
Abstract
Scrub typhus is a mite-borne infectious disease caused by Orientia tsutsugamushi (previously called Rickettsia tsutsugamushi). The severity of this disease varies from only mild symptoms to death, and its manifestations are nonspecific. Therefore, clinicians may not correctly diagnose scrub typhus early enough for successful treatment. Reports of infections in travelers returning from Asia to their home countries are increasingly common. Thus, it is important that even clinicians in nonepidemic regions be alert for this disease. Here we describe the epidemiological aspects and clinical manifestations of scrub typhus encountered at a teaching hospital in Penghu, Taiwan, over the past 5 years. A total of 126 patients were confirmed to be positive for scrub typhus at the hospital from 2006 to 2010. All cases were confirmed by the Centers for Disease Control and Prevention or its contract laboratory through pathogen isolation and an indirect immunofluorescence assay. Medical records of these patients were reviewed, and demographic and clinical characteristics, laboratory data, seasonal data, geographic distribution, complications, and outcome were analyzed. The incidence of scrub typhus peaked in individuals aged 0–10 and 51–60 years, with the highest incidence among those ≤10 years of age. No significant difference was noted between sexes. Fever was the most common symptom (93.6%), followed by chills (23.8%), cough (18.3%), and headache (14.3%). Eschars were observed in 78 (61.9%) patients, with the axilla being the most frequent site (n=17; 21.8%). Most patients were retirees (n=63; 50%), followed by students (n=16; 12.7%). Patients were more likely to live in rural areas than urban areas. Scrub typhus was epidemic in the spring (April to June) and fall (October to December) in a bimodal distribution similar to that observed in Japan. Leukocytosis was not common, but most patients had abnormal C-reactive protein levels, thrombocytopenia, and elevated liver function test results. Residents of Penghu, particularly Makung City and Husi Township, as well as travelers to the region during the spring and fall seasons should be educated about the signs and symptoms of scrub typhus. All physicians who come into contact with individuals residing in or traveling to or from epidemic regions should remain alert about the manifestations of this disease.
Introduction
Scrub typhus is endemic to a region of Asia that covers an area west to Pakistan and Afghanistan, east to Japan, and south to Australia (Chang 1995, Hornick 1996). One section of this region is Taiwan, and particularly eastern Taiwan and Penghu Island. The latter region is located at 23.569°N latitude and has a subtropical climate. Although the epidemiology of scrub typhus in Penghu was studied from 1975 to 1979 (Fang et al. 1975, Bourgeois et al. 1977, Olson and Bourgeois 1977, Olson and Bourgeois 1979), few studies have assessed the epidemiology in Penghu over the past 30 years. Therefore, this study was conducted to assess scrub typhus cases encountered at a teaching hospital in Penghu, Taiwan, between 2006 and 2010.
Materials and Methods
This retrospective study was conducted at the Penghu branch of the Triservice General Hospital, which is a 200-bed teaching hospital in Penghu. From 2006 to 2010, 126 patients were treated for scrub typhus. Using pathogen isolation and an indirect immunofluorescence assay (IFA), these cases were confirmed by the Centers for Disease Control and Prevention (CDC) or one of its associated contract laboratories. Confirmation required fulfillment of at least 1 of the following criteria: (1) A positive PCR result for O. tsutsugamushi; (2) a 4-fold increase in the indirect IFA for O. tsutsugamushi as measured in acute and convalescent paired sera; or (3) an immunoglobulin M (IgM) antibody titer against O. tsutsugamushi greater than 1:80. Demographic and clinical characteristics as well as complications, laboratory data, geographic distribution, seasonal differences, clinical symptoms and signs, and outcome were reviewed.
Results
During the period from 2006 to 2010, 126 patients were diagnosed with scrub typhus at the Triservice General Hospital in Penghu. Among the patients with serologically confirmed cases, the IgM antibody titer against O. tsutsugamushi was 1:80 in 17 (13.5%), 1:160 in 83 (65.9%), 1:640 in 2 (1.6%), and negative in 24 (19%) patients (Table 1). Importantly, all 24 patients with negative IgM antibody titers had fulfilled criterion 2 (4-fold rise in indirect IFA for O. tsutsugamushi as measured in acute and convalescent paired sera).
