
Abstract
Human brucellosis is a disease of protean manifestations, and has been implicated in complications and focal disease in many human organ systems. However, little is collectively known about the background, the course, the clinical characteristics, the diagnostic issues raised, and the short- and long-term therapeutic approaches in patients with aortic involvement as a complication of brucellosis. With the aim to glean from the literature useful information to better understand and manage this complication, a computerized search without language restriction was conducted using PubMed and SCOPUS. An article was considered eligible for inclusion in the systematic review if it reported data on patients with involvement of the aorta due to a Brucella infection. The epidemiologic and clinical characteristics of 44 cases of brucellar aortic involvement found through the systematic review of the literature were analyzed together with those of two new cases that we treated in the recent past. This complication involved the ascending thoracic aorta in 18 cases (in 16 of them as a consequence of brucellar endocarditis), and the descending thoracic aorta or the abdominal aorta in the remaining 30 cases. In the latter it was associated with spondylodiscitis of the lumbar spine in 13 cases. History of or symptoms indicative of brucellosis were not universally present. Brucellar aortic involvement represents a possibly underdiagnosed and underreported complication with major morbidity and mortality potential. Experience with novel invasive therapeutic approaches remains limited. Early suspicion through detailed history and diagnosis, aided by advances in aortic imaging, would allow for better planning of therapeutic interventions.
Introduction
Human brucellosis is a disease of protean manifestations, and has been implicated in focal complications of many human organ systems. Osteoarticular disease is the most common complication observed, while endocarditis, although rare, remains the principal cause of mortality, usually involving the aortic valve and generally requiring immediate surgical valve replacement (Pappas et al. 2005). Aortic or peripheral arterial involvement is an even rarer brucellosis complication (Adaletli et al. 2006). Little is collectively known about the background, the course, the clinical characteristics, the diagnostic issues raised, and the short- and long-term therapeutic approaches in patients with brucellar aortic involvement.
In this article the epidemiologic and clinical characteristics of all cases of brucellar aortic involvement found through a systematic review of the literature are analyzed, together with those of two new cases that we treated in the recent past.
Literature Review
For the review of historical published cases, a computerized search without language restriction was conducted using PubMed and SCOPUS. The search was performed combining the terms (aneurysm OR mycotic OR pseudo-aneurysm OR aorta OR aortitis) AND (Brucella OR brucellosis OR spondylitis) for the period between January 1950 and December 2011. Furthermore, all references listed were hand-searched for other relevant articles, and a citation tracker was used to identify any other relevant literature. Published articles written in languages other than English, French, or Italian were further reviewed by a native speaker of the relevant language. The selected articles were reviewed by two independent authors (A.C. and S.L.), and judged on their relevant contribution to the subject of this study. An article was considered eligible for inclusion in the systematic review if it reported data on patients with involvement of the aorta due to a Brucella infection. Cases of stand-alone aortic valve Brucella endocarditis were not included in this study. Cases of aortic valve Brucella endocarditis were included in this study if concomitant infection of any segment of the aorta was present. A flow chart summarizing the literature research approach is reported in Figure 1.
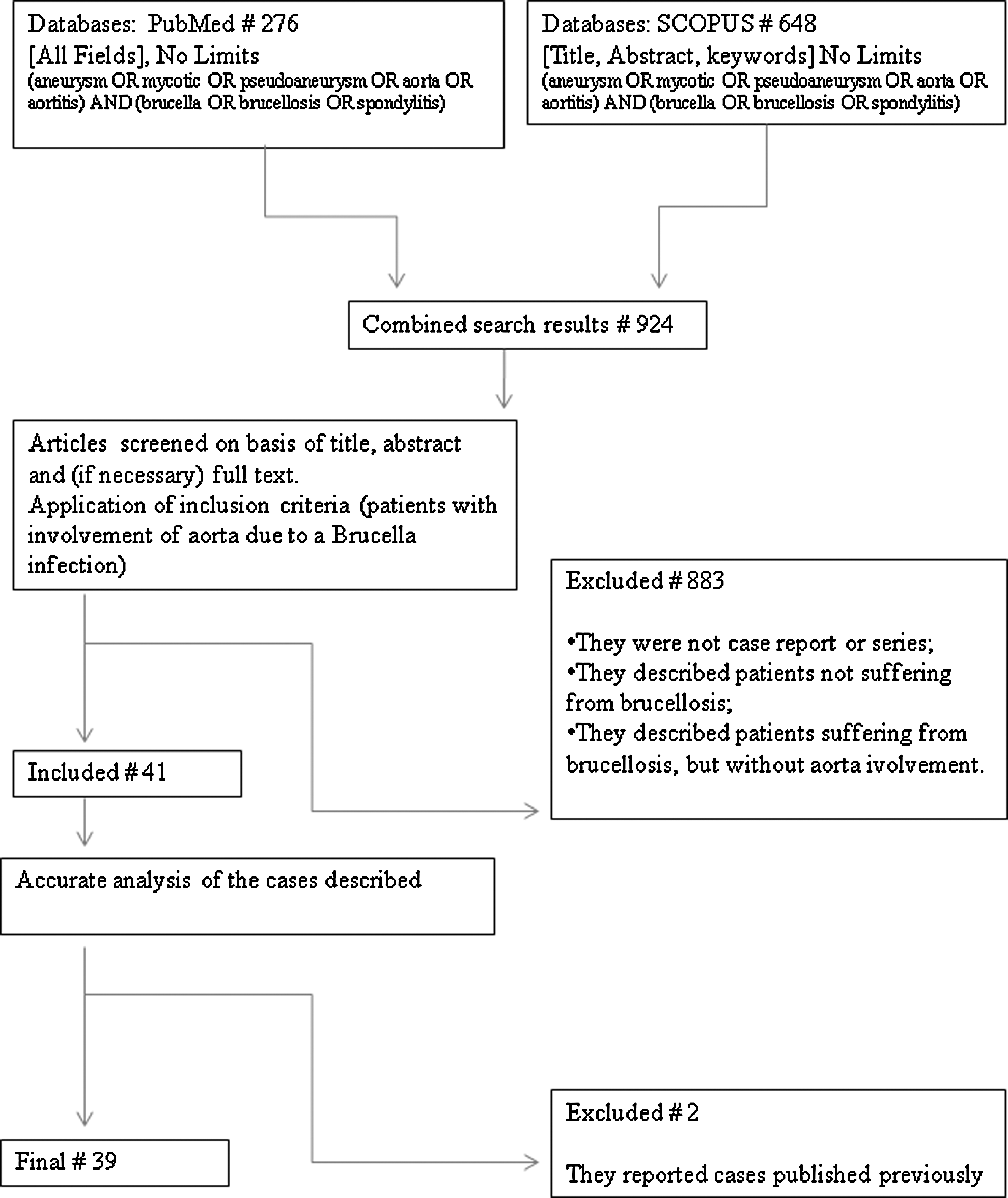
Flow chart summarizing the literature research approach (#=number of articles).
