
Abstract
We conducted a cross-sectional study to assess cattle owners' awareness, perceptions, and attitudes toward zoonoses, with particular emphasis regarding anthrax. Data on awareness of zoonoses, clinical signs of anthrax in animals and human, its routes of transmission and methods of prevention, the families' consumption habits of anthrax-infected carcasses, and other family activities that increase exposure to anthrax were collected using an interviewer-administered questionnaire. A total of 41.4% (135/326) of the farmers were from high-anthrax-risk districts, whereas 28.5% and 30.1% were from medium- and low-risk districts, respectively. Overall, the level of awareness amongst the farmers for the named zoonoses were rabies (88.7%), anthrax (71.5%), and brucellosis (20.9%). Except for anthrax, awareness of other zoonoses did not differ significantly (p>0.05) among the district categories. Farmers from anthrax high-risk districts were significantly more aware of anthrax compared to those from moderate- (p=0.000) and low- (p=0.000) risk districts. All of the farmers were aware that anthrax occurs in cattle, and 73% indicated the presence of unclotting blood oozing from natural orifices as a consistent finding in cattle that died of anthrax, whereas 86.7% of them indicated the presence of skin lesions as the most common sign of the disease in humans. The good efficacy of human anthrax treatment (58.3%), slaughter of moribund cattle and selling of meat from cattle found dead to unsuspecting consumers (59.8%), reluctance to lose animals (47.9%), and forgetting about anthrax (41.1%) were cited as the major reasons for consuming anthrax-infected carcasses. Given that 75.2% of cattle owners indicated that they would not consume meat from cattle found dead, because they were discouraged by veterinary authorities, introducing meat inspection services is likely to have a positive impact in preventing human anthrax outbreaks in Zimbabwe.
Introduction
Human behavior, such as skinning and cutting meat of infected carcasses, not using protective clothing, eating contaminated meat, and belonging to a religious sect that allows eating of meat from animals that have died of unknown causes, have been reported to be important risk factors contributing to frequent outbreaks of human anthrax in Zimbabwe (Mwenye et al. 1996, Chirundu et al. 2009, Gombe et al. 2010). It has been reported elsewhere that this human behavior is partly influenced by lack of awareness (Mosalagae et al. 2011), perceptions, and attitude (Opare et al. 2000, Shirima et al. 2003, John et al. 2008), and/or misconceptions (Webb 2003) about zoonoses. Hence, it is important for cattle owners to acquire a certain degree of awareness of livestock diseases in their areas, the risks they pose, and possible transmission routes to humans, if they are to make informed decisions on diseases suspected to have zoonotic potential. Studies on awareness of pet (Pfukenyi et al. 2010) and milk-borne (Mosalagae et al. 2011) zoonoses have been conducted in urban/periurban areas and commercial and smallholder dairy farms, respectively, but they have not been carried in the rural communities of the country. Although a few relevant studies in communal areas have focused on risk factors in the face of human anthrax outbreaks (Mwenye et al. 1996, Gombe et al. 2010), information is not available regarding the level of public awareness and the risk of anthrax in these rural communities. Thus, the objective of this study was to assess cattle owners' awareness, perceptions, and attitudes toward zoonoses with particular reference to anthrax in low-, medium-, and high-anthrax (Chikerema et al. 2012) outbreak settings. It is envisaged that the baseline information generated will facilitate the development of effective guidelines and policies for controlling anthrax outbreaks.
Materials and Methods
Study location and selection of study sites
The study was conducted in rural communities of 7 districts in Zimbabwe for the period February to November, 2010. On the basis of the mean number of outbreaks per district, mean number of years of occurrence, and mean number years of recurrence of cattle anthrax outbreaks over a 40-year period (1967–2006), administrative districts in Zimbabwe have been classified as high-, medium-, and low-risk anthrax districts (Chikerema et al. 2012) (Fig. 1). On the basis of this classification, three high-, two medium-, and two low-risk districts were randomly selected, giving a total of 7 study districts. The selected high-risk districts were Chegutu, Murewa, and Lupane in the central, northeastern, and northwestern parts of the country, respectively. Gutu and Makoni were the selected medium-risk districts, whereas Chiredzi and Gwanda were the selected low-risk districts (Fig. 1).
