
Abstract
Malaria continues to be a major global public health problem with 3.3 billion people at risk in 106 endemic countries. Globally, over 1000 plants have been used as potential antimalarials in resource-poor settings due to fragile health-care systems and lack of accessibility and affordability of artemisinin-based combination therapies (ACTs). Although many believe that the use of medicinal plants that have folklore reputations for antimalarial properties is relatively safe, many herbs may be potentially toxic due to their intrinsic adverse side effects. Therefore, herbal-derived remedies require powerful and deep assessment of their pharmacological qualities to establish their mode of action, safety, quality, and efficacy. In addition, the evolution of drug resistance also demands new antimalarial agents. This can be achieved by forming a vibrant antimalarial discovery pipeline among all stakeholders, including traditional healers, ethnobotanists, scientists, entomologists, pharmacists, and research institutions, for the isolation and characterization of the bioactive compounds with the ultimate objective of finding novel modes of action antimalarial compounds that can be used to fight against drug-resistant malarial parasites.
Introduction
Malaria is a disease of poverty and inflicts a serious negative impact on the health and socioeconomic development among the poorest countries of the world (Karunamoorthi 2012a). Although malaria is both a preventable and curable illness, it remains one of the most important causes of maternal and childhood morbidity and mortality in sub-Saharan Africa, despite the availability of effective interventions (Karunamoorthi et al. 2010). At the moment, the battle against malaria is becoming a serious challenge due to the development of insecticide-resistant vectors, emergence of drug resistance, and lack of an effective reliable vaccine (Karunamoorthi and Sabesan 2009).
Although, insecticides are appropriately credited for much of the success of the first global eradication campaign carried out in the mid-20th century, careful review of malaria control and elimination efforts shows that treatment and prevention with drugs have also been essential components of all successful malaria elimination schemes (The malERA Consultative Group on Drugs 2011). Today, the chemotherapeutic arsenal for malaria treatment is limited to three main families of compounds—quinolines, antifolates, and artemisinin derivatives. Quinine was the first drug used successfully to treat malaria (Fig. 2A). However, this alkaloid has a high level of toxicity and a short pharmacological half-life, limiting its usage (Camargo et al. 2009, Muregi 2010). Currently, artemisinin-based combination treatment (ACT) is the therapy of choice for uncomplicated Plasmodium falciparum malaria in areas of widespread parasite choloroquine (CQ) resistance (Mackinnon and Marsh 2010)(Fig. 2B,C). However, failure to clear parasites after ACT treatment has recently been reported on the Cambodia–Thailand border, and genes related to artemisinin resistance have been discovered (Noed et al. 2008, Dondorp et al. 2009, Rodrigues et al. 2010, Saralamba et al. 2011).
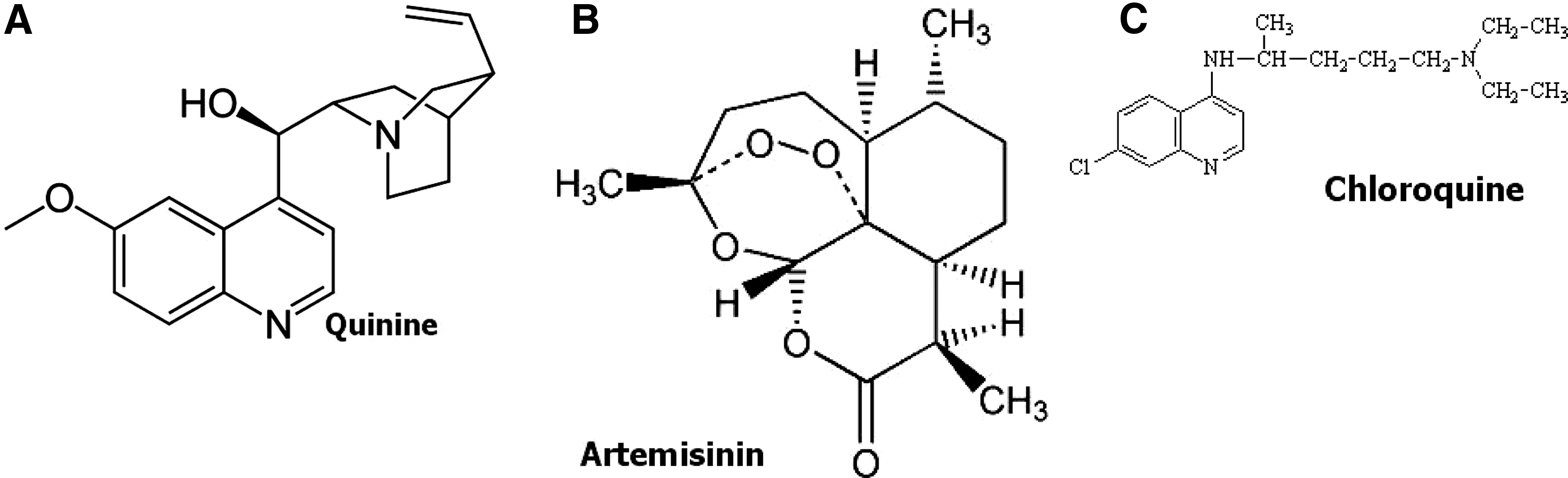
Chemical structures of quinine (
The cost of the new ACTs is significantly greater than that of the older classes of drugs such as chloroquine and the previously recommended first-line treatment, sulfadoxine+pyrimethamine (Cameron et al. 2011). Artesimin-based treatment costing about 50 cents to $2.50 per treatment course (sometimes more in the private sector) may not sound like a lot to pay for saving the life of a child, but it is often unaffordable to the rural poor, who are the most affected by malaria (Ngemenya et al. 2004). One full treatment course for a child takes at least 10% of the monthly income. On average, one child can have four malaria episodes per year and another four episodes that may be wrongly treated as malaria (Zirihi Guédé et al. 2010). Since 1996, no new class of antimalarial has been formulated (Ekland and Fidock 2008).
