
Abstract
There has been a marked increase in the incidence of tick-borne encephalitis (TBE) in the last two decades, with new foci of the disease evolving. TBE is endemic in Slovenia, and the incidence rate is one of the highest in the European Union. A survey of notified TBE cases started in 1999, aiming to collect additional epidemiological data that are not available through the usual notification system. From 1999 to 2009, a short, anonymous, self-administered questionnaire was sent to 2779 notified TBE cases. The response rate was 69.5%. The willingness to respond was higher in those over 60 years of age, but did not differ by gender. In all, 1564 (82.3%) of the responders had a tick bite on one or multiple sites on the body. Age and gender influenced the location of the tick bite: males patients most often had the tick located on the torso, and females had them on the legs. Ticks located on the head and neck were significantly higher in preschool children compared to school children and adults. The estimated duration of tick attachment was less than 6 h in 23.5% of TBE cases. Long attachments (more than 24 h) were reported by only 10% of the patients. The tick bite occurred while the TBE patients were engaged in leisure time activities (sports or camping, 32.8%), mushroom or berry picking (30.2%), or farming (23.3%). Almost two-thirds of TBE patients reported that they had practiced at least one of the recommended preventive measures, most frequently self-inspection, and least often repellent use. The patients were asked to disclose the most probable geographical location of the TBE viral (TBEV) infection. Maps were created on a county level and showed that the risk of TBE is widespread, with few counties unaffected. The counties located in the northern and the central areas had the highest risk of TBEV infection.
Introduction
TBE was recognized as a new clinical entity in the early fifties in the last century in Slovenia (Vesenjak-Zmijanec et al. 1955). TBE is an obligatory reportable communicable disease with an average incidence rate of approximately 13/100,000 in last 10 years (Grgič-Vitek and Klavs 2011). To gain knowledge on the epidemiological parameters of the disease in Slovenia, a survey began in 1999.
Materials and Methods
Data collection
The mandatory notification system requires every patient with meningo-encephalitis and a microbiologically-confirmed infection with TBEV to be reported to the regional public health authorities. The standard notification form includes the following data: name, surname, date of birth, permanent address, time of the onset of symptoms/signs, notification date, hospitalization, outcome data, and information on whether or not the diagnosis was confirmed by microbiological tests. Notified cases are recorded in the electronic Database for Notifiable Communicable Diseases. The notifications collected regionally are sent to the National Institute of Public Health on a weekly basis and the data are merged at the national level.
The survey
A short (two-page) anonymous, self-administered questionnaire was developed in 1998. From 1999 onwards, the questionnaire has been sent to every notified TBE case, together with an invitation letter. This article presents the data collected from 1999 to 2009.
The patients were requested to disclose their gender and age (in years) without a name or any other identifier. The feedback form contained questions on the tick bite before the illness, including the location of the tick bite (head, neck, arms, legs, or torso), the estimated duration of tick attachment, and the presence of an erythematous skin lesion (with a diameter of at least 5 cm) at the location of the tick bite.
The patients were asked to pinpoint, if possible, the most probable geographic location where they judge the infection with TBEV occurred, and what outdoor activity they were engaged in when they contracted the TBEV infection (e.g., recreational activities, farming, working in the forest, hunting, picking berries or mushrooms, or military service), and what kind of protection against ticks they used: vaccination against TBE, protective clothing, repellent, self-examination after outdoor activity, or nothing. The patients were asked about the consumption of goat's milk in the 3-week period before the illness.
Statistical analysis
The data collected were entered into Epi Info™ Version 6. The descriptive statistics included frequency analyses (percentages) for categorical variables. All the percentages were calculated using the number of patients with data available as the denominator. A chi-square test was used to test the differences for categorical variables. p Values <0.05 were considered statistically significant.
The most probable geographic location of the infection was entered on a map of Slovenia. The population by county was extracted from the web pages of the Statistical Office of the Republic of Slovenia (
We decided not to ask for ethical approval for the study, as the patients responded anonymously and on a voluntary basis.