Epidemiology and Risk Factors
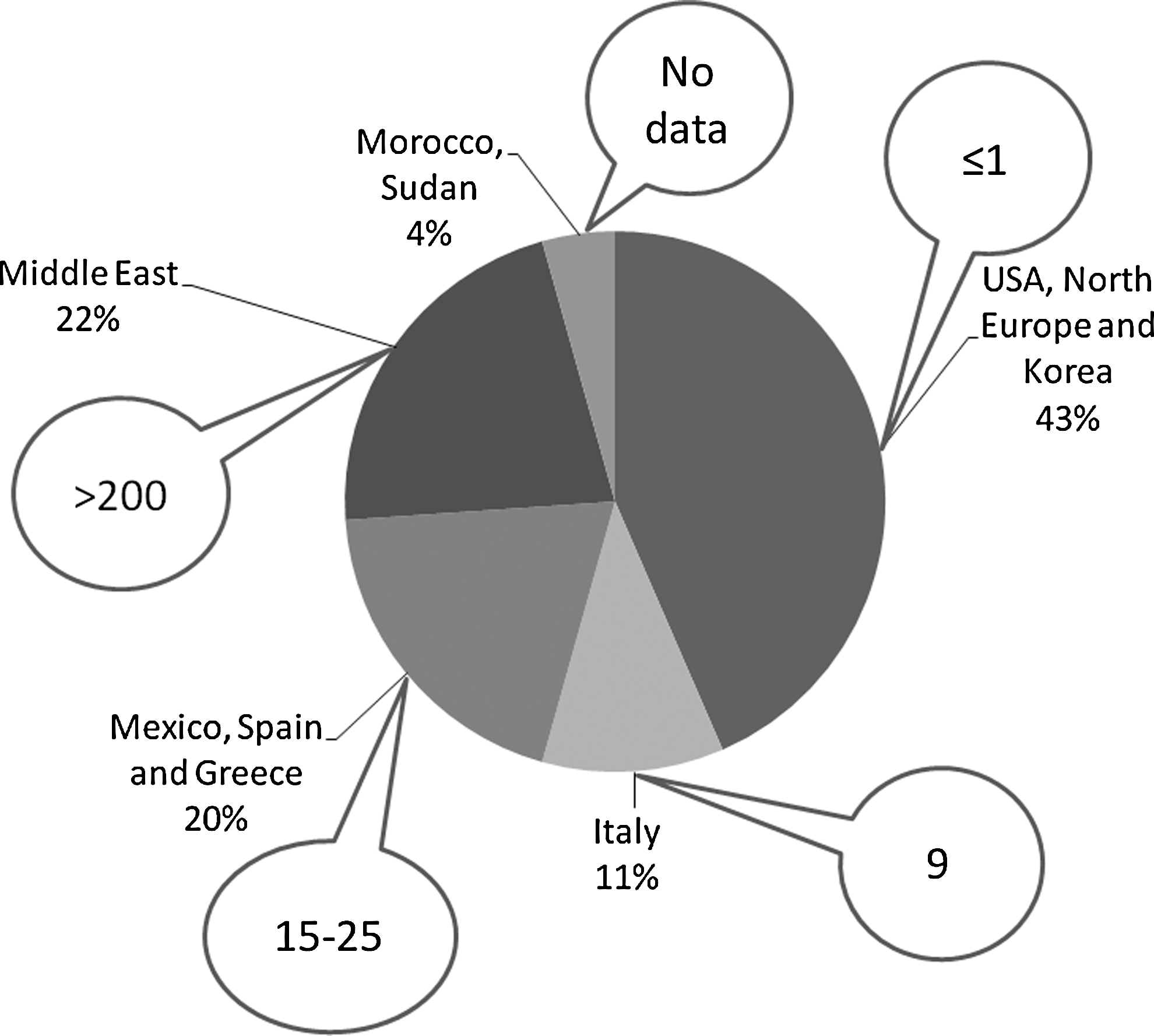
Up to now, 46 cases of brucellar aortic involvement have been detailed in the published literature, either as single case reports or as small surveys from a single center (Hart et al. 1951; Peery and Belter 1960; Bennett 1967; Golden et al. 1970; Quilichini et al. 1974; Cros et al. 1975; Gillet et al. 1976; Fudge et al. 1977; Sava et al. 1977; Colonna et al. 1978; Cueto Garcia et al. 1983; Gillet et al. 1983; Aguado et al. 1987; al Kasab et al. 1990; Pressl et al. 1990; Bergeron et al. 1992; Kumar et al. 1993; Gross et al. 1994; Sanchez-Gonzalez et al. 1996; Yee et al. 1996; Blain et al. 1997; Cano Trigueros et al. 1997; Peláez Fernández et al. 1999; Shehata et al. 2001; Rousie et al. 2004; Alhyari et al. 2005; Quaniers et al. 2005; Tsioufis et al. 2006; Biyik et al. 2007; Bul et al. 2007; Kusztal et al. 2007; Park et al. 2007; Kokkinis et al. 2008; Wolff et al. 2009; Ahmed et al. 2010; Bakhos et al. 2010; Jun Park et al. 2010; Kwon et al. 2010; Sasmazel et al. 2010; Amirghofran et al. 2011; Benedetto et al. 2011). Two cases were reported twice (Gillet et al. 1976; Sava et al. 1977), and for the purpose of this review are only considered once. Two new cases we recently observed were also considered, for a total of 46 cases. All the tracts of the aorta were involved. Data regarding the epidemiological and clinical characteristics and outcomes (historical and novel), of the patients are summarized in Table 1. About half of the cases (20/46) were from Mediterranean countries. Other regions represented include northern Europe, the U.S., Mexico, Saudi Arabia, Jordan, Iran, Kuwait, Korea, and Sudan; one patient residing in The Netherlands acquired brucellosis while on holiday in Syria, while a resident of Belgium contracted brucellosis while on holiday in Sicily (Figs. 2 and 3). All but an 11-year-old boy were adults, with mean and median ages of 54.2 and 59 years, respectively (range 23–80 years), and 41/46 were males. The mean age of the patients with abdominal or descending thoracic involvement was significantly higher than that of patients with ascending aortic involvement (65.5 and 42.5 years, respectively; p=0.0006). This difference could be explained by the high prevalence of abdominal aortic comorbidity in the elderly. Possible occupational exposure was reported in 20 cases; in the other cases infection was probably acquired through consumption of unpasteurized dairy products.