A recent study conducted in Uganda found that although ACTs are provided free of charge to patients, availability is a frequent problem, indicating that ACTs remain unaffordable and inaccessible to a large part of the population, many of whom living below the poverty line and predominantly in rural areas. In some districts, only 50% of public health facilities were found to have regular supplies of ACTs. Many Ugandans still have to seek ACTs treatment for malaria through the private sector, and it typically costs up to 30–60 times more than the older ineffective non-artemisinin–based medicine. In a typical family, the hard choice of spending their little disposable income on either basic needs like food and education or the treatment of malaria, the 11 days' average household income would be needed to purchase a single course of ACT for a 5-year-old child (MMV 2008, Cameron et al. 2011).
Traditional medicinal plants have been the main source of antimalarial drugs, with the two major drugs quinine and artemisinin being used worldwide for the treatment of malaria (Wright and Phillipson 1990, Thomson 1993). Quinine and artemisinin were obtained directly from the Peru tree Cinchona (Cinchona succiruba [Rubiaceae]) and Qinghao (Artemisia annua [Asteraceae]) plant, respectively, and were developed using plant-derived chemical structures as templates. Chemical modification of artemisinin has led to a series of potential antimalarial drugs (artemether, artesunate, and arteether) that are currently being used in combination with conventional drugs for treatment of malaria (Simon et al. 1990, Bai 1993, Nicholas 1994). These drugs clearly demonstrate that the plant kingdom is a rich warehouse of antimalarial products.
The use of combination chemotherapy is the current innovative strategy for controlling malarial disease; it involves the use of a short half-life–acting antimalarial agent of artemisinin drug in combination with a long half-life conventional drug, for example, artemether/lumifantrine and artesunate-melfoquine drugs (Nosten et al. 2000). The artemisinin drug (short half-life) kills the parasites and is excreted rapidly, resulting in the re-emergence of the parasites after a period of time. Therefore, its use in combination with longer half-life antimalarial drug results in achieving full eradication of the parasites and prevents the recrudescence that occurs with the use of artemisinin monotherapy (Walsh et al. 2007).
Currently, the drugs being used in combination with artemisinin drugs are the conventional drugs (lumifantrin, melfoquine, and amodiaquine), which have developed resistance to P. falciparum parasites when used in monotherapy. The use of the conventional drugs in combination therapy might not solve the problem of multidrug resistance of the parasites in the near future. There is an urgent need in discovering and developing new antimalarial drugs from traditional medicinal plants that can be used in combination therapy with artemisinin drugs to reduce the development of resistance and the occurrence of recrudescence (Kebenei et al. 2011). Because there is an urgent need for new, more affordable and accessible antimalarials possessing original modes of action, there is a revival of research interest in medicinal plants as sources of antimalarials.
This article reviews the current status of botanical screening efforts in Africa, Asia, the Middle East, Latin America, and beyond, as well as in vitro and clinical studies on antimalarial plants. It is also an attempt to document and preserve our traditional knowledge and to create a database of these plants that may pave way for policymakers with scientific consensus and researchers to formulate potential plant-based novel antimalarial drugs and traditional health care practices in the near future.
Importance of the Traditional System of Medicine
Despite recent scientific advancement and globalization, the system of traditional medicine (TM) and complementary/alternative medicine (CAM) is considered to be a primary health-care modality in resource-constrained health-care settings. Herbal medicinal system has been postulated and established through empirical observation and trial-and-error experiments since time immemorial to maintain good health and alleviate ailments and diseases. Even in the era of modern computational pharmacological approach, traditional medicinal plants are an important source, as well as a tool, for treating various ailments in developing countries (Fig. 1). The recent success of drug development from medicinal plants inspires and encourages many researchers to investigate and validate the uses of traditional medicinal plants (Karunamoorthi et al. 2012a,b).

The authour conversing with an Ethiopian key informant about the traditional antimalarial plants.
Over 70,000 angiosperm plants of the 300,000 angiosperm plants recorded so far in the world are used for medicinal purposes by people of different cultures throughout the world (Pushpangadan 2006). Because of this strong dependence on plants as medicines, ethnopharmacological studies have been conducted to determine their safety and efficiency and on the other hand to find out new active principles from plants (Bruhn and Holmested 1981).