Results
Demographic data
The survey started in 1999 and ran until the end of 2009. The questionnaire was sent in total to 2779 notified TBE cases, and 1930 TBE patients chose to return the completed or partially completed forms with some questions left unanswered. The response rate varied slightly from year to year. The lowest response rate was in 2003 (63.8%), and the highest percentage of patients responded in 2004 (74.5%), with an overall response rate of 69.5%. The gender and age structure of the responders was compared to the notified TBE cases. There were 1579 (56.8%) males and 1200 (43.2%) females among the notified cases. The distribution by gender was practically the same among those who responded; 54.9% of male and 44.1% of female patients responded, and 1.0% of the responding patients refused to reveal their gender.
Patients over 60 years old were more willing to respond compared to younger and middle-aged adults, as shown in Figure 1.
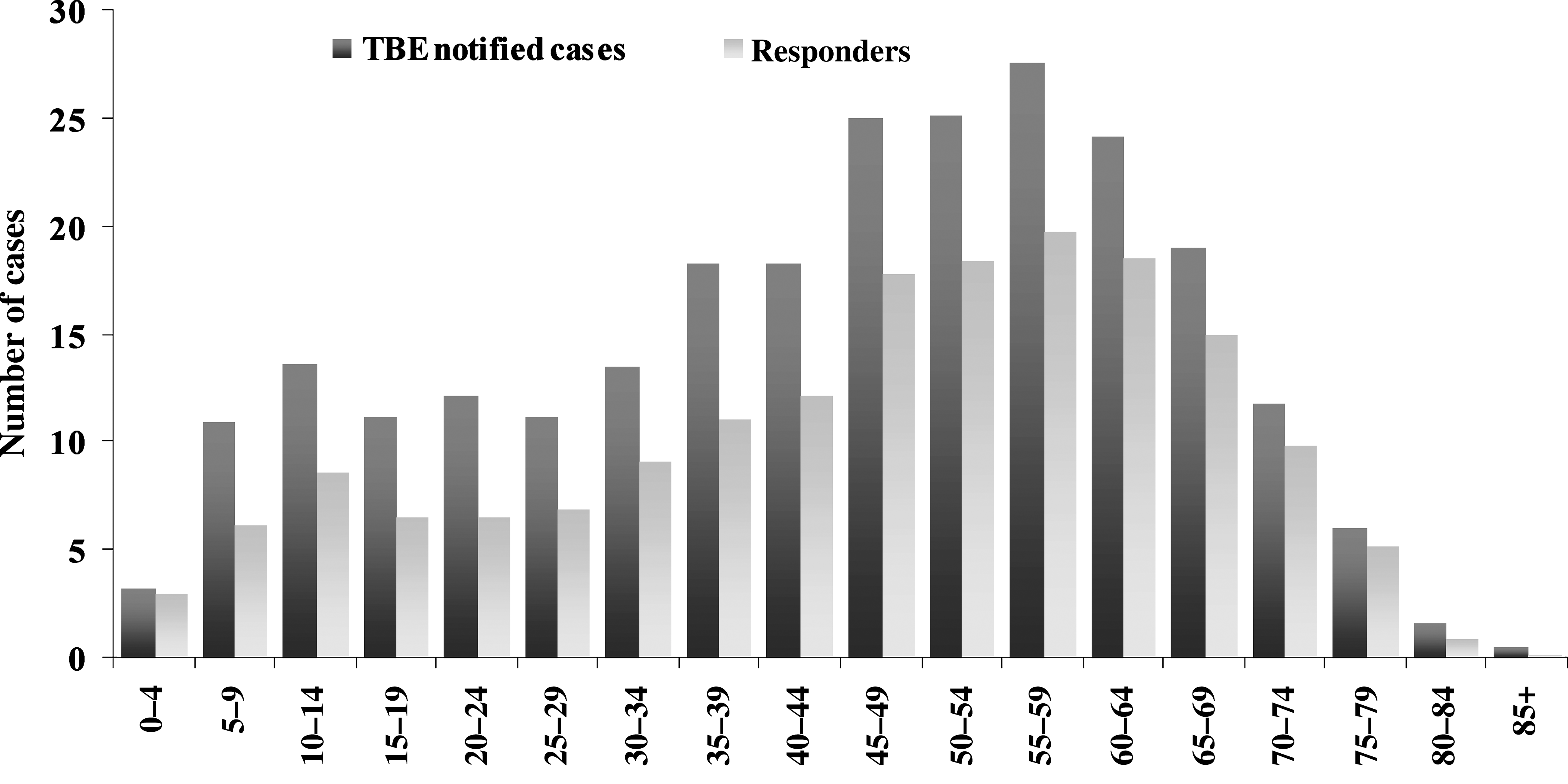
The age structure of tick-borne encephalitis (TBE) notified cases and the survey responders from 1999 to 2009.