IgM, Immunoglobulin M; IFA, immunofluorescence assay.
Demographic data
Demographic data are summarized in Table 2. Of the 126 patients with a confirmed diagnosis, 48.4% (61/126) were male and 51.6% (65/126) were female. The rates of incidence of scrub typhus in those aged 0–10, 11–20, 21–30, 31–40, 41–50, 51–60, 61–70, 71–80, and 81–90 years were 18.3, 9.5, 10.3, 7.9, 13.5, 15.9, 11.9, 9.5, and 3.2%, respectively, with peaks in the age ranges of 0–10 and 51–60 years. In addition, of the infected patients, there were 7 (5.6%) public officials, 7 (5.6%) military personnel, 2 (1.6%) housekeepers, 2 (1.6%) businessmen, 2 (1.6%) farmers, 2 (1.6%) fishermen, 16 (12.7%) students, 63 (50%) retirees, 14 (11.1%) construction workers, and 11 (8.7%) people in other jobs. Retirees, students, and construction workers were the groups most commonly infected over the 5-year period.
Geographic distribution
As illustrated in Figure 1, Makung City (n=68; 54%) and Husi Township (n=50; 39.7%) had the largest numbers of cases. Although scrub typhus occurred year-round, most patients were diagnosed from April to December in a bimodal distribution. Spring (April to June) and fall (October to December) were epidemic periods, with a high peak in October and a smaller peak in June (Fig. 2).
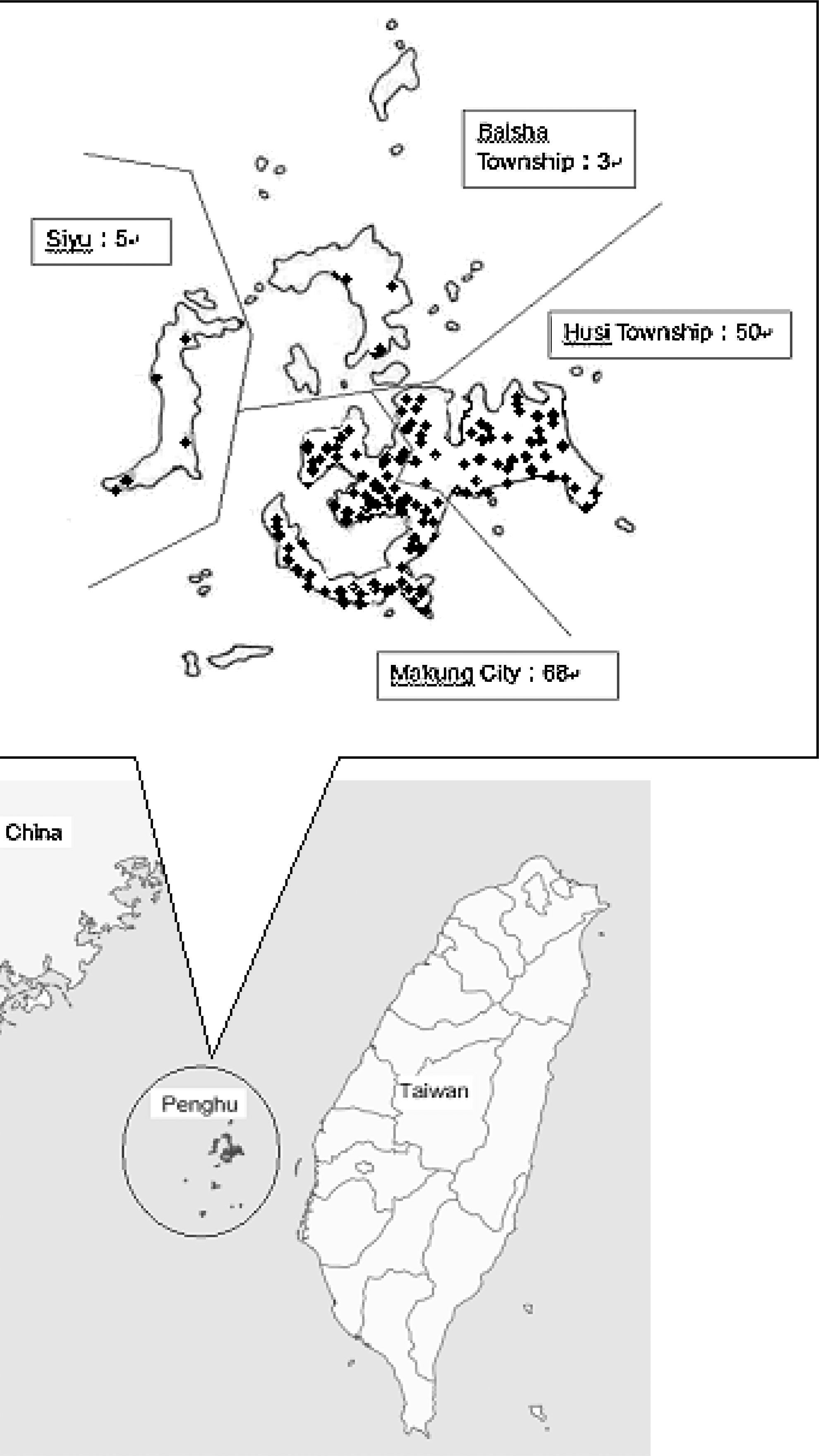
Distribution of cases by geographical region.

Monthly distribution of the total cases.
Clinical symptoms, signs, and complications
Patients were characterized by a broad clinical spectrum ranging from such mild symptoms as malaise and dizziness to such severe complications as acute hepatitis and acute renal failure. Fever was the most common symptom in the patients studied (93.6%), followed by chills (23.8%), cough (18.3%), headache (14.3%), sore throat (11.9%), and malaise (11.9%). Other nonspecific symptoms included nausea, diarrhea, muscle ache, arthralgia, and dizziness (Table 3).
