseptic meningitis, were enrolled in the study. All patients were hospitalized in one of the infectious diseases wards in hospitals throughout the region. Serum was taken from patients during the acute phase of the neurological disease. When clinically appropriate, CSF was drawn (11 of 120 specimens were tested). Serum and CSF samples were generally tested within 24 h of admission; if not, the specimens were stored at −80°C until analysis.

Circulation of Toscana virus in Emilia Romagna, Italy. The flag symbols show the areas of the region with Toscana virus acute infections.
Each patient's epidemiological, demographic, and clinical data were collected retrospectively in a dedicated database. Specifically, data on the potential exposure to TOSV vectors were carefully assessed, such as residence in rural areas with elevated concentrations of sandflies, and participation in professional or recreational outdoor activities in or travel to (within 2 weeks before clinical onset) known TOSv-endemic areas.
All samples were tested for West Nile infection as previously described (Angelini et al. 2010), and all were negative.
The virological diagnosis of TOSv was made by: (1) the identification of specific IgG and IgM to TOSv, and (2) molecular detection of the TOSv genome. IgG and IgM were detected by semi-automated, qualitative ELISA. IgM measurements were based on the “capture technique.” The presence of serum IgM indicated an active or recent infection by TOSv.
An in-house real-time RT-PCR method per Perez-Ruiz and colleagues (Perez-Ruiz et al. 2007) was used to detect TOSv RNA in cerebrospinal fluid (CSF) specimens.
Samples were extracted with the NucliSENS easyMAG automated nucleic acid extractor (BioMerieux, Marcy l'Etoile, France) and amplified with the SuperScript III Platinum One-Step Quantitative RT-PCR system (Invitrogen, Carlsbad, CA). The reaction mixture contained 0.5 μL of SuperScriptIII RT/Platinum Taq Mix, 10 μM of each primer, and 2.5 μM of probes. The reaction was performed on a Step-One Plus (Applied Biosystems, Foster City, CA).
Results
We performed a serological analysis of 120 patients, and 37 were positive for anti-TOSv IgG, 14 of whom also expressed anti-TOSv IgM; 1 patient developed an IgM response only.
Paired CSF and serum samples were available for 11 of the 37 serologically-positive patients. Because the serological method that we used is not officially approved for examining CSF, all 11 CSF specimens were evaluated by RT-PCR, wherein the CT value ranged from 8–10 (total CT was 35). Eight of the 11 CSF samples were positive by RT-PCR, and serum samples were positive for anti-TOSv IgG and IgM. The remaining three cases were positive only in the CSF samples by RT-PCR, all of whom were lost in the follow-up period, precluding any seroconversion from being detected.
Discussion
Based on these findings, 18 of 120 patients (15%) (15 IgM-positive and 3 RT-PCR-positive without IgM) had an ongoing acute TOSv infection. Clinically, these patients were reported as 14 cases of meningitis, 2 cases of meningoencephalitis, and 2 cases of encephalitis.
The age of the patients ranged from 17 to 83 years (mean age 42.5±19.4 years), and the male:female ratio was 1:1.8. We did not observe a significant association between older age and higher symptom severity.
The clinical course of the infection was mild in all cases; the median in-hospital length of stay was 7.2 days (SD±3.4 days), and the median duration of symptoms was 8.3 days (SD±7.2 days).
Fever and headache were the most common symptoms, occurring in 92% and 100% of patients, respectively. No associated comorbidities were noted. Other clinical, laboratory, and demographic characteristics of the 18 acute-stage patients are summarized in Table 1. All subjects had a positive prognosis and experienced complete recovery, with no neurological sequelae after 5 months of follow-up.
Fever and headache occurred in 92% and 100% of patients, respectively. No associated comorbidities were noted.
n.a., not available.
The epidemiological profiles of the acute infections are shown in Figure 1. Most cases occurred in the eastern part of the region, wherein 11 of 18 acute infections developed in the province of Bologna (Fig. 2). No entomological surveillance data on sandflies were available for this area during the study period.