Tick bite
A total of 1564 (82.3%) of the responders knew they had a tick-bite on one or multiple sites of the body (Table 1), and 336 (17.7%) of responders did not remember the bite before the illness. The tick bite was most frequently found on the torso only (563 patients, 36%), while an additional 233 patients had the bite on the torso and on some other part of the body (Fig. 2).
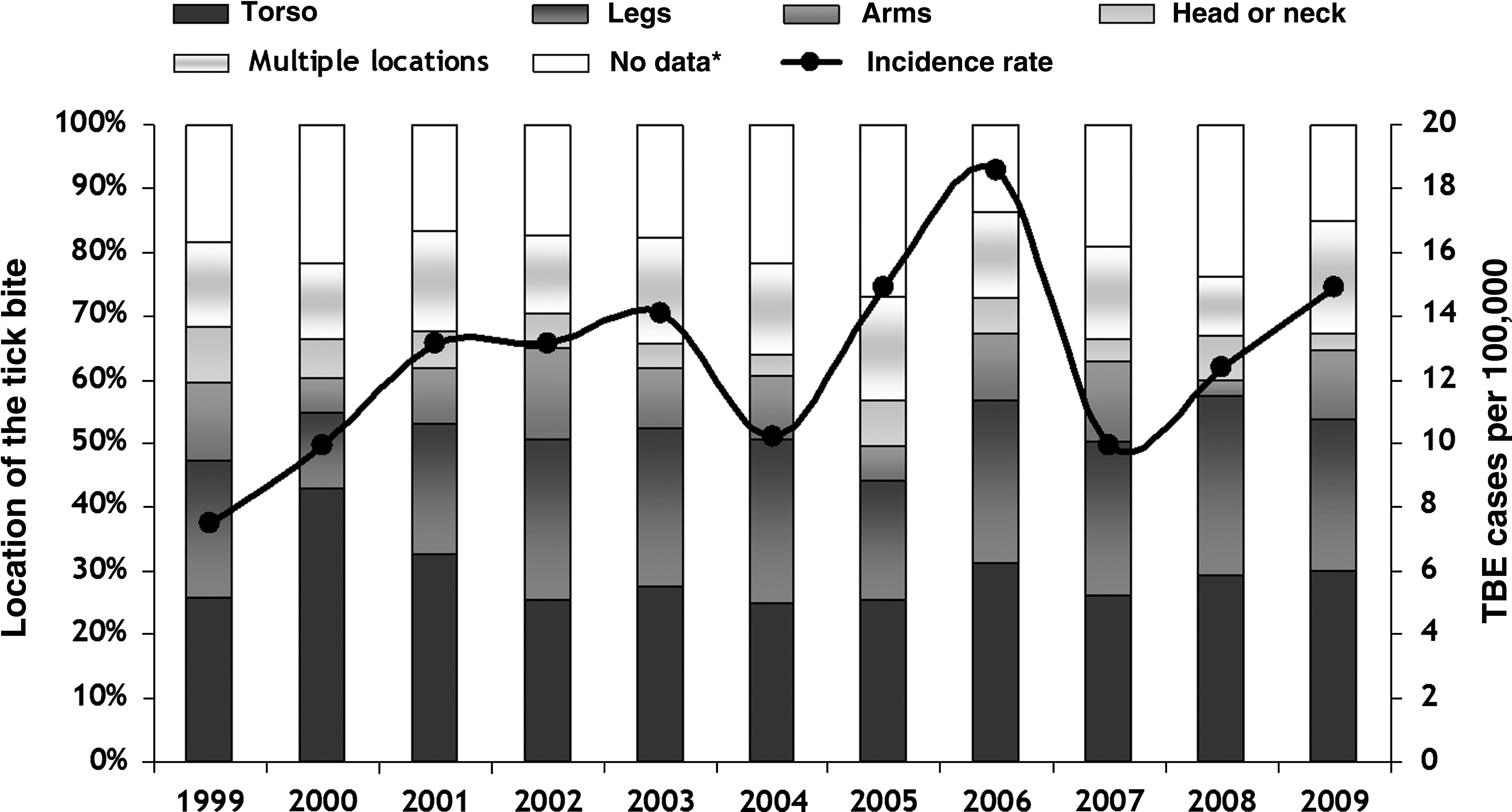
The reported incidence rate of tick-borne encephalitis (TBE) in Slovenia from 1999 to 2009 and the location of the tick bite. No data*; No location of the tick bite disclosed.
Age and gender influenced the location of the tick bite. A much higher percentage of preschool children (aged less than 7 years) received a tick bite on the head and neck compared to school children (p=0.003) and adults (p<0.001). Significantly higher numbers of females claimed to have a tick bite on the head or neck (p=0.003), or lower extremity (p=0.002), than male patients. The male patients more frequently found the tick bite located on the torso than females (p<0.001).
Duration of tick attachment