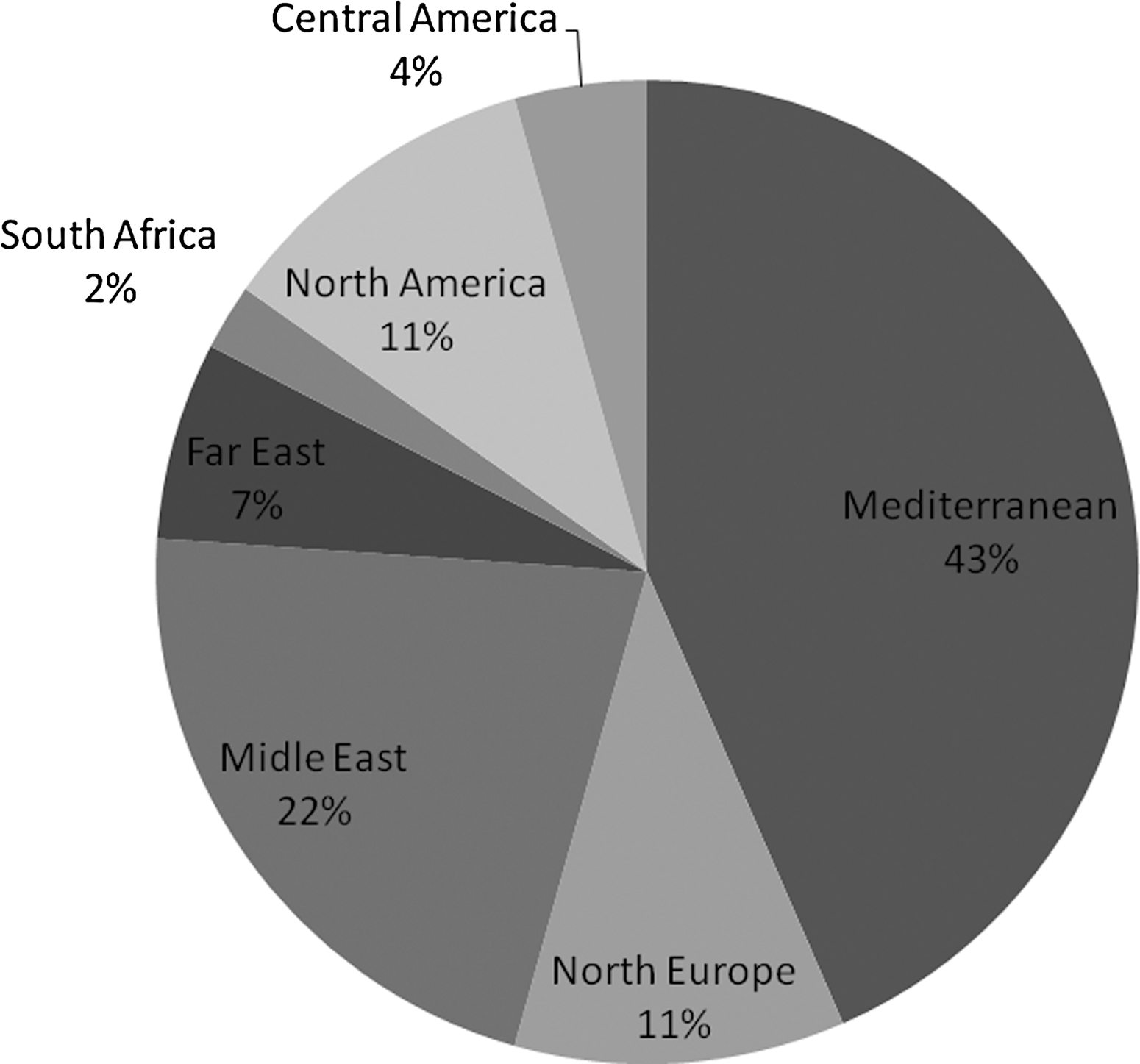
Geographic origin of the cases of brucellar aortic involvement.
(
CT, computed tomography; Chl, chloramphenicol; Cipro, ciprofloxacin; FYROM, former Yugoslav Republic of Macedonia; CTX, cotrimoxazole; Dox, doxycycline; F, female; IV, intravenous; mo, months; NA, not available; Neg, negative, NR not reported; M, male; MOF, multi-organ failure; PME, post-mortem examination, PO, per os (oral); Pos, positive; PTFE, polytetrafluoroethylene prosthesis; Rif, rifampin; Strepto, streptomycin.
Direct fluorescence was positive for Brucella.
Acquired on vacation in Sicily (Italy).