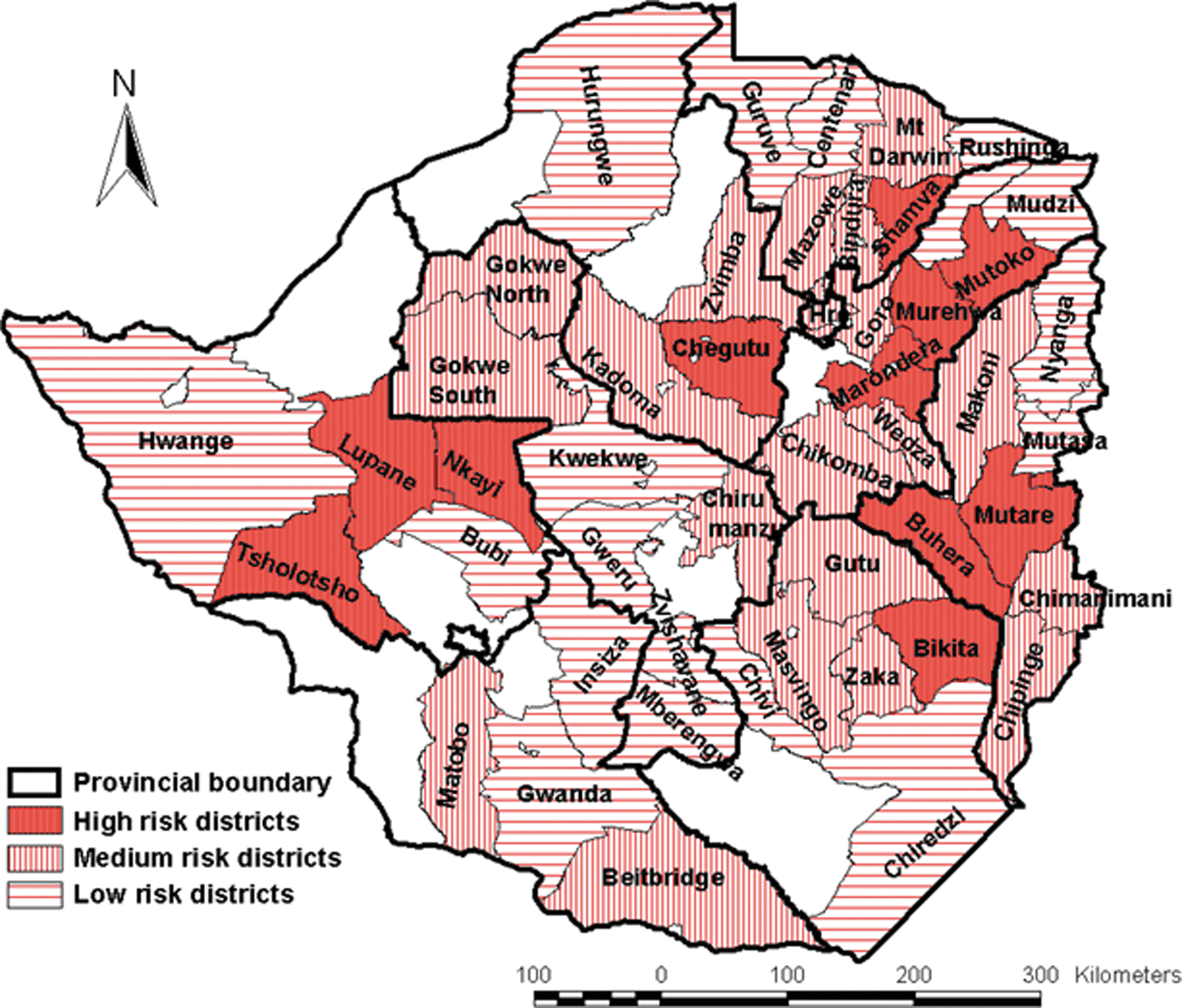
High-, medium, and low-anthrax-risk districts for the period 1967–2006. (Color images available at
In Zimbabwe, animal health regulations compel cattle owners in rural communities to dip their cattle weekly during the rainy season and fortnightly during the dry season for control of ticks and tick-borne diseases. Considering that over 90% of cattle owners dip their cattle (DVS Annual Reports), dipping attendance was believed (by us) not to be a significant source of selection bias for the farmers. Hence, due to easy access to cattle owners during the dipping sessions, dip tanks were selected as the study sites for focus group discussions with cattle owners and animal and human health workers. Two dip tanks were randomly selected from each district, giving a total of 14 study sites. Due to logistical constraints, households nearest to the selected dip tanks were visited for a one-on-one questionnaire survey of the cattle owners. A written ethical approval to carry out the study was obtained from the Department of Veterinary Services and the Ministry of Health.