The patients were asked to estimate how long the tick had been attached to the skin before it was found and removed, and 367 (23.5%), 474 (30.3%), and 314 (20.8%) patients estimated that the tick was attached for less than 6 h, 6–12 h, and 12–24 h, respectively. Also, 169 (10.8%) judged that the tick was attacked for more than 24 hours (Fig. 3). There was no difference in the duration of the attachment by age group or sex (p=0.486 and p=0.226, respectively).
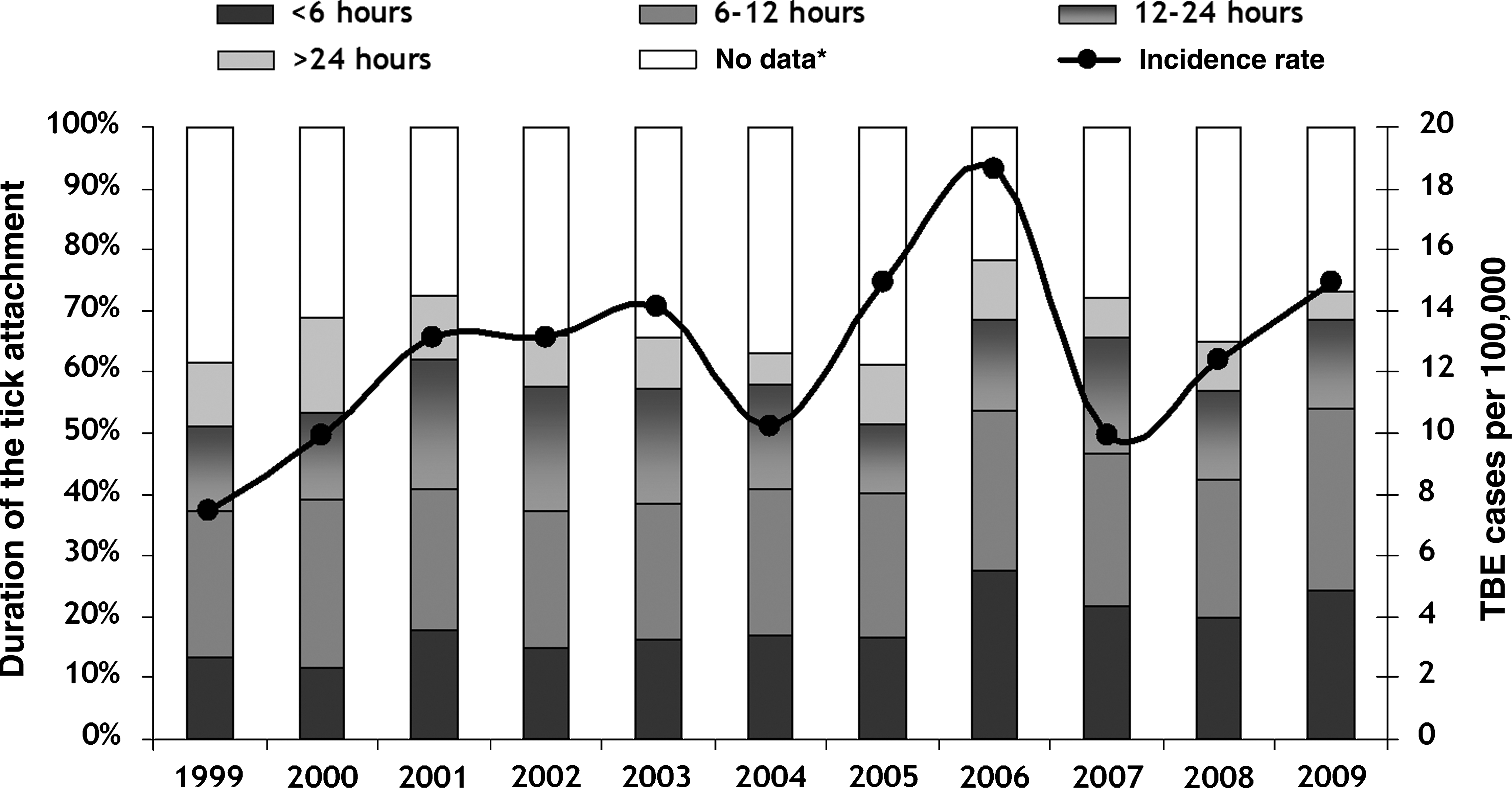
The reported incidence rate of tick-borne encephalitis (TBE) in Slovenia from 1999 to 2009 and the estimated duration of tick attachment.
An erythematous area larger than 5 cm in diameter around the tick bite was reported by 85 (5.4%) of patients. The percentage of women with erythematous lesions did not statistically significantly outnumber men (p=0.346). There were no additional questions posed to the patients with TBE to indicate the nature of the skin lesion; it could be erythema migrans, or just a more intensive skin reaction around the tick bite.
Sixty-nine (3.6%) patients were goat's milk consumers. The non-consumers were compared to the consumers regarding tick bites, and 82% of the non-consumers remembered receiving a tick bite before the illness compared to 78% of the consumers (p=0.342). As a high percentage of goat's milk consumers had a history of tick bites, it is not possible to draw any conclusion regarding the source of infection. Theoretically it could be from infected goat's milk or vector-borne.
Activity at the time of the tick bite
The largest number of responders (618 patients, 32.8%) were spending their leisure time outdoors engaged in walking, jogging, other sports or camping when the tick bite occurred. The next highest number (569 patients, 30.2%) were picking mushrooms or berries, 440 (23.3%) were infected with TBEV while farming, and 63 (3.3%) worked in the forest as foresters, professional hunters, or military personnel when they were exposed. There was a significantly higher number of men farming or on duty when they were bitten by the tick (p=0.005 and p<0.001, respectively). Picking mushrooms or berries seems to be predominantly a women's hobby, as a significantly higher percentage of women experienced the tick bite during this activity (p<0.001). No difference was found by comparing males and females for leisure time activities (p=0.633).