Brucella polymerase chain reaction-positive.
UMIME #1, UMIME #2, UMIME #3 are three cases we treated at University of Messina. The first one was published in 2011.
This complication could be more common than these cases show. In fact, the analysis of the origin of the historical cases shows that most of them arise from European Mediterranean countries, which although generally endemic for brucellosis, are hardly a significant portion of worldwide human brucellosis cases (Pappas et al. 2006). Hyperendemic regions such as the Near East/Middle East and Latin America are under-represented as areas of origin of patients with aortic complications related to brucellosis (Fig. 3). The probable explanation for this is that the developing world has limited access to scientific publications due to language, scientific background, and financial barriers. So it is likely that numerous cases went undiagnosed in the developing world, thus vastly underestimating the true incidence of the disease. One can hardly imagine the use of aortography to allow a proper diagnosis 40 years ago in the developing world. Thus many more cases may have remain undetected, even in rural areas of the developed world. For the same reasons one can imagine that many cases were lost due to the absence of post-mortem histology. It is not common for surgeons to consider brucellosis as the etiology of an aneurysm rupture, and thus specific forensic testing may not have been systematically performed.
Pathological Findings and Pathogenesis
The abdominal aorta was involved in 26 cases, the descending thoracic aorta in 5 cases, and the ascending thoracic aorta in 18 cases, 16 of whom had concomitant aortic valve endocarditis. Endocarditis was not found/reported in any of the patients with aortic involvement localized outside the ascending aorta.
Concomitant involvement of the abdominal and thoracic aorta was observed in three cases (Fudge et al. 1977; Peláez Fernández et al. 1999; Kusztal et al. 2007), while multiple aneurysms were present in two cases (Fudge et al. 1977; Quaniers et al. 2005). In one case a mesenteric artery aneurysm was contextually diagnosed (Fudge et al. 1977), while in three cases the aortic aneurysmal dilatation extended to the iliac artery, causing further aneurysmal involvement or thrombosis (Bennett 1967; Yee et al. 1996; UNIME #2).
In most cases aortic involvement was described as a mycotic aneurysm. In 6 cases it was a pseudo-aneurysm (Gillet et al. 1983; Bergeron et al. 1992; Cano Trigueros et al. 1997; Bul et al. 2007; Kwon et al. 2010; Benedetto et al. 2011), a dissecting aneurysm in four cases (Colonna and Cristallo 1978; Cueto Garcia et al. 1983; Biyik et al. 2007; Kusztal et al. 2007; Amirghofran et al. 2011), an intramural hematoma in one case (Bakhos et al. 2010), an ulcerative process in two cases, an aortic root abscess in seven cases (al-Kasab et al. 1988; Alhyari et al. 2005; Biyik et al. 2007; Ahmed et al. 2010; Amirghofran et al. 2011), and as thrombosis in one case (Sanchez-Gonzalez et al. 1996; Fig. 4).
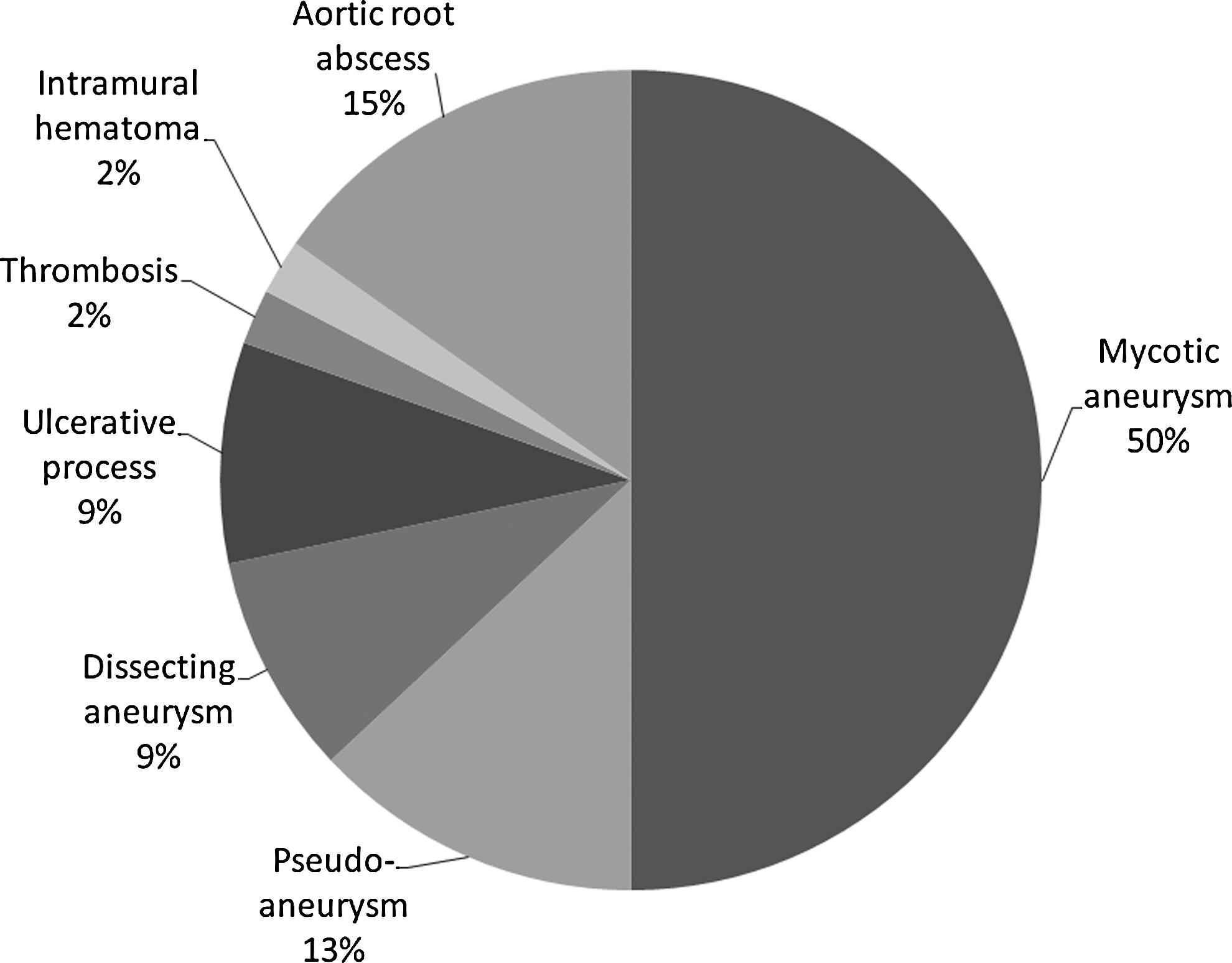
Types of aortic involvement.