Eschar is the single most useful diagnostic indication of scrub typhus. Seventy-eight (61.9%) patients had eschars, which were distributed all over the body, as described in Table 4. The axilla was the most frequent site of eschars (n=17; 21.8%), followed by the inguinal region (n=10; 12.8%), chest (n=8; 10.3%), abdomen (n=8; 10.3%), and back (n=8; 10.3%).
Laboratory data
Laboratory tests included white blood cell and platelet counts, CRP levels, and liver function tests (Table 5). White blood cell count was in the normal range (<11,000 cells/mm3) in 102 (83%) patients, 11,001–15,000 cells/mm3 in 15 (12.2%) patients, and 15,001–20,000 cells/mm3 in 5 (4.1%) patients. One patient had leukocytosis, with a white blood cell >20,000 cells/mm3. Platelet count was in the normal range (>150×103/μL) in 37 (30.3%) patients, 100–150×103/μL in 44 (36%) patients, and 50–100×103/μL in 39 (31.2%) patients. Only 2 patients had thrombopenia, with platelet counts <50×103/μL (1.6%). In addition, only 4 (3.5%) patients had normal CRP levels (<0.5 mg/dL). Among the other patients, CRP levels ranged from 0.5 to 5 mg/dL in 51 (45.1%) patients, 5 to 10 mg/dL in 37 (32.7%) patients, and above 10 mg/dL in 21 (18.6%) patients.
WBC, White blood cells; CRP, C-reactive protein; PLT, platelets.
Liver function was abnormal in most of the patients tested. Aspartate aminotransferase (AST) levels were elevated in 109 (91.6%) patients, ranging from 40.01 to 80.00 IU/L in 43 (36.1%) patients, 80.01 to 120.00 IU/L in 25 (21%) patients, 120.01 to 360.00 IU/L in 33 (27.7%) patients, and above 360.00 IU/L in 8 (6.7%) patients. Alanine aminotransferase (ALT) levels was elevated in 105 (89.7%) patients, ranging from 40.01 to 80.00 IU/L in 31 (26.5%) patients, 80.01 to 120.00 IU/L in 29 (24.8%) patients, 120.01 to 360.00 IU/L in 35 (29.9%) patients, and above 360.00 IU/L in 10 (8.6%) patients. Among those for whom bilirubin data were available, only 3 (22.3%) patients had an abnormal direct bilirubin level (>0.41 mg/dL); 10 (18.8%) patients had an abnormal total bilirubin level (>1.21 mg/dL).