Data collection and analysis
A cross-sectional survey was employed to collect data from the respondents. A semistructured, open-ended questionnaire was developed to gather information on the awareness, perceptions, and attitudes towards zoonoses by farmers. Field-testing of the questionnaire was conducted in January, 2010, in 1 district, which was not included in the study, where the easiness of completion and lack of clarity of questions was noted and subsequently revised. Interviews of farmers using the semistructured questionnaire (Supplementary Data are available at
The questionnaire was designed to obtain information on known zoonoses, awareness of anthrax, causative agent of anthrax, animals affected, animal and human clinical signs of anthrax, time of occurrence of anthrax, and routes of transmission of the disease. Respondents were also asked about consumption habits, family and community-based activities that increase risk of contracting anthrax, treatment-seeking behavior, and prevention of anthrax.
Each respondent's responses were recorded and entered into a Microsoft Excel database. Data analysis was carried out using SPSS 16.0 for Windows to generate descriptive statistics (frequencies/proportions) related to the cattle owners' awareness of zoonoses, causative agent of anthrax, animals affected, animal and human clinical signs of anthrax, time of occurrence of anthrax, routes of transmission of the disease, consumption habits, family and community-based activities which increase risk of contracting anthrax, treatment-seeking behavior, and prevention of anthrax. The chi-squared test was used to measure associations between categories, and values of p<0.05 were considered as significant.
Focus group discussions were used to probe further and have an in-depth understanding and a consensus on some of the issues arising during individual interviews. The focus group comprised of key informants, such as animal and human health workers and the farmers. This was carried out to crosscheck responses given by individual respondents during questionnaire interviews. The responses that were selected for group discussions were those reported by less than 20% and/or greater than 60% of the respondents. Data generated during the focus group discussions were collected through notes taken by the moderator and audiotapes. Framework analysis (Rabiee 2004) was used to analyze the focus group discussions data.
In addition to questionnaire information, data on anthrax outbreaks and cases in cattle and humans in the studied districts were also extracted from the monthly reports of various departments within the Division of Livestock Production and Veterinary Services in Harare for the period January, 1995, to March, 2010.
Results
Demographics of respondents and anthrax outbreak data
Table 1 summarizes the number of participants involved in the survey and anthrax data of the studied districts for the period 1995 to March, 2010. A total of 41.4% (135/326) of the farmers were from anthrax high-risk districts, while 28.5% (93/326) and 30.1% (98/326) were from medium- and low-risk districts, respectively. Out of the 326 farmers, 226 (69.3%) were males and 100 (30.7%) were females. Sixty percent of the farmers were above 25 years of age and over 85% had undergone formal education. Over 90% of the farmers owned cattle and over 80% of them belonged to different Christian denominations. In general, the interviewed farmers had small herd sizes, with the majority (>60%) having 6–10 cattle.