The TBE patients who claimed that they acquired the infection during leisure activities were significantly younger compared to those who were picking mushrooms or berries when exposed.
In all, 1348 (70.6%) patients believed that they contracted the infection within their county of residence at the time of infection. There was no difference found when comparing males and females or age groups. Infections within the county of residence were acquired in 92% of the farmers, in 60% of those who were in the forest professionally, 68% of those picking mushrooms or berries, and 78% of those who were undertaking leisure activities.
Self-protection against tick-borne infections
The patients were asked what kind of protective measures they were using before they contracted TBE. Approximately a third of them (583 patients, 31.5%) self-inspected, 167 (9.0%) were dressed appropriately during outdoor activity, 122 (6.7%) applied repellent, 16 (0.9%) claimed to have received at least one dose of TBE vaccine (1–3 patients per year), and 426 (23.0%) combined protective measures. Wearing long-sleeved clothing and self-inspection after outdoor activity were practiced most frequently (alone or in combination with other protective measures).
Some 535 (28.9%) of responders did not use any of the above measures. Women claimed to use them more often than men.
Maps
The patients disclosed the most probable geographical location where they acquired the TBEV infection. The county incidence rates were calculated and maps were drawn. As shown in Figures 2 and 3, the incidence rates varied from year to year. In years with a higher number of cases, there was a more widespread geographical appearance of the TBE cases. Nevertheless, there were cases every year in the counties located in the central part of the country (Fig. 4).
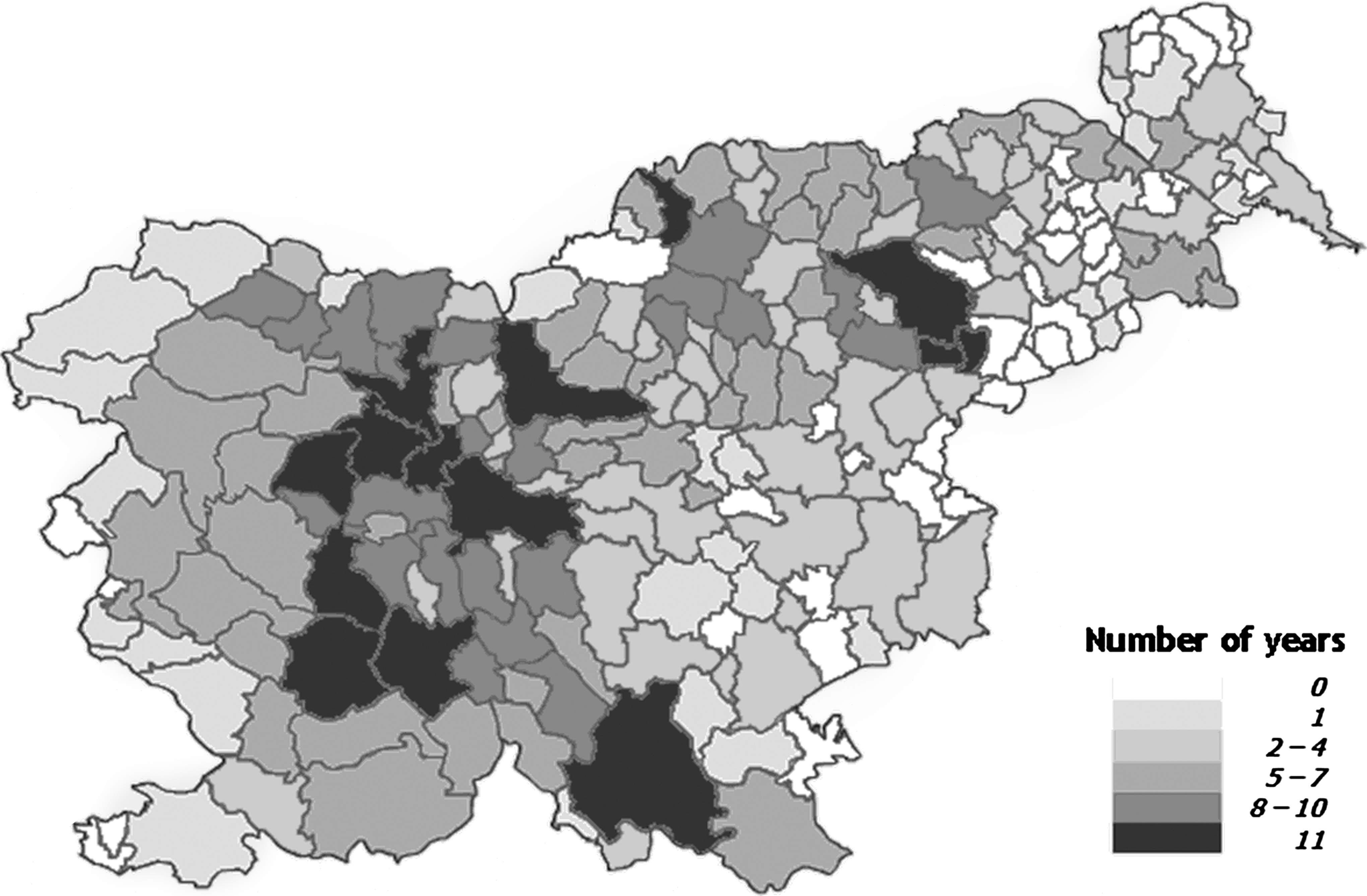
Occurrence of tick-borne encephalitis (TBE) by counties in Slovenia, and the number of years with at least one reported TBE case per county from 1999 to 2009.
Discussion
This study gives us insight into the epidemiology of TBE in Slovenia based on an analysis of the data collected through a survey of notified TBE cases.