Outcome
All patients analyzed had recovered without significant sequelae and performed well at the follow-up visit 4 weeks after discharge.
Discussion
Among the 126 patients with a confirmed diagnosis in this study, the distribution between sexes was not significant. The data from this study differ from those reported in Taiwan and other countries, where cases of scrub typhus have occurred predominantly in males. One explanation for the difference is that the men of Penghu are largely fisherman, whereas women tend to work on farms accompanied by their children (Olson and Bourgeois 1979). Therefore, women and children are at a relatively higher risk of exposure than men. On the other hand, the risk of infection was almost equal between students and retired persons due to the natural environment in Penghu. In Penghu, coral was often used to build the walls of houses, and fencerows of miscanthus and coral walls are commonly used as windbreakers around cultivated fields. Miscanthus and coral walls have been shown to be the most productive habitats for scrub typhus, because the percentage of infected mites was highest in collections from these habitats (Cooper 1964, Wang 2007). Therefore, the exposure to the walls that surround dwellings and fields accounts for the equal incidence of students and retired persons of different sexes. Moreover, young people tend to move to cities for work, and the elderly are left to work as farmers on their own land. Retired persons enjoy outdoor activities. Therefore, both natural environment and daily activity account for the lack of a significant difference between sexes of the student and retired person demographic groups (Lee et al. 2006).
In addition, a major change has occurred in Penghu since Olson's study was conducted 30 years ago (Olson and Bourgeois 1979), which reported that children were less likely to be infected. The data reported here reveal a higher infection rate in children over the last 5 years, with the highest incidence among those aged 0–10 years. Moreover, most of these children (18/23) were preschool children. Among the 18 preschool children (18/126; 14.3%), 11 lived in Husi Township, which was a much higher incidence than in Makung City. Moreover, 15 students were infected, which accounted for 11.9% of all cases.
We hypothesize that there are 3 main reasons that could explain why our study found that more children were infected compared to the study from 30 years ago: (1) The increasingly older age distribution due to advancements in public health have increased the number of persons within the retired persons demographic, who may be more likely to take children outside for activities. (2) More young people go to cities for work today and leave older people to handle affairs on their own farms (Lee et al. 2006). This may have increased the number of children brought to the farms. (3) Due to economic and transportation developments, it is convenient and affordable for parents to travel with their children around Penghu. These reasons may have increased the exposure risk of children compared to the risk that was present 30 years ago.
The largest number of cases occurred in Makung City (n=68; 54%) and Husi Township (n=47; 37.3%). According to the website of the Penghu government (
Several decades ago, the incidence of scrub typhus in Penghu peaked during June and early July (Bourgeois et al. 1977), which is a pattern similar to that in Taiwan and southern China (Huang et al. 2009). In this study, epidemics in Penghu over the last 5 years occurred in the spring (April to June) and fall (October to December), with a high peak in October and a smaller peak in June. Such a bimodal pattern—spring and fall—is similar to the pattern observed in Japan (Liu et al. 2009). Epidemics are influenced by climatic factors, such as temperature and humidity, which are related to the activities of the infected mite. Moreover, this may be due to changes in mites or rodents species over the past several decades. We review several papers (Olson 1979, Ogawa 2002, Lee et al. 2006, Wang 2007, Huang et al. 2009, Liu et al. 2009) about climate change in Penghu as well as changes in the species of mites and rodents in Taiwan, Japan, and China in an attempt to determine to the reason for the change in seasonal distribution of scrub typhus in Penghu over the past 30 years. We found that Leptotrombidium deliense remained the major mite of the regions, but the main hosts have shifted from Suncus murinus and Rattus spp. 30 years ago to Rattus losea today. The peak breeding season for S. murinus is during the summer and autumn, and for R. losea is in July and August (Luo 1988, Wang et al. 2007). The gestation period of R. losea is usually 23 days, so there is an abundance of rodents present in September or October (Traub and Wisseman 1974, Kawamura et al. 1995, Kuo 2010). However, the change in the main host in Penghu does not seem to explain the temporal shift of the scrub typhus peak. Therefore, we further evaluated the responses of chiggers to environmental change.