Indeed, the induction of modern health-care services has posed an immense threat to indigenous health practices because of their potential and speedy therapeutic effects. Therefore, in the recent past, the traditional system of medicine has been disappearing, displaced, and undervalued by the people (Karunamoorthi et al. 2012b). Over the past three decades, the worldwide scientific community is extremely inclined toward our long-standing traditional system of medicine to explore the opportunities to formulate the novel phytotherapeutic agents (Karunamoorthi 2012b).
Important Antimalarial Plants
It has been estimated that the number of medicinal plants in the world varies between 30,000 and 75,000 (Pampona-Roger 2001). To date, there are 1277 plant species from 160 families listed in a database that have been actually used to treat malaria or fever (Willcox and Bodeker 2004). One of the most compelling sagas in the history of medicine and therapeutics is the emergence of the Peruvian bark (Cinchona) and also of the pharmacologically active substance derived from it, quinine. Its discovery involved exploration, exploitation, and secrecy (Lee 2002a).
Cinchona: The tree of fever
For centuries there was no specific treatment for malaria, and it was not until the 17th century that Spanish colonizers brought back from Peru the tree bark from which quinine was later extracted. In the 20th century, synthetic alternatives to quinine were developed (Butler et al. 2010). The discovery of chloroquine and its subsequent worldwide use against malaria in the 20th century produced one of the greatest public health advances ever achieved by a drug against an infectious disease (Wellems 2002). Quinine was used as a template for the synthesis of another antimalarial drug, chloroquine, in 1940.
Cinchona has been known in the West for almost 400 years (Lee 2002a). The first widely used antimalarial drug was quinine, a natural product extracted from the bark of the tree Cinchona calisaya. Synthetic derivatives of quinine, such as 8-aminoquinoline primaquine and 4-aminoquinoline chloroquine, can be traced back to the pioneering work of Ehrlich on Methylene Blue in the late 19th century. These drugs cause parasite death by blocking the polymerization of the toxic byproduct of hemoglobin degradation, heme, into insoluble and nontoxic pigment granules, resulting in cell lysis and parasite cell autodigestion (Olliaro and Yuthavong 1999).
History of chloroquine: An incredible chapter in the control of malaria
In 1820, quinine was isolated by the French scientists Pelletier and Caventou from the bark of the Cinchona spp. (Oliveira et al. 2009). Many physicians are familiar with the story of the Countess of Chinchón, wife of the Viceroy of Peru. It was claimed by Bado that she was cured of a certain ague by Cinchona bark sometime in the late 1620s or early 1630s (Jaramillo-Arango 1949), and thus the genus Cinchona is said to have been named after the Spanish Countess of Chinchón (Garnham 1966).
The first definite written account of the medicinal properties of the bark appears to be that by Fray Antonio de la Calancha, an Augustinian missionary, in 1633, who wrote an account of “the fever tree” which “grows in Loja, Peru, the bark of which when made into a powder and given as a beverage, cured the tertian fevers.” He also described its widespread use in Lima, the capital of Peru (Paredes-Borja 1946). In 1630, Juan Lopez, a missionary Jesuit, learned of the bark from Pedro Leiva, chieftain of the Malacatos tribe. He, and probably other Jesuits, took the knowledge of the bark and seeds back to their headquarters, St. Paul's at Lima, and then to Europe (Lee 2002a), where it was used for centuries to treat human malaria with efficacy.
In the 17th century, Rome had been a malarious zone, and many Catholic cardinals died of the “malignant ague” (or malaria) while attending the papal congregations in the Eternal City. By the time of the Conclave of 1655, during which Alexander VII was elected Pope, despite the availability of the bark, the “malignant ague” had not been recorded among the attendees, although Cardinal de Lugo died in 1660 due to the same malignant ague. Redi wrote some years later to the noted Jesuit Chircher that “the whole World owes a debt of gratitude to those Fathers of your most venerable Order who were the very first, much to their glory, to bring the bark to Europe.” We would now add “and in particular to de Lugo and Puccerini” (Redi 1966). Cinchona plantations were established in Java, and they were the source of quinine supply until the Second World War (Krettli et al. 2001).
In 1940, the antimalarial drug chloroquine was synthesized. The structure of quinine was established by Rabe in 1908, and its synthesis was accomplished in 1944 by Woodward and Doering (Oliveira et al. 2009). However, this synthetic production is by industrial means and is both complex and costly. It is currently derived by extraction from the Cinchona spp., which grows wild in South America and is cultivated in Java (Boulos et al. 1997). Chloroquine became the chief replacement for quinine during the Second World War, and until recently this was the only drug used for the treatment of malaria (Bharel et al. 1996, Krettli et al. 2001).
Chloroquine resistance: A great disaster in the fight against malaria
Chloroquine was close to the ideal antimalarial drug and was used for decades due to its high efficacy against all species of malaria parasites and its high tolerance (Krettli et al. 2001). However, P. falciparum, the most malignant of the four human malaria parasite species, showed foci of chloroquine resistance (CQR) in Southeast Asia and South America in the late 1950s, Papua New Guinea in the 1960s, and East Africa in the late 1970s. The steady and unremitting spread of CQR from these foci could only be met by a few alternative drugs, all of which were more expensive and encountered resistance problems of their own, or were less safe and more difficult to use than chloroquine itself (Wellems 2002). Over the last 30 years, the increasing prevalence of resistant strains of P. falciparum was the major factor responsible for the increase in mortality that occurred mainly in Africa (World Malaria Report 2005).