More than 80% of the patients with TBE were able to remember a tick bite. A similar percentage of TBE patients recalling a tick bite was found in an earlier clinical study (Logar et al. 2006). In a study focusing on severe forms of TBE, significantly lower numbers of patients (58%) noticed a tick bite before admission (Jereb et al. 2006).
The torso was the most common anatomical area bitten by ticks in the present survey, followed by the legs and arms. The legs were the major anatomical site of bites, followed by the torso in two observational studies (Robertson et al. 2000; Hügli et al. 2009). The previous studies found that more children than adults were bitten on the head or neck area (Robertson et al. 2000; Hügli et al. 2009), a finding confirmed by this survey. Children's shorter height and behavior in the outdoor environment are the most probable reasons for the difference observed. An interesting finding in this study was that a statistically significantly higher number of women than men claimed to have the tick bite located on the head or neck. More female than male patients acquired the tick while picking mushrooms or berries. Picking blueberries is most popular in the early summer, when the air temperatures are usually pleasant and the humidity is suitable for ticks to be active. Collecting blueberries takes a lot of time and the picker has to lean forward or crouch down to reach the low blueberry bushes. This position of the picker gives the ticks in the nearby undergrowth the opportunity to attach themselves to the head or neck area.
The duration of the tick attachment seems to be an important factor for infection. The risk of transmission increases with the duration the tick is attached (Hügli et al. 2009). TBEV could be transmitted from the saliva of an infected tick within minutes of the tick bite (Lindquist and Vapalahti 2008). In the present survey, TBE patients were asked to assess the duration of tick attachment. Slightly fewer than a quarter of them claimed to have the tick attached for a relatively short time (less than 6 h), and only 10% for more than a day. Our findings support previous observations that early tick removal does not prevent TBE. Nevertheless, the data should be interpreted cautiously, as the reliability of the patients' reports is impossible to assess.