One study (Wang 2007) found that, in addition to temperature, rainfall may be the main cause of the effect on mite activity in tropical regions such as Penghu. Approximately 1–2 months after the period of increased rainfall, an increased infection rate of scrub typhus was observed. In Penghu, 2 rainy seasons occur each year in May and June, which is called the plum rain season, and in July to September, which is the typhoon season. In the past several decades, the rainfall in May and June decreased and the rainfall from July to September increased according to reports by the Central Weather Bureau (
The clinical spectrum of scrub typhus is broad, ranging from subclinical disease to severe complications, such as pneumonia, acute respiratory distress syndrome, pulmonary edema, congestive heart failure, central nervous system dysfunction, acute renal failure, and septic shock. According to previous studies (Lee et al. 2006, Huang et al. 2009, Jim et al. 2009), fever is the most common symptom (90.1–100%) of scrub typhus, followed by cough (50%), poor appetite (43 %), headache (40–61.9%), and skin rash (21.6–36%). The symptoms of the patients described here were similar to those previously reported. The clinical manifestations are not pathognomonic and may initially mimic many other conditions, including meningitis, hepatitis, acute pulmonary distress syndrome, and interstitial nephritis. The varied clinical presentation can be explained by the pathogenesis of the disease: O. tsutsugamushi frequently enters the human body through areas of the skin and mucous membranes damaged by mite bites and spreads through the bloodstream and tissues, initially without inflammation. Vasculitis, perivasculitis, endothelial damage, and inflammatory infiltrates composed of monocytic cells, histiocytes, and neutrophils develop in any tissue affected (Settle et al. 1945, Levine 1946, Saah 2000). According to Yoon's analysis, interleukin-17 might be a cause of vasculitis-associated headache (Yoon et al. 2010). The clinical presentation reflects secondary changes in the affected organs and the severity of the damage, although the great majority of infections caused by scrub typhus are self-limited.
An eschar begins as a small papule that enlarges, undergoes central necrosis, and eventually acquires a blackened crust with an erythematous halo that resembles a cigarette burn. It is the single most useful diagnostic sign of scrub typhus. It usually occurs at sites where skin surfaces meet or clothes bind, such as the axilla, groin, neck, waist, and inguinal areas. Therefore, the aforementioned sites, and especially the axillary and groin regions, should be carefully examined in patients with fever but without a significant source of infection in regions in which scrub typhus is endemic, even if a contact history is not confirmed.
Leukocytosis was not common in the patients of this study, but most had abnormal CRP levels and elevated liver function tests. These findings were also reported in a previous study (Lee et al. 2002). Therefore, elevated CRP levels without leukocytosis may suggest scrub typhus. We also found that in contrast to the findings from previous studies, most of the patients in this study had thrombocytopenia. Thrombocytopenia and elevated liver function tests are manifestations of ongoing hepatitis. However, although most of the patients showed hepatic dysfunction, the underlying mechanism remains unknown.
Conclusion
Penghu has a high prevalence of scrub typhus due to the subtropical climate. This study found that children, retirees, and students are demographic groups at a high risk for contracting scrub typhus. Prevention of scrub typhus requires educating residents of Penghu as well as travelers to the region to avoid contact with soil and vegetation and to wear protective clothing and footwear, especially in Makung City and Husi Township, during the spring and fall seasons. Parents have to be reminded that children up to age 10 are at the highest risk. Physicians must be informed that early diagnosis is critical, and they must remain alert to the possibility of scrub typhus infection not only in people living in regions in which scrub typhus is endemic, but also in those traveling to or from these regions.
Author Disclosure Statement
No competing financial interests exist.