
Abstract
During 2008–2011, we tested 874 blood samples from febrile patients who had a fever >37.5°C, and 207 surface samples in households for Coxiella burnetii DNA in two rural Senegalese villages (Dielmo and Ndiop). Fisher's exact test and Spearman's correlation coefficient were used for statistical analysis. We identified four blood samples as positive for Coxiella burnetii DNA. The prevalence of Q fever in all tested samples was 0.46% in the two villages. C. burnetii DNA was also found in 7.5% of the dust samples in Ndiop, and in 0.9% in Dielmo; the prevalence in households was 22.6% in Ndiop and 2.6% in Dielmo. In Ndiop we found a weak correlation between positive environmental samples and the occurrence of the disease. Our findings show an association of environmental C. burnetii with human Q fever cases in a recently identified endemic area in rural Senegal.
The seroprevalence of Q fever has been reported throughout the African continent, but is generally higher in West Africa (Tissot-Dupont et al. 1995; Boni et al. 1998). Recently, we have reported a high seroprevalence of Q fever in the Sine-Saloum region of Senegal (59/238, 24.8% in Dielmo, and 9/241, 3.7% in Ndiop) (Mediannikov et al. 2010). The objective of this study was to continue the survey of Q fever in this region, where we investigated the possible association of the acute Q fever cases with environmental exposure.
We conducted sampling during November 2008–July 2009 and June 2010–October 2011 in two rural Senegalese villages in the Sine-Saloum region: Dielmo (13°43’N, 16°24’W), and Ndiop (13°41’N, 16°23’W) in both villages for both time periods (Trape et al. 1994). During the study periods, we screened 874 blood DNA samples for Q fever. A total of 643 samples were collected from 273 patients (including 143 patients with >1 sample) from Dielmo (434 inhabitants), and 231 from 141 patients (including 52 patients with >1 sample) from Ndiop (457 inhabitants). Medical examinations and blood sampling were conducted for each person who had a fever >37.5°C. There was no overlap in samples between this and previous studies (Mediannikov et al. 2010). At the beginning of the study, all participants, including parents or legal guardians of all children, gave written individual informed consent. The national ethics committee of Senegal and the local ethics committee of Mediterranean University, Marseille, France, approved this project. No one died during the study, and all patients with identified Q fever recovered completely.
To predict the occurrence of C. burnetii in the household environment, swab samples from the dust-accumulating surfaces of the main entrance, bed, and storehouse of each household in Dielmo and Ndiop were collected in September, 2011. We tested 207 surface samples for C. burnetii DNA in 69 households (114 samples in 38 households in Dielmo, and 93 in 31 households in Ndiop). The areas were swabbed with a moisturized (phosphate-buffered saline) sterile thin cotton swab (100×0.9 mm). DNA was extracted as previously reported (Mediannikov et al. 2010).
Bacterial DNA from blood and dust was initially detected by C. burnetii-specific semi-quantitative PCR with primers and probes designed for the amplification of IS1111 and IS30A spacers. Appropriate handling and DNA extraction from blood were controlled with qPCR of the β-actin gene (Rolain and Raoult 2005; Mediannikov et al. 2010). We analyzed the incidence and prevalence data using Epi Info software, version 7.0.8.0 (Centers for Disease Control and Prevention).
We identified four blood samples as positive by two genus-specific qPCR systems. The prevalence of Q fever in all tested samples was 0.46% (4/874). All positive samples were found at the end of the dry season and the beginning of the rainy season (one at the end of May 2011, two in June 2009 and 2011, and one at the beginning of July 2010). One patient lived in Dielmo (2009), and three lived in Ndiop (2010–2011). Essentially no difference in the incidence rate for the survey period was found between Dielmo (7.3/10,000 person-years) and Ndiop (22.3/10,000 person-years).
C. burnetii DNA was also found in 7.5% of the dust samples from all locations in Ndiop, and in 0.9% of the samples from Dielmo (7/93 versus 1/114; p=0.024 by two-tailed Fisher's exact test). The prevalence in households was 22.6% in Ndiop and 2.6% in Dielmo (7/31 versus 1/38; p=0.019 by two-tailed Fisher's exact test). In both villages, the contamination was distributed among the different locations sampled (four in beds, two in entrances, and two in storehouses). In Ndiop, we found C. burnetii in dust samples in two-thirds of households where patients with acute Q fever were recorded, and the weak correlation between positive environmental samples and the occurrence of the disease was significant (Spearman ρ=0.35, p=0.05).
We concluded that in 2008 we identified an epidemic focus in Dielmo with 59 (24.8%) serologically converted individuals. In contrast, in Ndiop we reported only nine cases that were seropositive for C. burnetii (Mediannikov et al. 2010). We overlaid the previously published data on C. burnetii antibodies detected in 2008 in Dielmo and Ndiop on top of the data on the prevalence of C. burnetii DNA in the blood of acute febrile patients and households surveyed in 2010 and 2011, to trace the development of the epidemiological situation in both villages (Fig. 1).