Artemisia (Qinghaosu or the sweet wormwood): The magical Chinese thyme
The genus Artemisia is a member of the family Compositae and comprises more than 300 species of annual, biennial, and perennial herbs (and shrubs) (Hyam and Pankhurst 1995). The plants have pinnate, divided, silky, hairy leaves, and these are often grey to white in color. The flowers are pendant and daisy-like but with no rays (Lee 2002b). A. annua has been known to the Chinese herbal practitioners for at least 1000 years, but was introduced into Western medicine only during the past 30 years. A major difference between Cinchona and Artemisia is the speed with which the active principle of the latter, artemisinin was isolated, synthesized, and then modified to produce effective therapeutic entities, largely due to the efficiency of modern chemical techniques (Lee 2002b). In 1972, the artemisinin compound was isolated from A. annua; this plant species has had many traditional uses in China for several millennia (Wright 2005a).
History of artemisinin derivatives
In China, around 2800 BC, Shen Nung was known as the “Divine Ploughman” (Huang 1998), and his works were later set down by an anonymous scribe in 101 BC. He codified rules for the cultivation of crops such as rice and millet, and having tested many herbs himself, described those that were poisonous and those that might be useful in medicine. Amongst the herbs described by the Ploughman was Qinghaosu, an agent effective in the treatment of fever (Lee 2002b).
In the 1960s, China was fighting a war in the jungles of North Vietnam, a malarious region, and signs of chloroquine resistance were manifested. Unknown to the rest of the world, the Chinese government established a large research program to find a replacement for chloroquine (Li 2007). In 1967, more than 500 scientists from more than 60 institutions, including chemists, pharmacologists, medical entomologists, and doctors, were recruited by the Chinese government for the antimalaria drug project known as Project 523 (Butler et al. 2010).
Mao Zedong had insisted that traditional Chinese medicine was a “great treasure house,” a phrase immortalized in “The Little Red Book” (Taylor 2005). The early studies of Qinghaosu established that this preparation was very active against malaria and that the active herb in the preparation was almost certainly A. annua (Qinghaosu Antimalaria Coordinating Research Group 1979, Li et al. 1982). Initial attempts to isolate the active principle or principles from the plant failed, but in 1971 success was achieved by extraction into diethyl ether at low temperature. The extract cured mice infected with Plasmodium berghei and, in 1972, further work culminated in the isolation of a crystalline compound called Qinghaosu (artemisinin) by the Chinese (Ying and Yu-Lin 1998).
Artemisinin chemical structure
The chemical structure of the active substance in this extract was identified in the late 1970s and was found, totally unexpectedly, to be sesquiterpene lactone peroxide. Pharmaceutical production of marketable drugs began in 1986. The WHO started to investigate artemisinin and its derivatives in the early 1990s and has promoted them on a large scale since 2004. Semisynthetic derivatives, including arteether, artemether, and sodium artesunate, are used increasingly more often (Wright 2005b). Although they are effective against CQ-resistant P. falciparum as single therapeutic agents, to minimize the risks of recrudescence and the development of resistance, a combination treatment with a second antimalarial drug is recommended (World Malaria Report 2005). The isolation of artemisin has inspired many research groups, since the early 1980s, to look for new plant-based antimalarial drugs to potentially contain malaria (Krettli et al. 2001). The first major hurdle in translating artemisinin into a global leader in malaria chemotherapy is its short half-life, which indicates the need for repeated doses and potential problems with treatment adherence and subsequent drug resistance (Awofeso 2011).
Ethnobotanical Studies on Traditional Antimalarial Plants
In light of this historic success and the fact that most indigenous people living in malaria endemic areas use traditional medicines to fight this disease, there is every possibility that ethnopharmacological approaches could lead to new antimalarial agents (Phillipson and Wright 1991). The term “ethnobotany” refers to all studies that are related to the reciprocal relationship between plants and traditional peoples. Through an understanding of the biological and cultural aspects of these relationships, ethnobotany seeks to understand the practical, material, symbolic, and identity-formed potential of plants for human populations. Ethnopharmacological investigation has been found to be one of the most reliable and meaningful approaches to potent new drug discovery (Fabricant and Farnsworth 2001). This approach is based on plants used in organized traditional medical systems, such as Ayurveda, Unani, and traditional Chinese medicine (Bannerman et al. 1975, Bannerman 1979), or from herbalism, folklore, and shamanism, which concentrate on an apprenticeship system of information passed down form generation to generation through a traditional healer or herbalist (Rastogi and Dhawan 1982). This system of medicine is widely practiced in the developing countries, in particular Southeast Asia, South America, and Africa.