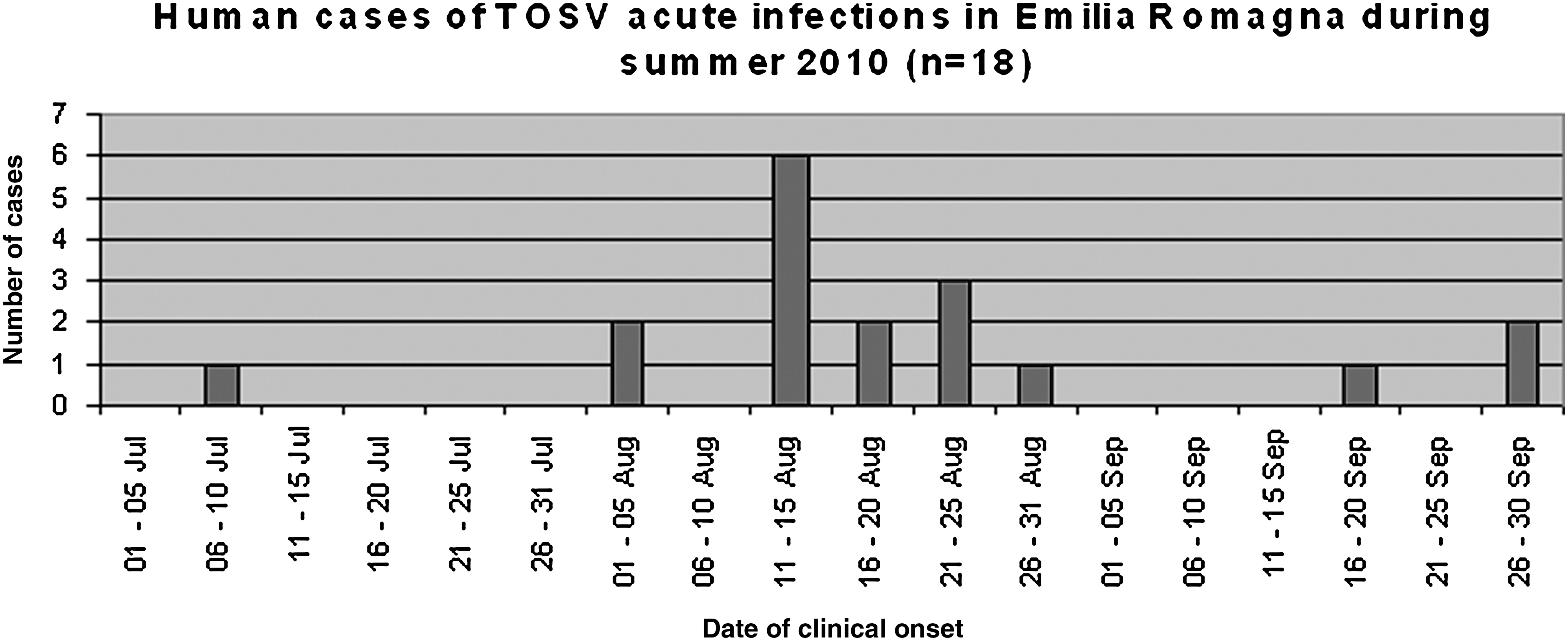
Epidemiological profile of the human cases of Toscana virus infection in northern Italy during summer 2010. Bars indicate the number of cases (n=18) and the periods of clinical onset.
In 13 of 18 cases, the infections might have had an autochthonous origin. However, that of the remaining 5 cases could not be determined, because the patients had traveled to central and southern Italy (Tuscany 2/18 and Lazio 1/18) and other countries (Spain 1/18 and Croatia 1/18) in the 4 weeks prior to clinical onset, raising the possibility that the infections were not autochthonous. For the 37 patients with only IgG responses, it was possible to determine when and where they acquired the infection.
The samples in this study are being evaluated with regard to the presence of TOSv-neutralizing antibodies; a phylogenetic analysis of the viral isolates is underway.
Regarding the limitations of our study, we only detected serum IgM in 4 cases, which might have been a false-positive result, because no additional samples were obtained from these subjects; thus seroconversion was not evaluated. Further, in 3 cases, we only obtained positive PCR results and could not study the generation of TOSv immune responses. These samples, 4 IgM+ and 3 PCR+ cases (7 in all), were included as positives to TOSV in our analysis (15% of positives).
Our results are significant, because they implicate the unusual circulation of phlebotomine sandflies in urban areas. Most patients apparently became exposed to vectors in urban locations—where TOSv vectors are believed to be scarce—not in rural areas.
Our study is the first report of a cluster of acute cases of TOSv infection in northern Italy, suggesting that TOSv circulates widely in the area north of the Appenini Mountains. Based on our results, we hypothesize that TOSv mediates the etiology of nonbacterial CNS infections in this area during the summer months. Thus, a systematic evaluation of this virus should be considered for all acute CNS infections during the vector activity season.
Footnotes
Acknowledgments
This study was supported by “Fondi Finalizzati Centro di Riferimento Regionale per le Emergenze Microbiologiche (LAB P3),” Regione Emilia Romagna.
Author Disclosure Statement
No competing financial interests exist.