
Abstract
Human brucellosis in Ecuador is underreported and based only on passive surveillance. Since 2008, brucellosis was removed from the list of communicable diseases in the country. Until now, the true human brucellosis picture has not yet been determined. The aim of this study was to determine the seroprevalence of the disease, identify risk factors associated with brucellosis seropositivity in humans, and isolate circulating strains of Brucella spp. in the northwestern part of Ecuador. Between 2006 and 2008, a large transect survey was conducted, based on blood sampling of people from the northwestern part of Ecuador (n=3733) together with an epidemiological inquiry. On the basis of three diagnostic tests used in parallel, the overall seroprevalence was estimated as 1.88% (95% confidence interval [CI] 1.48–2.38). Based on a multivariable random effects logistic regression analysis, the main risk factors associated with human brucellosis seropositivity were contact with livestock (odds ratio [OR]=3.0; CI 1.25–7.08), consumption of fetus and placenta (OR=2.5; CI 1.18–5.22), and involvement in activities at risk for brucellosis infection (OR=1.8; CI 1.00–3.35). Noticeable variation in brucellosis seropositivity among humans within cantons was observed. The circulating strain was Brucella abortus biotype 4. This study emphasized that contact with livestock, consumption of fetus and placenta, and occupational hazard group were all significant risk factors for the transmission of brucellosis among individuals in the northwestern part of Ecuador. Alongside encouraging the launching of educational campaigns against brucellosis, especially in rural areas where 36% of the population lives, controlling this zoonotic disease in animals will directly benefit its prevention in humans, especially because there is no safe and efficacious vaccine against brucellosis in humans.
Introduction
B
In Latin America, four in ten people live in areas where brucellosis is endemic in natural animal reservoirs (Alvarez 2001). However, the infection in humans is underestimated and often not reported (Dean et al. 2012), and only few reports exist concerning the identification of circulating strains of Brucella spp. (e.g., Deodato et al. 2011, Aznar et al. 2012, Ron-Román et al. 2012). In addition, the true incidence of this zoonosis has not yet been estimated (Lucero et al. 2008, Aznar et al. 2012).
In Ecuador, by means of diagnostic assays with low sensitivity, several authors have reported the presence of antibodies against Brucella spp., mainly among slaughterhouse workers. Intriago (1971) reported a prevalence of 4% (1/25), León (1979, cited by Delgado 1992) detected 10.90% (23/211), Zurita (1980, cited by Díaz 2001) detected 23.83% (56/235), and finally Delgado (1992) mentioned a seroprevalence of 2.32% (4/173).
Despite brucellosis being a communicable disease in Ecuador since 2007, the true incidence of human cases remains largely unknown. According to the Ministry of Health (MSP), only 111 human cases were reported between 1990 and 2007 (EPI-2 2008), whereas, the National Institute for Statistics and Census (INEC) registered 152 persons hospitalized for brucellosis between 1995 and 2007 (INEC 2008).
The aim of the present work was to obtain a realistic figure of the prevalence of human brucellosis by determining the seroprevalence of antibodies against Brucella spp., and by identifying the causal agent together with possible infection-associated risk factors among people living and/or working in the northwestern part of Ecuador.
Materials and Methods
Description of the study and selection of the study region
Between 2006 and 2008, a transect study was conducted, based on blood sampling of people from the northwestern part of Ecuador together with an epidemiological survey. After informed consents were obtained, blood samples were taken from persons inhabiting the high-altitude or Sierra provinces such as Carchi, eastern Imbabura, eastern Pichincha, and the coastal provinces such as Esmeraldas, Manabí, western Imbabura, and western Pichincha.
Selection of provinces was based on the high provincial-level seroprevalence of bovine brucellosis reported in Ecuador. Seroprevalence was officially estimated to be between 4.0% and 10.62% in the Sierra and between 5.88% and 10.62% in the Coast (MAG-SESA 1999, Torres 2008). Prior to this study, the seroprevalence was also estimated to be between 2.17% and 9.42% using the Rose Bengal (RB) test and indirect enzyme-linked immunosorbent assay (iELISA), respectively, in bovines of Santo Domingo (Pichincha) and between 1.08 and 9.73% to RB and iELISA, respectively, in El Carmen (Manabí) (Angulo and Tufiño 2005). The selection of the study zone was also based on the occurrence of 41.30% (19/46) of the human cases, as reported by MSP between 1997 and 2007 (EPI-2 2008) and 51.97% (79/152) of the hospitalized brucellosis patients, as reported by INEC (2008). In addition, because sheep, goats, and camel populations are very small in the study area, only the link between brucellosis seroprevalence in bovines and humans was investigated. A map of the study area is shown on Figure 1.