Among the 23 thoracic aneurysm cases 5 were ruptured (Hart et al. 1951; Peery et al. 1960; Blain et al. 1997; Peláez Fernández et al. 1999; Bakhos et al. 2010); two fistulized into the right ventricle, two fistulized into the Valsalva sinuses (Hart et al. 1951; Peery and Belter 1960), two caused an aortobronchial fistula (Blain et al. 1997; Bakhos et al. 2010), and one an aortoesophageal fistula (Bakhos et al. 2010). Of the 26 cases with abdominal aorta involvement, a contained rupture was described in 15 cases, while aortoduodenal fistula formation was described in a single case (Cano Trigueros et al. 1997). Concomitant spondylodiscitis was diagnosed in 13 cases, 12 of which occurred in patients with abdominal aortic aneurysms. In all cases, spondylodiscitis involved 2 vertebral bodies and was located between L2 and S1. Figure 5 shows the localization of aortic involvement and the relationships with endocarditis and spondylodiscitis. Figure 6 shows the radiological findings of case UNIME #3. Atherosclerotic plaques were found in nine cases. Other comorbidities included congenital heart disease, history of rheumatic fever, dyslipidemia, diabetes mellitus, hypertension, heavy smoking, heart failure history, and steroid use. Of interest is a single case in whom histological findings were consistent with syphilitic aortitis for which brucellosis served as a complicating factor (Peery and Belter 1960).
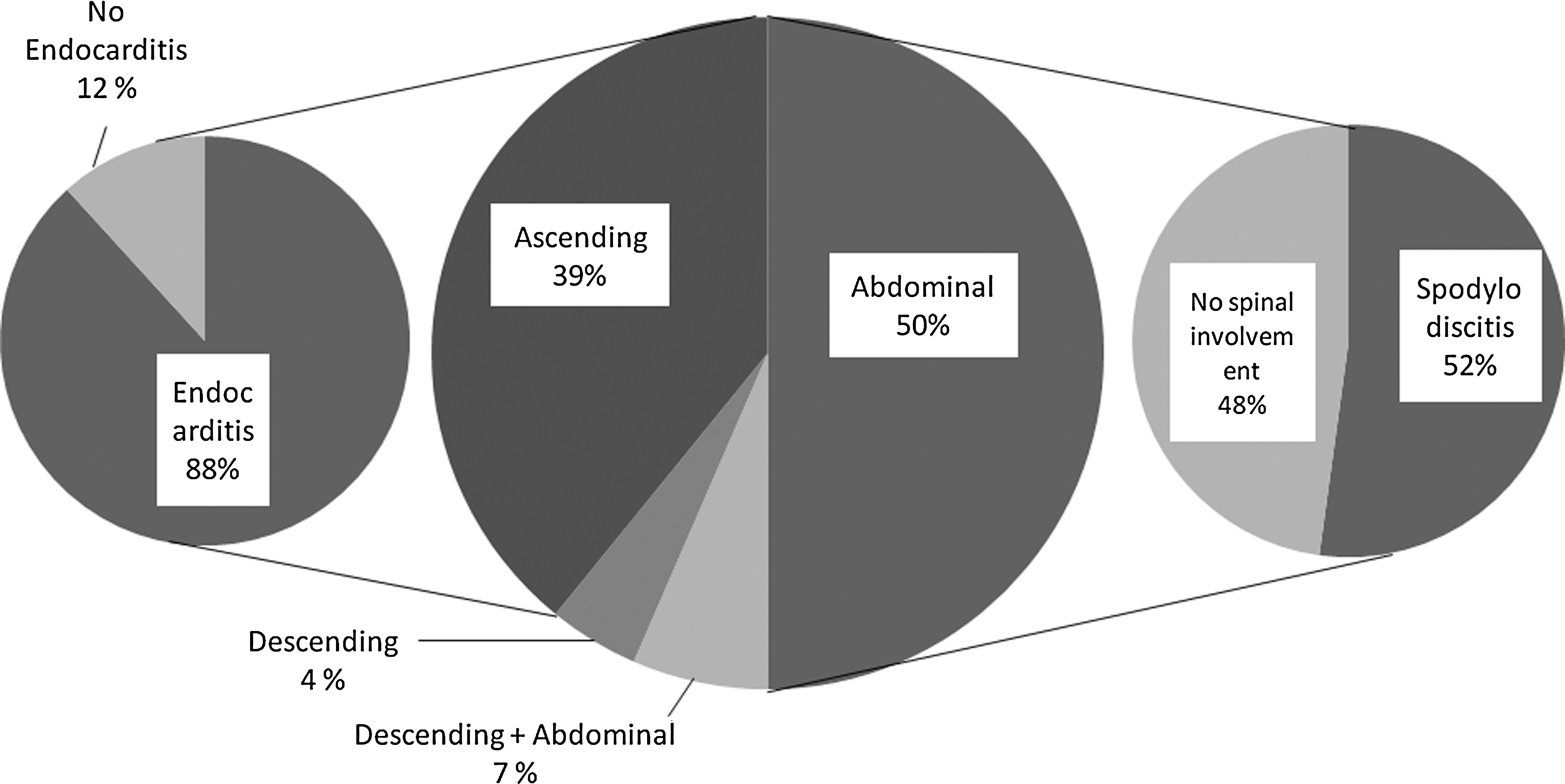
Anatomical localization of the 46 cases of brucellar aortic involvement and relationships with endocarditis and spondylodiscitis.