During the period January, 1995, to March, 2010, the high-risk anthrax districts accounted for 67% of the cattle outbreaks in the studied districts, followed by the medium-risk districts (25%); the low-risk districts recorded the lowest (8%). No cattle outbreaks were recorded in Gwanda, a low-risk anthrax district. Human outbreaks were recorded in the high- (90.2%) and the medium-risk districts (9.8%) only with no outbreaks reported in the low-risk districts.
General awareness of zoonoses
Table 2 shows the zoonoses named by farmers. Farmers were mostly aware of rabies (88.7%), anthrax (71.5%), and brucellosis (20.9%). Other zoonoses mentioned were bovine tuberculosis, Rift Valley fever, and bovine cysticercosis. Except for anthrax, awareness of named zoonoses did not differ significantly (p>0.05) among the studied district categories (Table 2). Overall, farmers from anthrax high-risk districts were significantly more aware of anthrax compared to those from moderate- (χ2=20.9, degrees of freedom [df ]=1, p=0.000) and low- (χ2=66.7, df=1, p=0.000) risk districts. However, farmers from Chiredzi (65.2%), classified as an anthrax low-risk district, had a relatively high awareness of anthrax. Overall, farmers from anthrax low-risk districts were significantly more aware of brucellosis (p=0.024), Rift Valley fever (p=0.006), and bovine tuberculosis (p=0.001) compared to those from anthrax high-risk districts. Chiredzi district recorded the highest awareness for brucellosis (43.5%), bovine tuberculosis (37%), and Rift Valley fever (21.7%), whereas Gwanda recorded the highest for bovine cysticercosis (7.7%). Animal health workers were aware of all the zoonoses named by cattle owners. However, in contrast, the human health workers were aware of rabies, anthrax, and to some extent tuberculosis only as zoonoses.
District categories with different superscripts within same columns differed significantly (p<0.05).
Anthrax detection
When asked specifically about anthrax, less than 30% of the farmers knew the causative agent of the disease. All farmers knew that anthrax occurs in cattle. Other animals mentioned, in which farmers had noticed the disease, were goats, pigs, and kudus by farmers from Lupane, Chegutu, and Chiredzi, respectively. When questioned on clinical signs that suggest anthrax in animals, farmers mentioned the presence of blood oozing from natural orifices (73%), unclotting blood (69.3%), sudden deaths (41.4%), and rapid decomposition (37.1%) as signs indicative of anthrax (Table 3). In humans, the presence of skin lesions (86.7%) was identified as the most predominant sign suggestive of anthrax, whereas less than 20% of the farmers reported diarrhea and vomiting as other clinical signs of anthrax in humans (Table 3). Skinning (96.6%) and eating (85.3%) infected carcasses were mentioned as important routes of transmission. A very high proportion (91.4%) of the farmers indicated that they would refer a sick family member who had consumed an anthrax carcass to the clinic or hospital, whereas a very small percentage (7.7%) would send to a traditional healer (Table 3). Over 80% of the farmers were aware of anthrax preventive measures, such as burying and/or burning the carcass and vaccination (Table 3). Most farmers (85%) indicated that the disease occurs during the dry season.
Consumption behaviour and family activities
Women were indicated as generally responsible for preparation and cooking (85%) of the meat, whereas men were responsible for slaughtering (88%), skinning (92%), and butchering (75%). Table 4 shows the farmers' reasons for cattle meat consumption behavior. The farmers cited prohibition by veterinary authorities (75.2%), religion (60.7%), and fear of contracting diseases (48.5%) as reasons for not consuming meat from cattle that were found dead. The reasons for eating meat from cattle that died of unknown causes were: Could not just afford to lose the carcass (88.3%), ‘slaughtered’ a moribund animal to salvage meat for consumption and/or sale (59.8%), long time since ate meat (57.1%), price of meat from local butchery was too high (52.7%), and had forgotten about anthrax (41.1%). When asked for the reasons for consuming meat from cattle suspected to have died of anthrax, 58.3% of the respondents indicated that they would go to the hospital once they developed skin lesions and the treatment was effective, 47.9% indicated that they could not just afford to lose the beast, while less than 15% indicated that they would dry the meat and then overcook it or cooking it with herbs to kill the germs (Table 4).