Plant usage custom is a result of thousands of years of experience. This expertise has been passed down to many generations chiefly through word of mouth. This mode of conveying information may result in distortion or loss of indigenous knowledge and usage custom of plants. Therefore, right now the documentation and safeguarding of these practices are becoming crucial core issues (Karunamoorthi et al. 2009a, 2009b). As a result, there is a renewed worldwide interest to explore plant-based antimalarial products by exploiting traditional medicinal systems (Karunamoorthi and Tsehaye 2012). Numerous ethnobotanical surveys on traditional antimalarial plants have been conducted to preserve traditional knowledge and to identify the people's usage customs. The most relevant studies are listed in the Table 1 (Leaman et al. 1995, Marshall et al. 2000, Randrianarivelojosia et al. 2003, Bidla et al. 2004, Asase et al. 2005, Njoroge and Bussmann 2006, Ouattara et al. 2006, Alshawsh et al. 2007, Botsaris 2007, Odugbemi et al. 2007, Roumy et al. 2007, Tene et al. 2007, Adekunle 2008, Ajibesin et al. 2008, Hlaing et al. 2008, Ramalhete et al. 2008, Kantamreddi et al. 2009, Al-Adhroey et al. 2010, Jain and Singh 2010, Karou et al. 2011, Nadembega et al. 2011, Namsa et al. 2011, Karunamoorthi and Tsehaye 2012).
NA, related information not available.
The above-cited studies have specifically highlighted that the ethnopharmacological approach is the first phase for prioritizing plants as antimalarials and one of the most important and powerful tools for picking and choosing plants among the countless promising candidates to search future ideal antimalarial drugs. Although the use of crude extracts of various antimalarial plants is a custom of time immemorial, modern affordable potent antimalarial drugs can be formulated by conducting extensive investigation regarding their bioactivity, mode of action, pharmacotherapeutics, and toxicity after proper standardization and clinical trials. However, these ethnopharmacological surveys are commonly conducted among the rural poor in the resource-poor settings, where there is a lack of sophisticated equipment, laboratories, and skilled personnel to judge the bioactivities and efficacy of these traditional antimalarial plants. Therefore, further research must be carried out by international organizations like the WHO and collaboration with other agencies in the developed/developing countries with adequate funds to measure/improve their effectiveness as modern antimalarial agents.
In Vitro Antiplasmodial Activity of Traditional Medicinal Plants
In the developing countries, where malaria is endemic, people heavily rely on traditional medicine, the health-care modality for the treatment of malaria. However, scientific data to validate the antimalarial properties of these herbal remedies are scarce. Consequently, it is important that antimalarial medicinal plants are investigated to establish their efficacy and to determine their potential as sources of new antimalarial drugs (Ramalhete et al. 2008). Numerous studies have been undertaken across the globe to assess the in vitro antiplasmodial activity of traditional medicinal plants. The most important and relevant of these studies is summarized in Table 2 (Gessler et al. 1995, Awe et al. 1998, El-Tahir et al. 1999, Marshall et al. 2000, Ancolio et al. 2002, Muregi et al. 2004, Garavito et al. 2006, Ouattara et al. 2006, Muthaura et al. 2007, Nguyen-Pouplin et al. 2007, Hlaing et al. 2008, Wangchuk et al. 2010).
IC50, half-maximal inhibitory concentration; NA, not available.
The presence and/or quantities of bioactive compounds in plants are influenced by survival factors, including seasons, environment, plant part used, intraspecies variation, and plant age (Weenen et al. 1990). This may explain the discrepancies observed in in vitro activities of the plant parts reported. The major setback of in vitro studies is the antiplasmodial activity (half-maximal inhibitory concentration [IC50] μg/Ml]) of traditional medicinal plants, and in many cases it may not be comparable. The possible explanation could be that factors such as chemotypes, environmental parameters, harvesting, solvents, and storage conditions could collectively influence the plant metabolites prior to and following harvestings, which in turn, would be reflected in the bioactivity (Ramazani et al. 2010). The regions and periods of the year of plant collection are also known to play an important role in the variation of the type of compounds found in plants as well as their concentration.
Several pharmacologically active antimalarial compounds have been isolated from different plants used in ethnomedicine. Active compounds can be isolated from different parts of medicinal plants (such as leaves, roots, bark, fruits, or seeds) varying from species to species, and the active chemical ingredients of these parts can be different from one another (Van Wyk 2000, Pamplona-Roger 2001). One part of those plants may be quite toxic or useless and another may be quite harmless and useful. In traditional therapies, the whole plant is therefore rarely used for medicine. For example, the stem bark of Gardenia jovistonatis showed antiplasmodial activity against P. falciparum malaria, whereas no activity was found in the fruit of this species; the aerial part crude extract of Cassia species exhibits high antiplasmodial activity against different strains of P. falciparum (El-Tahir 1999).
With the problems of increasing levels of drug resistance and the difficulties in poor areas of being able to afford and access effective antimalarial drugs, traditional medicines could be an important and sustainable source of treatment (Willcox and Bodeker 2004). Over 1200 plant species are reportedly used for the treatment of malaria and fevers worldwide, and are potentially important sources of new antimalarial treatments (Willcox et al. 2004). According to Rukunga and Simons (2006), research on plant extracts carried out worldwide during the last decade covers over 300 extracts obtained from over 60 plant families. The antiplasmodial activity of these plants is assessed with various strains of the Plasmodium parasites.