One-third of TBE patients probably acquired the tick infected with TBEV during outdoor sports or camping. A healthy lifestyle demands regular physical activity, though outdoor activities during the warmer part of the year pose a risk of acquiring vector-borne diseases, a fact confirmed by this survey. Slightly fewer than one-third of our TBE patients were picking berries or mushrooms when they had contact with infected ticks. This activity is highly risky for a tick bite, as pickers wander for hours in bushy areas of the forest.
A study from the Czech Republic showed that TBE remains a recreational disease, as low numbers of farmers were affected (Križ et al. 2004). In this study, approximately a quarter of the patients (23%) with TBE most likely became infected while farming. According to official statistics, 2% of Slovenian citizens are registered as farmers (Statistical Office of Slovenia, available at:
Protective clothing, applying repellent, and self-inspection after outdoor activity are recommended measures to prevent a tick bite and the transmission of tick-borne diseases. The data on the effectiveness of these measures are limited (Orloski et al. 1998; Vázquez et al. 2008). A case-control study from Connecticut in the U.S. showed that protective clothing and the use of tick repellents on the skin or clothing were 40% and 20% effective against Lyme borreliosis, respectively (Vázquez et al. 2008). Self-inspection after outdoor activity did not appear to offer any protection (Vázquez et al. 2008). Wearing long clothing (pants and long-sleeved shirts) does not prevent a tick-bite on the head or neck. The repellent should be applied on all exposed parts of the body, and reapplied after a couple hours, or even sooner if someone is sweating intensely. Approximately 70% of TBE patients who responded claimed to use one of the recommended preventive measures to avoid a tick bite. Practicing protective measures was self-reported, so the actual practices and their appropriateness could not be validated. Sixteen patients (0.8% of responders) claimed to be vaccinated against TBE before the illness. It is not known how many doses were administered or the time elapsed between the last dose of vaccine and the TBE infection. Not asking for a detailed vaccination history was identified as one of the questionnaire's shortcomings, which has been corrected in 2010. The reason for TBE vaccine failure can only be guessed; it might be a consequence of non-compliance with the recommended schedule or a genuine vaccine failure. The latter has been clearly documented, even in effectively vaccinated individuals (Grgič-Vitek et al. 2011).
The number of reported cases of two vector borne diseases–Lyme borreliosis (LB) and tick-borne encephalitis—are high in Slovenia (Arnez and Avsic-Zupanc 2009, Sumilo et al. 2008). The notified incidence rate from 1999–2009 for TBE was 12.6/100,000, and for Lyme borreliosis was 195/100,000 (per data from annual epidemiological reports, available at:
The country's natural environment and climatic conditions are supportive for the survival of ticks, small mammals, and ungulates, as most Slovenian forests are located within areas of beech, fir-beech, and beech-oak growth. In the second half of the 19th century the forests covered only 36% of the territory. The social changes seen in last century, notably the move away from farming and the industrialization of the country, caused the forests to spread and cover areas where meadows and pastures used to be. Today, forests cover approximately 60% of the country, which makes Slovenia the third most forested country in Europe (
Human habits (including the location of residency) strongly influence the distribution and incidence of vector-borne diseases (Süss et al. 2011). It is much less likely to acquire a tick-borne infection in a highly urbanized area (though not impossible) than in a forested rural area. The Organization for Economic Cooperation and Development (OECD) classifies regions as predominantly urban, intermediate, or predominantly rural, depending on the population density. According to the OECD, Slovenian regions are classified as rural or intermediate (
In conclusion, this survey disclosed for the first time the counties in Slovenia with the highest risk of TBEV infection. The results of the survey underline the importance of continuous surveillance of tick-borne diseases in ever-changing natural and social environments.
Footnotes
Author Disclosure Statement
No competing financial interests exist.