Discussion
Consistent with earlier observations on pet owners' (Pfukenyi et al. 2010) and dairy farmers' (Mosalagae et al. 2011) general knowledge on zoonoses in the country, most rural cattle owners knew rabies, anthrax, and brucellosis as zoonoses. Similar findings have been reported in Tanzania (Kambarage et al. 2003, Shirima et al. 2003, Swai et al. 2010). High awareness of anthrax (as confirmed by focus group discussions) and rabies by farmers could probably be attributed to periodic vaccination campaigns launched by the Department of Veterinary Services in the farming areas of the country. The other reason could be that the most named zoonoses cause great losses in animals in terms of morbidity and mortality and also pose a threat to public health. Diseases such as anthrax, brucellosis, and rabies are potentially devastating and impair production and reproduction in livestock and are also a danger to the health of the human population (Shirima et al. 2003).
In Zambia, the awareness of bTB was observed to be lower in low-prevalence settings compared to high-prevalence settings (Munyeme et al. 2010). Similarly, Brook and McLachlan (2006) also indicated that the level of disease awareness among farmers in North America is related to the prevalence of the disease. Findings of this study also concurred with this observation because a higher awareness of anthrax was noted in those districts with a higher outbreak incidence. However, despite being classified as a low-risk anthrax district, cattle owners in Chiredzi district were relatively aware of anthrax. Since 1967, the first reported cattle anthrax outbreak in the district was in 2005, but no human outbreaks have yet been reported. Between August and November, 2004, a massive outbreak of anthrax occurred in wildlife (Clegg et al. 2007) in the Malilangwe Wildlife Reserve located in Chiredzi district resulting in the death of almost all of the reserve's estimated 500 kudu (Tragelaphus strepsiceros). Cattle owners in Chiredzi district named the kudu as another animal species affected by anthrax. Hence, the recent wildlife and cattle anthrax outbreaks in the district have probably increased their awareness. In contrast, in Gwanda, another low-anthrax-risk district, cattle outbreaks were last reported in 1987 with no human outbreaks reported and this could probably account for their low awareness. Recent studies on bTB (de Garine-Wichatitsky et al. 2010, Gomo 2011), brucellosis (Gomo et al. 2011), and Rift Valley fever (de Garine-Wichatitsky et al. 2011) in cattle and wildlife at a wildlife/livestock interface in the southeast lowveld of Zimbabwe, where the Chiredzi district is located, could probably account for the high awareness of these diseases by cattle owners in this district.
Despite a high awareness of anthrax, its clinical features in animals and humans, routes of transmission, and preventive measures, results of the present study showed that people in rural communities would still consume carcasses suspected to have died of anthrax for various reasons. The importance of cattle to rural communities cannot be underestimated. They are a source of food and draught power, are a cash buffer, and provide organic fertilizers in addition to various uses in cultural and social roles. Currently, a cow in Zimbabwe sells at a market price of US $300 to US $500 and, hence, understandably poor rural families are reluctant to bury or burn the family cattle. Similar observations have been reported in Haiti (Peck and Fitzgerald 2007). The practice of salvaging meat from carcasses and slaughter of moribund cattle of unknown causes for household consumption and sale to the unsuspecting public contributes significantly to human anthrax outbreaks. In spite of religion forbidding consumption of meat from animals that die of unknown causes, the practice of slaughtering moribund animals makes belonging to a restrictive religion a nonprotective factor, as was also observed earlier by Gombe et al. (2010).