A survey completed by WHO's Roll Back Malaria program showed that in Ghana, Mali, Nigeria, and Zambia, around 60% of all febrile cases in children, presumably due to malaria, are treated at home with herbal medicine (WHO 2002, 2004b). In many resource-poor settings, particularly in Africa, fever has been equated with malaria throughout most of the continent and the rest of the world. The assumption that fever equals malaria may be wrong as well as being a dangerous practice. It must be addressed effectively by developing appropriate communication strategy and health education campaigns in the malaria endemic settings.
Plants widely used as antimalarials by traditional healers are significantly more active in vitro and/or in vivo against Plasmodium spp. than plants that are not widely used, or not used at all, for the treatment of malaria (Brandão et al. 1985, Carvalho et al. 1991, Leaman et al. 1995, Krettli et al. 2001, Vigneron et al. 2005). The traditional antimalarial plants are a unique source of various types of compounds having diverse chemical structure; however, only limited amount of research has been carried out on the biological activity and plausible medicinal applications of these compounds, and therefore more extensive investigation is extremely important and inevitable to exploit their therapeutic utility to combat malaria effectively.
Clinical Studies: Clinical Safety and Efficacy of Herbal Preparations
Clinical observations on traditional remedies are feasible and useful. Some herbal remedies may be safe and effective for the treatment of malaria, as shown by many studies (Tsu 1947, CCRAS 1987, Guindo 1988, Boye 1989, Koita 1991, Yao-De et al. 1992, Valecha 2000, Benoit-Vical et al. 2003, Mueller et al. 2004) and reviewed by Willcox and Bodeker (2004). A recent study examined the efficacy and safety of an infusion of fresh Vernonia leaves for the treatment of uncomplicated malaria in patients aged 12 years and over. It found adequate clinical response (ACR) at day 14 in 67% of cases. However, complete parasite clearance occurred in only 32% of those with ACR, and of these, recrudescence occurred in 71%; there was no evidence of significant side effects or toxicity from the medication (Challand and Willcox 2009).
Patients being treated for malaria at an herbalists' clinic in southwestern Uganda were followed up, and their response to a particular herb, “AM,” was monitored. Eighty-eight patients were enrolled; 72 were followed up for at least 2 days. Nearly 50% experienced minor side effects. Although complete parasite clearance was achieved in only one case, the geometric mean of parasite counts had declined significantly by day 7. There was also a marked symptomatic improvement in 17 of the 19 patients (Willcox 1999).
A prospective, dose-escalating, quasi-experimental clinical trial was conducted with a traditional healer using a decoction of Argemone mexicana for the treatment of malaria in Mali. The remedy was prescribed in three regimens: Once daily for 3 days (group A, n=23); twice daily for 7 days (group B, n=40); and four times daily for the first 4 days followed by twice daily for 3 days (group C, n=17). Thus, 80 patients were included, of whom 80% were aged <5 years and 25% were aged <1 year. All presented to the traditional healer with symptoms of malaria and had a P. falciparum parasitemia >2000/μL but no signs of severe malaria. The proportions of ACR at day 14 were 35%, 73%, and 65% in groups A, B, and C, respectively (p=0.011). Very few patients had complete parasite clearance, but at day 14, 67% of patients with ACR had a parasitemia <2000/μL (Willcox et al. 2007).
Current Development Efforts in Developing Plant-Based New Antimalarials
In malaria-endemic countries, traditional medicinal plants are frequently used to treat malaria. The analysis of traditional medicines that are employed for treatment of malaria represents a potential for the discovery of lead molecules and hence for further development as potential antimalarial drugs (Muthaura et al. 2007). New drugs are required to combat the emergence of antimalarials resistance. The main goal of ethnopharmacology is to discover novel plant-derived compounds based on the indigenous use of medicinal plants that can be developed into new pharmaceuticals. Historically, plants have proven to be a major source of drugs (Newman et al. 2003), with two of the most widely used antimalarials originating from plants. The quinoline-based antimalarials are modeled on quinine, derived from the bark of the Peruvian Cinchona tree, and the endoperoxide-based antimalarials originated from artemisinin, first isolated from the Chinese herbal medicine A. annua (Camacho et al. 2000).
In light of this historic success, there is every possibility that ethnopharmacological approaches could lead to new antimalarial agents (Phillipson and Wright 1991). ACTs have now been adopted globally as the first line of treatment. Together with mosquito-control measures such as insecticide-treated bed nets, ACTs have driven down malaria rates across sub-Saharan Africa (Eastman and Fidock 2009). The emergence and spread of drug-resistant malaria parasites is the major threat to effective malaria control. Experience has shown that resistance eventually curtails the life span of antimalarial drugs. If measures are not applied to contain resistance, the investment put into the development of new drugs will be squandered (Olliaro and Taylor 2003).
The discovery and development of new antimalarials are at a crossroads. Fixed-dose artemisinin combination therapy is now being used to treat a hundred million children each year, with a cost as low as 30 cents per child, and with cure rates of over 95%. They are also relatively safe, often with no serious adverse events seen in phase III trials of several thousand patients. However, in the long term, there will always be a need for new therapies, no matter how carefully the current medicines are used, and there is also the constant threat of resistance (Wells 2011). This is an early warning sign that new classes of antimalarials are needed and are an urgent priority. It takes at least 10 years to move a molecule from late in the discovery phase to completion of clinical trials. Herbal medicinal products carry one strategic advantage–in several cases we know that there is an activity in patients. Once the active ingredients are identified, it is likely that medicinal chemistry will be needed to optimize it for clinical use (Wells 2011).