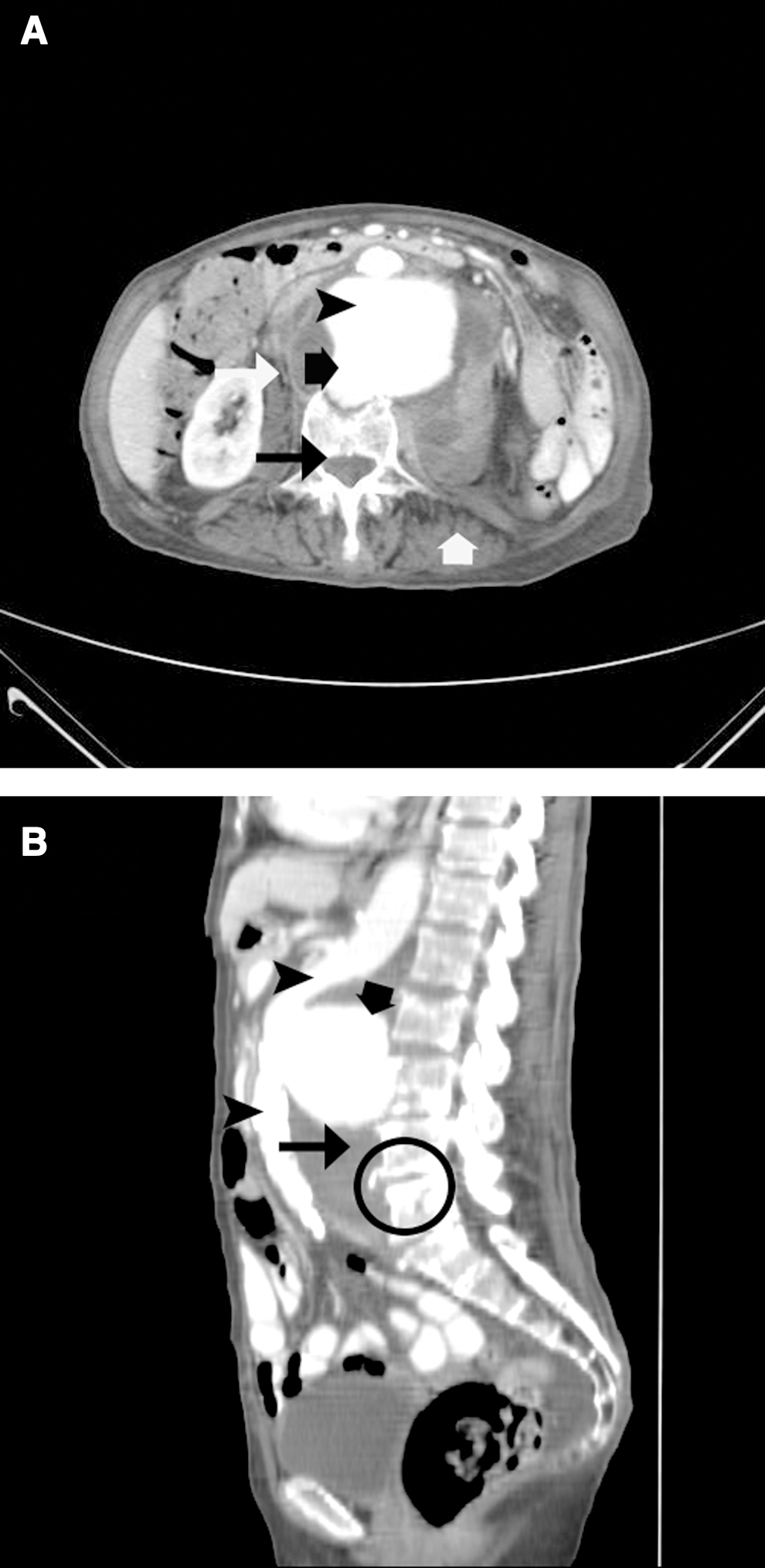
Sagittal and longitudinal angioCT scans of patient UNIME #3. (
Mycotic aneurysms are an infectious degeneration of the arterial wall, caused either by endocarditis with septic emboli to the vasa vasorum, or by direct hematogenous spread during bacteremia. The term “mycotic” was coined by Osler in 1885 to denote fungus-like vegetations; this is misleading, because generally mycotic aneurysms are caused by bacteria. However, circulating microorganisms can colonize: (1) a normal aorta (with or without atherosclerotic plaques); (2) a pre-existing abdominal aortic aneurysm; or (3) a post-traumatic false aneurysm (Papadimitriou et al. 2003). Nevertheless, most authors use the term mycotic aneurysm to describe any aneurysm secondary to infection, regardless of its pathogenesis, including those originating from degeneration of the arterial wall of extravascular origin (Nakata et al. 1968). The term “pseudo-aneurysm” or “false aneurysm” is used to indicate a hematoma communicating with the artery that forms outside the arterial wall secondarily to a contained rupture. Dissecting aneurysms are generally not considered mycotic aneurysms; however, they can be caused by infective aortic involvement. Apart from the 3 cases presented in this review, dissecting aneurysms have also rarely been caused by Salmonella spp. (Kimura et al. 2007), Mycobacterium tuberculosis (Nachega et al. 1998), Treponema pallidum (Kellett et al. 1997), Clostridium septicum (Yang and Reilly 2009), Listeria monocytogenes (Kimura et al. 2008), and Serratia spp. (Matsubayashi et al. 1999).
Immunocompromised patients, including diabetics, alcoholics, and those on steroids or chemotherapy, are at higher risk for mycotic aneurysm formation. Age >50 years has been considered to be a risk factor due to a higher incidence of atheromatous plaques, which serve as microorganism attachment sites due to their irregular surfaces (Betancourt et al. 2007).