In countries where anthrax is endemic, 95–99% of all human cases are cutaneous (Swartz 2001), and during the present study most respondents mentioned skin lesions as indicative of human anthrax. Previous human outbreak studies in the country (Mwenye et al. 1996, Gombe et al. 2010) and elsewhere (Woods et al. 2004, Peck and Fitzgerald 2007) have shown the cutaneous form to be more prevalent than the inhalational and gastrointestinal forms; clinical signs such as diarrhea and vomiting were mentioned by a very low proportion of cattle owners. Cutaneous anthrax has been reported to have a very low case-fatality rate <1% when treated early and appropriately (Christie 1973). Low case-fatality rates have been reported in human anthrax outbreak investigations in the country (Mwenye et al. 1996, Takawira et al. 2004, Chirundu et al. 2009, Gombe et al. 2010). Other literature also confirms low case fatality rates with treatment (Lakshmi and Kumar 1992, Kumar et al. 2000, Woods et al. 2004). In the present study, a significant proportion of the respondents would send a sick family member who had consumed an anthrax carcass to the hospital rather than to the traditional healer. Similar findings have been reported in other studies (Opare et al. 2000). Because of the strong desire to salvage something from the animal coupled with the knowledge of treatment efficacy and at times having forgotten about anthrax, cattle owners are reluctant to bury/burn the carcass and expose themselves to anthrax infection. However, in Haiti (Peck and Fitzgerald 2007) and Turkey (Kaya et al. 2002), cutaneous anthrax was associated with significant morbidity and mortality due to asphyxiation from edema of the neck with tracheal compression and concurrent gastrointestinal anthrax.
As observed earlier in Ghana (Opare et al. 2000) and in Zimbabwe (Gombe et al. 2010), another reason for eating meat from anthrax-suspect carcasses is the belief that drying, overcooking, and cooking the meat with herbs will prevent anthrax. However, only a small proportion of the respondents had such a belief, and during focus group discussions most cattle owners overwhelmingly disagreed with such beliefs.
In support of earlier observations on cattle anthrax outbreaks in Zimbabwe (Chikerema et al. 2012), cattle owners indicated that anthrax is a hot-season disease. Focus group discussions revealed cattle owners' observations on an increased trend of cattle anthrax outbreaks, which they attributed to cessation of government-sponsored annual cattle vaccinations that used to be conducted by the government. Temporal distribution of the disease in cattle showed a reduction in outbreaks during the period 1982–1996, and this was attributed to mass annual vaccinations done during that period (Chikerema et al. 2012). However, a gradual increase in outbreaks was demonstrated from 1997 to 2006, and this was attributed to vaccinating in the face of an outbreak and also due to budgetary constraints faced by the country in the 2000s (Chikerema et al. 2012).
The results of this study demonstrated that anthrax awareness among cattle owners is high, but it differs depending on incidence of the disease in a particular area. Efficacy of human anthrax treatment, slaughtering of moribund cattle, selling meat from cattle that died of unknown causes to unsuspecting community members, and having forgotten about anthrax were found to be major reasons for consumption of anthrax-infected carcasses. This was further revealed during focus group discussions. By targeting some of the practices that encourage the transmission of the disease through public health education initiatives, human anthrax could be preventable in the studied areas. In many developed countries, human anthrax has been virtually eliminated because of effective control measures, including human and animal vaccination, veterinary supervision of animal slaughter, and quality control of animal products (Turnbull et al. 1999). Given that cattle owners would not consume meat from animals that died of unknown causes as a discouragement from veterinary officials, introducing veterinary-supervised meat inspection services is likely to have a positive impact in preventing human anthrax outbreaks. Also encouraging was the fact that awareness of animal vaccination and disposal of anthrax-infected carcasses was high. During focus group discussions, annual vaccination of cattle with cost recovery, introducing meat inspection services, prompt reporting of cattle deaths to the veterinary department, continued education, and awareness and collaboration between human and animal health workers were considered to be important in combating the disease. In addition, continued education on existing guidelines for the slaughter, disposal, and quarantine of domestic animals suspected to have anthrax and for those that have been exposed to anthrax would be beneficial. Furthermore, given the frequency of cutaneous anthrax, a simple intervention would be to wear gloves during high-risk activities of slaughtering and butchering livestock, as highlighted by human health workers during focus group discussions.
Footnotes
Acknowledgments
The authors would like to thank the Norwegian Council for Higher Education (NUFU) for financial support.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.