Even though currently ACT serves a pivotal role to combat malaria, they are mostly inaccessible and unaffordable in the resource-limited settings. Besides, there are signs of resistance to artemisinins and this has led to exploration for the low-cost and easily accessible plant species as a potential source of antimalarials in the near future (Karunamoorthi and Tsehaye 2012). However, the new antimalarial drugs must meet the requirements of rapid efficacy, minimal toxicity, and low cost.
The Role African or Asian Network on Drugs and Diagnostic Innovation
The African Network for Drugs and Diagnostics Innovation (ANDI) was conceived and launched as a concept at Abuja in 2008 by the WHO through TDR and its African and East Mediterranean Regional Offices, several African institutions, policy makers, Africans in the Diaspora, the African Development Bank (AfDB), and other stakeholders. ANDI intends to develop and fund a portfolio of collaborative network projects and leverage existing capacity in Africa in a manner that will support capacity and infrastructural development for product research, development, and delivery. The key objective is to discover, develop, and deliver affordable new drugs, vaccines, diagnostics, and other health products (including those based upon natural products and traditional medicines) to fight and prevent diseases that disproportionately affect the African continent (Addae-Mensah et al. 2011).
It is known that up to 80% of African populations use traditional medicines to address their health issues (WHO 2002). In spite of this, the biodiversity of Africa has yielded few examples of standardized phytomedicines, and only limited systematic analysis of available medicinal plants has been undertaken. The development of traditional medicines should not be seen as the answer to providing cheap treatments to poor populations. But it is important that such medicines are given the same scrutiny as any other pharmaceutical to ensure the protection of patients from any major adverse event and also to ensure the benefits of optimal efficacy. Research in support of the use of traditional medicines and natural products in disease prevention and control should also receive attention, for example, vector control (Addae-Mensah et al. 2011).
Major Challenges and Opportunities in Developing New Antimalarials
Continued and sustainable improvements in antimalarial medicines through focused research and development are essential for the world's future ability to treat and control malaria. Unfortunately, malaria is a disease of poverty, and, despite a wealth of scientific knowledge, there is insufficient market incentive to generate the competitive, business-driven industrial antimalarial drug research and development that is normally needed to deliver new products (Ridley 2002).
The challenge of any drug discovery effort is to identify and develop compounds with properties that are predictive of good efficacy and safety in humans. For malaria, additional hurdles that need to be overcome include the selection of compounds that are reasonably cheap to produce and that are effective against drug-resistant strains. The potential of a candidate compound to be used by the most vulnerable populations (young children and pregnant women) in disease-endemic countries also needs to be assessed as the candidate moves into development. In addition to being effective against uncomplicated P. falciparum malaria, compounds that can be easily formulated for severe disease (that is, amenable to parenteral administration) bring an added benefit, as do compounds that work against P. vivax (Ridley 2002, Nwaka and Ridley 2003). Their ultimate success depends on the intrinsic qualities of the molecule, as well as how the development of the drug is planned and implemented (Fidock et al. 2004). Apart from these, further challenges and issues are discussed below.
Imprecise diagnosis and treatment
The WHO Global Malaria Programme recommended that all suspected cases of malaria receive an appropriate diagnostic test prior to treatment. But in malaria-endemic countries, economic and logistic reasons force entire populations to rely on clinical diagnosis. Each traditional system of medicine having its own unique diagnostic procedure, the diagnosis is involves examination of patient, reviewing physical signs such as complexions, color, smell, texture of the tongue, postures of the patient, and the patient's personal lifestyle. Unfortunately, the diagnoses in traditional healer systems of malaria are often error-prone as well as not precise. This remains one of the major setbacks to advocate the plant-based therapies for the treatment of malaria.
Randomized clinical trials
Although traditional medicine is widely used to treat malaria, and is often more available and affordable than Western medicine, it is not without limitations. First, there are few clinical data on safety and efficacy. Second, there is no consensus, even among traditional healers, on the selection of plants, preparations, and dosages that are the most effective. Third, the concentration of active ingredients in a plant species varies considerably, depending on several factors. However, these limitations are all remediable through research (Willcox and Bodeker 2004). Nevertheless, better evidence from randomized clinical trials is needed before herbal remedies can be recommended on a large scale. In remote settings with poor resources where modern antimalarials are not steadily available, research can provide an evidence base for traditional medicine to inform local treatment choices (Willcox and Bodeker 2004).
Lack of standardization on quality, efficacy, and safety
The identity, authenticity, and quality of crude plants are often uncertain and difficult to assess (Morris 1998). Traditional medicines are currently undergoing scrutiny to evaluate their effectiveness and to monitor their adverse effects (Normile 2003, Hsieh et al. 2006). The active ingredients used in many traditional medicines are potentially toxic, often containing dangerous elements, and they may include heavy metals (Garnier and Poupon 2006, Palombo 2006). Even the use of ineffective nontoxic remedies can be harmful if they delay effective treatment. For instance, fears have been expressed that, in Nigeria, witchcraft and traditional remedies of unknown efficacy are widely employed as treatments for malaria to delay the access to modern medicines of proven effectiveness (Okeke et al. 2006).