Sixteen of 18 cases with ascending thoracic aorta involvement presented with some form of aortic valve endocarditis. The aortic valve is the most commonly involved valve in brucellar endocarditis, which in turn is often associated with spondylodiscitis and peripheral arterial aneurysms (Cakalagaoglu et al. 1999). The concurrent presence of abdominal aortic involvement and spondylodiscitis, observed in 12/26 patients in this series, is striking given the absence of endocarditis in these patients. In most cases in the present review, it was difficult to clarify whether spondylitis preceded aortic involvement or vice versa. In certain cases it was clear that aortic involvement was secondary to corrosive action of a paraspinal or psoas brucellar abscess (Gillet et al. 1983; Bergeron et al. 1992; Sanchez-Gonzalez et al. 1996; Kokkinis et al. 2008; Benedetto et al. 2011), a chain of events also observed in pyogenic and tubercular spondylitis (Doita et al. 2001; Falkensammer et al. 2005; Posacioglu et al. 2009). Alternatively, vertebral erosion could be secondary to mechanical loading induced by the aortic pulsation within the aneurysmal portion (Katz et al. 1962). Another explanation could be that the inflammatory granulomatous reaction surrounding an aortic aneurysm could subsequently infiltrate the vertebral body, leading to secondary erosion as described by Amouzougan and associates (Amouzougan et al. 2007).
The strikingly high percentage of observed complications such as rupture and fistulization can be explained in two ways: (1) either brucellar aortic involvement, even more so than most other causes of infectious aortitis, is a grave complication accompanied by significant mortality; or (2) the cases reported in the literature and summarized here are only the tip of the iceberg, the most severe ones, which were well recognized and deemed worthy of publication. By extrapolating, one can presume that aortic involvement in brucellosis is a much more common complication than these 46 cases indicate, but one that often goes undetected and unreported. For example, a simultaneous diagnosis of brucellosis and an abdominal aneurysm might not necessarily be etiologically correlated by the diagnosing clinician, who may consider the aneurysm's presence an accidental finding. This may be particularly true in the past, prior to the advent of imaging advances that allow recognition of the infective nature of an aneurysmal dilatation.
Clinical presentation and diagnosis
Patients with thoracic aorta involvement presented with chest pain and hypotension. Patients with abdominal aorta involvement exhibited severe abdominal pain and lumbar aches, particularly with accompanying spinal involvement. Cruralgia and testicular pain was reported by patients with psoas abscesses. In two cases the diagnosis of aortic involvement was subsequent to the diagnosis of spondylodiscitis. Two patients with aortobronchial fistulas presented with hemoptysis, while hematemesis was recorded in a patient with an aortoduodenal fistula. Only 11/46 patients acknowledged suffering or having suffered from brucellosis upon hospital admission. Symptoms that could have raised the suspicion of brucellosis (fever and profound perspiration, malaise, and lumbar aches or arthralgias) were present in 21 of the remaining 35 patients.
The diagnosis of aortic involvement was reached by aortography in nine cases, by computed tomography (CT) in 18 cases, by a combination of these in two cases, by a combination of abdominal ultrasonography and aortography in one case, via cardiac ultrasonography in 12 cases, and by post-mortem examination in four cases.
Early diagnosis requires a high index of clinical suspicion and awareness by the radiologist of the spectrum of imaging appearances, especially for the early changes. Imaging is necessary to establish the diagnosis; to localize, characterize, and assess the number of infected aneurysms; to identify associated complications; and to map relevant vascular anatomy (Lee et al. 2008). Sonography is not reliable as an initial imaging modality for the diagnosis of infected abdominal aortic aneurysms (Lee et al. 2008). Multidetector CT angiography is the current imaging modality of choice for the evaluation of suspected infected aneurysms (Lee et al. 2008). Early changes seen with aortic involvement preceding aneurysm formation include an irregular arterial wall, periaortic edema, a periaortic soft-tissue mass, and periaortic gas (Lee et al. 2008).
Serology for brucellosis was positive in 33 cases (in two of them the classic serum agglutination test [SAT] was negative, while Coombs test was positive), negative in 1 case, and of unknown results in 12 patients. Blood cultures were positive in 21 cases, negative in 14, and unknown in 11 patients. Cultures from biopsies (or fine-needle aspiration from abscesses) were positive in 17 cases, not reported in 19 cases, and negative in 10 patients. Polymerase chain reaction (PCR) for Brucella was positive in two patients with negative cultures, while a direct fluorescence assay was diagnostic in another patient. In 24 cases the Brucella species was identified (B. melitensis in 14 cases, B. abortus in 7 cases, and B. suis in 3 cases).
Blood cultures were positive in about 50% of cases, similarly to what was reported by Lehner in a series of aortic involvements due to other microorganisms (Lehner and Wittgen 2005). However, in cases of suspected brucellosis, at least three sets of blood cultures should be performed, and automated continuously monitored blood culture systems should be used (Araj 2010). SAT should always be performed. False-negative results on SAT may be due to the prozona phenomenon, or to the presence of blocking antibodies. The Coombs test, an extension of the SAT, is used for the detection of incomplete, blocking, or non-agglutinating IgG (Araj 2010). Enzyme-linked immunosorbent assay is the test of choice for complicated, focal, and chronic cases, especially when other tests are negative while the case is under high clinical suspicion. It can reveal total and individual specific immunoglobulins (IgG, IgM, and IgA) rapidly (4–6 h), with high sensitivity and specificity (Araj et al. 1986; Araj 2010). If available, PCR for Brucella should be performed on blood and biopsies.
It should be stressed that the diagnosis of brucellar aortic involvement should be suspected based on the epidemiological background, and then be meticulously sought. This is especially important as a lesson for surgeons, who may be the ones primarily tending to the patient, and who may not be familiar with the ability of brucellosis to cause nearly any complication imaginable.
Treatment and outcome
Among the 26 cases with abdominal aorta involvement, 15 were treated by aneurysm resection and dacron or polytetrafluoroethylene (PTFE) graft replacement, five by axillo-femoral bypass, and four by endovascular aneurysm repair (EVAR). In one case surgical treatment was not clearly reported. One patient died soon after laparotomy.