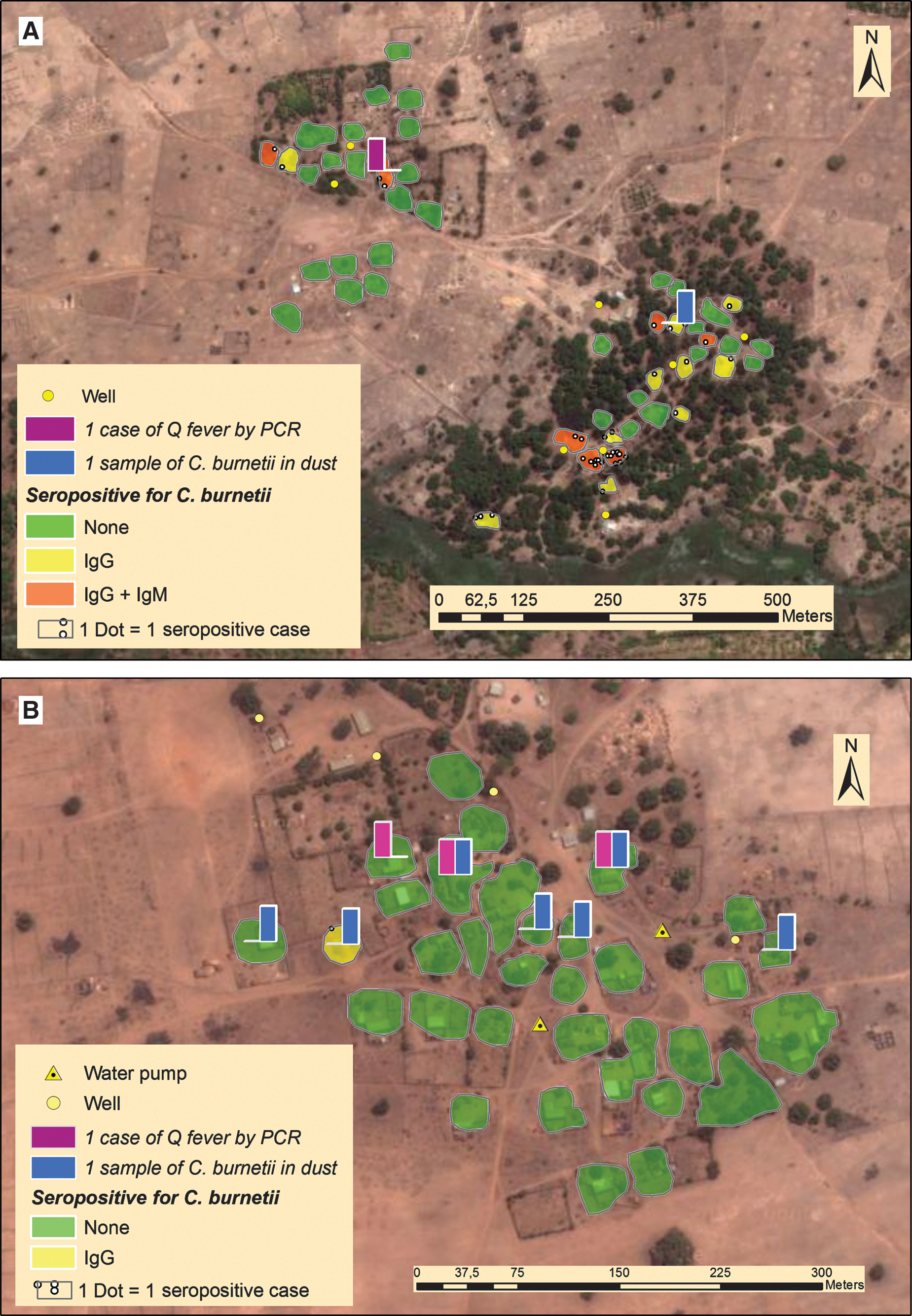
(
In 2010–2011 in Dielmo one PCR-positive patient was registered and only one environmental sample contained C. burnetii DNA that demonstrated the persistence of disease. In Ndiop during the subsequent years, three cases of C. burnetii DNA were found in blood (Fig. 1). The overall incidence of C. burnetii in dust samples in 2011 was also much higher in Ndiop than in Dielmo. It therefore appears that our survey revealed the probable beginning of the development of an epidemic focus in Ndiop.
A limitation of this study is that the prevalence of Q fever in domestic animals in these villages is still unknown. It is known that many herds of livestock are infected with C. burnetii, but livestock should be studied in future research efforts.
The classical epidemiology of Q fever suggests that it is transmitted from animals to humans by inhalation of aerosols (Maurin and Raoult 1999). Our study confirmed that the dust settled inside the households contains the agent of Q fever, and thus may be the direct source of the infection.
Our study demonstrated the presence of C. burnetii DNA in household environments in rural Senegal. The sample size and the collection at one point in time do not permit quantitative elaboration. We confirmed that rural Senegal is an endemic area for Q fever, with continuing cases and the presence of the pathogenic agent in household dust.
Footnotes
Acknowledgments
We are grateful to the inhabitants of Dielmo and Ndiop, Senegal, who participated in this study, and to Geetha Subramanian and Alpha Kabinet Keita for technical support.
Author Disclosure Statement
No competing financial interests exist.