There are still certain inherent problems with the medicinal plants. A good number of medicinal plants are cross-pollinated, and therefore there are a large number of genetic variants in the population, which accounts for the variation in chemical composition. Even the genetically similar plants behave differentially in different ecological, edaphic, and climatic conditions, leading to differences in the chemical composition and ultimately pharmacological action (Pushpangadan 2006). The medicinal plants may grow in areas of similar climatic conditions and soil, but the quality and composition of pharmacological components may be inconsistent in each and every harvest. In the case of A. annua, the concentration of artemisinin peaks around the time of flowering, although in some cases this may be just before flowering and in other cases during full flowering (Ferreira et al. 1995, Laughlin et al. 2002). The artemisinin concentration peaks at a slightly different time in different areas (Chang and But 1986).
Generally, the majority of the traditional healers treat their patients by administering various herbal medicines based on their previous knowledge and experience. However, the incorrect preparations, dosage, harmful side effects, and the end organ outcome are often ambiguous and unknown, and there could be potential risk if these medicines are not administered properly and appropriately (Robinson and Zhang 2011). The idea that just because traditional medicine products come from natural sources they are completely safe is dangerously false (Calixto 2000). Not everything that is natural is safe; traditional medicine products must be used judiciously and as indicated, just like any other medication, and with awareness of potential herb–herb and herb–drug interactions. The risks are relatively small when traditional medicines are used correctly, but they are still there and consumer understanding is generally low (Zhang et al. 2008). While acknowledging that all traditional medicines must be subject to evaluation of safety, therapeutic efficacy, quality control, and pharmacovigilance, according to prescribed criteria, we should, in conducting such evaluations, recognize the unique historical development of these products (WHO 2004a,b).
Lack of appropriate technology
In 1971, laboratory experiments verified the activity of extracts of a plant A. annua against Plasmodium berghei, using a mouse model of malaria (Schuster 2001). This discovery has since revolutionized the treatment of malaria around the world, but with little recognition for the traditional medicine practitioners of the African region who have used Artemisia spp. for centuries, but who lacked the technology or financing to prove its efficacy against malaria in a laboratory (Robinson and Zhang 2011).
The need for further research and development
Over the past several decades, numerous plants have been screened for their antimalarial bioactive compounds; however, this is a part of the minor-level research of the drug development program. Therefore, in-depth research is required to assess the antimalarial properties of such plants in terms of pharmacological investigation about their bioavailability, half-life, and interactions, etc. Furthermore, some of the plants may have potential antimalarial properties with a cytotoxic nature that may demand further extensive research.
Lack of accessibility of ACTs in the rural settings
Globally, many malaria-endemic countries have ACT-free treatment programs. However, these facilities are not reachable for the rural poor and those are living in the remote areas. For example, in 2005 more than half of the population of Ethiopia lived more than 10 km from health services (Bilal et al. 2010). These rural people must walk/travel a very long distance to reach the nearest health facility to access modern health-care facilities. Unfortunately, in malaria-endemic countries, many villages are not approachable by means of road. Even if they are reached, only a limited number of health facilities are found to have regular supplies of ACTs. From my personal observation in Ethiopia and India, of course, plant-based therapies are expensive in the urban areas but it is cheaper or inexpensive in the rural areas. I have witnessed in Ethiopia, where even the rural illiterate poor women prepare plant-based antimalarial therapy by using nearby freely available plants for their own children, who suffer from fever presumed as malaria. However, if the people consult a local traditional healer for herbal therapy, it may often be relatively expensive. It is purely because of the lack of accessibility and affordability toward effective antimalarial like ACTs. Therefore, the provision and scaling up ACTs along with rapid diagnostic tests (RDTs) at the village level must be implemented.
Conclusions
Traditional medicinal plants (TMPs) have been the main source of potential antimalarial drugs like quinine and artemisinin. Worldwide, over 1000 plant species have been used as a source of traditional antimalarial phytotherapy for many centuries. In the future, plant-derived compounds will still be an essential aspect of the therapeutic array of antimalarials. However their clinical efficacy, quality, and safety are a matter of grave concern. Because, in resource-poor settings, although traditional antimalarial therapy is certainly not a desirable one due to its safety and efficacy checkpoints, it is the accessible or possible one, because of remoteness, lack of affordability, and accessibility to ACTs. Therefore, the existing major issues, challenges, and risks must be addressed effectively and immediately by the public health experts for the betterment of traditional herbal systems of medicine and to develop potential antimalarial drugs. A vibrant antimalarial discovery pipeline must be formed by making collaboration among all stakeholders, like traditional healers, ethnobotanists, scientists, entomologists, pharmacists, and research institutions, to identify lead compounds and to develop usable antimalarials in the near future.
Footnotes
Acknowledgments
I would like to thank Mrs. Melita Prakash for her sincere assistance in editing this manuscript. My last, but not the least, heartfelt thanks go to my colleagues of our Department of Environmental Health Science, College Public Health and Medicine, Jimma University, Jimma, Ethiopia, for their kind support and cooperation.
Author Disclosure Statement
No competing financial interests exist.