Among the 23 thoracic aneurysm cases, 9 were treated by aneurysm resection and Dacron/PTFE graft replacement or pericardial patch repair, one by aorto-aorto bypass, five by Bentall (or similar) procedure for concomitant valve endocarditis, one by abscess evacuation and repair, and two by EVAR. One was not treated. The remaining four cases were diagnosed post-mortem.
Administered antibrucellar antibiotic regimens included a combination of doxycycline and rifampin in 12 cases, a tetracycline alone (terramycin, doxycycline, or tetracycline) in four cases, rifampin alone in one case, and various combinations of doxycycline, aminoglycosides, rifampin, trimethoprim-sulfamethoxazole, or quinolones in the remainder of cases. The length of antibiotic treatment for the cases with available information and favorable outcomes ranged from 1.5 to 9 months (median 6 months). Twelve out of 42 patients for whom data are available died. Thirty patients were considered cured after a mean follow-up of 21 months (median 18 months; range 0.5–84 months). Mortality was not reported in patients treated with EVAR.
A combination of antibiotic therapy and vascular surgical intervention is the therapeutic cornerstone for infectious aortic involvement (Kan et al. 2007). Medical treatment alone may be inadequate, and is reserved for non-surgical candidates or those refusing surgery; the necessity of lifelong antibiotic coverage in such cases is controversial (Lee et al. 2008). In brucellar infections, prolonged therapy is recommended, especially in the presence of spondylodiscitis, endocarditis, or if infected tissues are not removed. No consensus has been reached about the best treatment regimen for Brucella endocarditis. Ariza and colleagues recommended the combination of doxycycline 200 mg/day and rifampicin 600–900 mg/day for a period of 6 weeks (Ariza et al. 1992). Keles and associates recommended that antibiotic treatment should be continued for at least 6 months after surgery to prevent relapses (Keles et al. 2001; Sasmazel et al. 2010). For the medical treatment of brucellar spondylodiscitis, a regimen with doxycycline 100 mg orally twice daily and rifampicin 600 mg orally daily for 6–52 weeks, plus either streptomycin 1 g IM daily or gentamicin 3–5 mg/kg IV or IM daily for 14–21 days is usually given (Solera 2010).
Surgical treatment also needs to be individualized and may often be technically challenging. The traditional treatment for infected abdominal aortic aneurysms is surgical resection with in situ graft replacement. Prosthetic re-infection or aortic suture dehiscence are risks of this approach. An alternative approach is aortic ligation with resection of all infected tissues and extra-anatomic arterial bypass to the lower limbs. This extra-anatomic reconstruction avoids implantation of prosthetic grafts in an infected environment. Endovascular techniques for the treatment of aneurysms have achieved rapid international acceptance in recent years, as they are less invasive and could reduce mortality compared to conventional open surgery. The use of stent grafts to treat mycotic aneurysms without debridement of surrounding infected tissue, and the implantation of foreign material in infected fields contradicts the rules of septic vascular surgery. Nonetheless, recent literature tends to emphasize endoluminal treatment of mycotic aneurysms, though usually only in the form of case reports with short follow-up periods. A recent meta-analysis of endovascular stent repair for infected aortic aneurysms showed an overall mortality rate of 20.8%, and persistent infections were seen in 22.9% of cases. The 12-month survival rate in the group with persistent infection was 39%, whereas it was 94% in the infection-free group (Kan et al. 2007).
Particularly for brucellosis, one has to recognize the risk of inserting a prosthetic device in such patients, given that prosthetic devices (including joints, defibrillators, valves, or pacemaker leads) have been increasingly implicated in late brucellosis recurrence. Our limited experience with endovascular stents in this context precludes any certainty about their involvement in such scenarios, but experience with other prosthetics should make us cautious. We can thus ask this question about the optimal therapeutic approach: Should an aggressive short course of antibiotics precede any interventional measures when feasible (i.e., when rupture is not imminent), in order to “sterilize” the patient and the infected site as much as possible?
The analysis of the cases reviewed here and their wide distribution over time precludes reaching conclusions about the superiority of any therapeutic approach. However, all four cases treated by EVAR survived. This outcome could be biased, since the use of EVAR is a recent development, and thus improved pre- and post-surgical facilities are available, as are advanced diagnostic approaches that allow earlier diagnosis. The use of EVAR may also indicate a less severe presentation. However, several subsequent reports suggest that overall, EVAR provides a viable, less-invasive alternative for the management of mycotic aortic aneurysms, with favorable results (Dubois et al. 2010).
Conclusions
Brucellar aortic involvement is probably an underdiagnosed and underreported disease, especially in developing countries. Our review of the published work on the subject indicates that the diagnosis of aortic involvement due to Brucella should be established as early as possible to reduce subsequent morbidity and mortality. In particular, patients >50 years old who have blood cultures positive for Brucella, along with fever, back and/or abdominal pain, or chest pain, should undergo an extensive diagnostic work-up for Brucella aortic involvement and aneurysm formation. Similarly, patients with aortic mycotic aneurysms or with pseudo-aneurysms should be evaluated via history (in particular, epidemiologic characteristics), clinical signs and symptoms, and with culture and serology or molecular techniques, as available, for brucellosis. Patients with brucellar aortic involvement should undergo further screening to exclude concomitant endocarditis (in thoracic aortic involvement), or spondylodiscitis/abdominal or pelvic abscesses (in abdominal aortic involvement). A converse procedure should be applied in patients with endocarditis or spondylodiscitis. Anti-brucellar antibiotic therapy should be initiated as soon as possible, followed by whichever surgical approach is considered appropriate. Our limited experience with EVAR in brucellar aortic involvement has shown encouraging outcomes, but one has to take into account the theoretical risks of delayed brucellosis recurrence in the presence of prosthetic devices. The duration of antibiotic therapy, regardless of the accompanying surgical approach, should extend to 3–6 months or more, according to individual needs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.