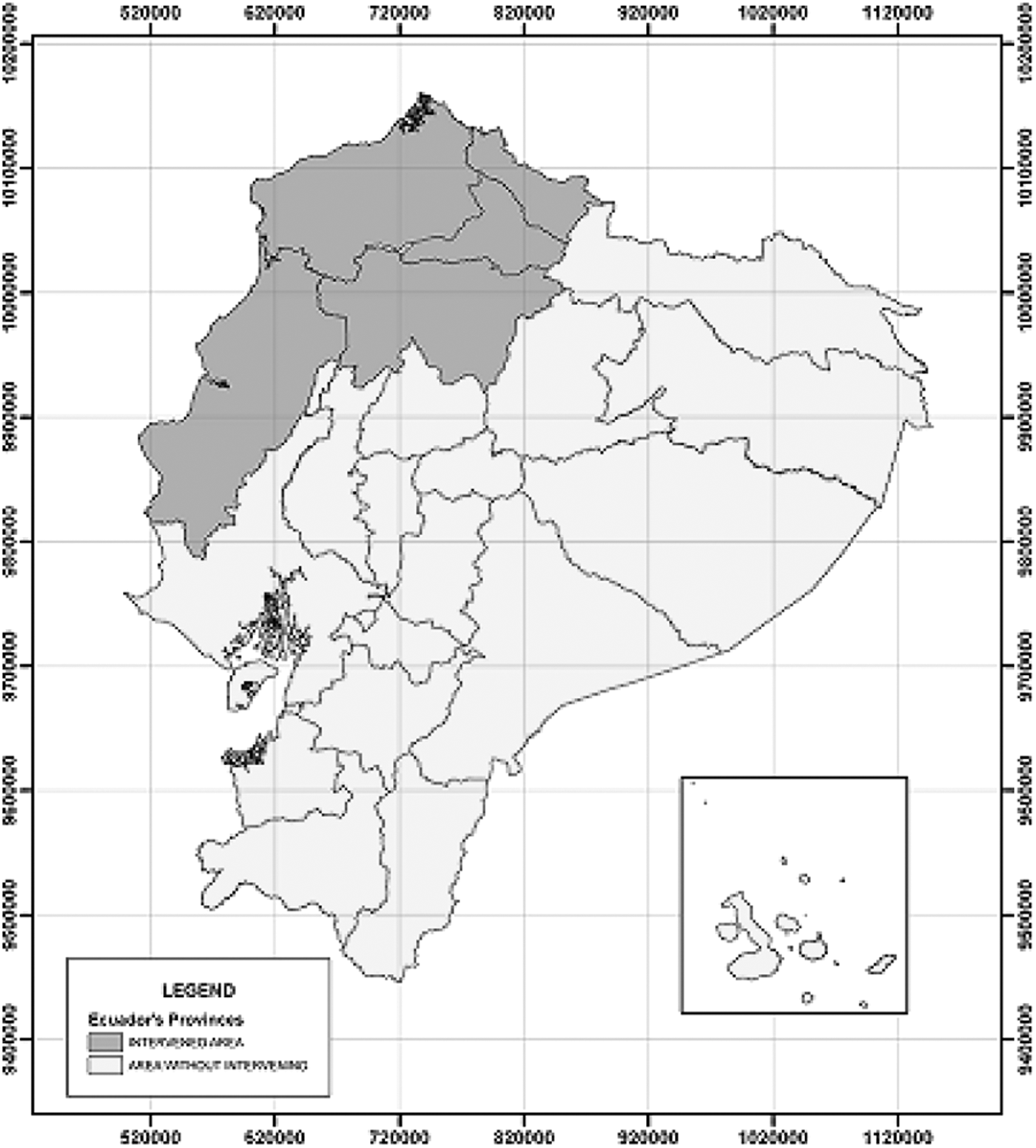
Location of the study area.
Samples
After informed consent, a total of 3733 blood samples were taken from people with different occupational hazards. A first possible high-risk group of people (n=2444) consisted of laborers at cattle farms, slaughterhouse workers, meat and organ traders, cattle traders, veterinarians, zoo workers, teachers and students from a faculty of animal production, and farm and slaughterhouse managers. A second possible low-risk group of people (n=1289) consisted of agricultural laborers, informal traders, public servants, school and college teachers and students, house workers, and transporters.
In addition to collecting blood samples, other information was collected through personal face-to-face interviews. The questionnaire recorded the following information for each subject: Age, sex, consumption of raw milk (yes or no), consumption of blood (yes or no), consumption of cheese (yes or no), region (Sierra or tropical), consumption of fetus or placenta (yes or no), occupational hazard group, contact with animals (yes or no), and presence of symptoms such as pyrexia, weakness, sweating, muscle pain, backache, and headache suggestive of brucellosis (Mantur et al. 2006). On the basis of results of the questionnaire, people were divided into two groups, i.e., those working directly or indirectly in a slaughterhouse (n=542) and those who were not (n=3191). The full questionnaire is available upon request from the corresponding author.
Diagnostic assays
Three serological assays to detect antibodies against Brucella spp. were used: RB fast agglutination test (RB), Wright's slow agglutination test with EDTA (SAT-EDTA), and iELISA. Samples were processed and analyzed in the laboratory for immunodiagnosis at the International Centre for Zoonoses (CIZ) of the Central University of Ecuador (UCE).
RB fast agglutination test
The RB assay was used with Bengatest® antigen, i.e., a concentrated suspension (4% vol/vol) of Brucella abortus Weybridge strain 19, heat- and phenol- (0.5%) inactivated, suspended in an acid buffer and stained with RB. Equal quantities (30 μL) of serum and antigen were mixed in a well (4 min) on a glass plate, and any degree of agglutination was considered a positive reaction.
Wright's slow agglutination test with EDTA
For SAT-EDTA, the antigen (Antigen SAW®, Synbiotics code #ASAW) was a concentrated suspension of B. abortus (strain 1119/3), heat and phenol (0.5%) inactivated, and suspended in a phenol buffer at 0.5%. The assay was performed as described by Godfroid and Boelaert (1995) with serum dilutions of 1/12.5, 1/25, 1/50, 1/100, 1/200, 1/400, 1/800, 1/1600, 1/3200, 1/6400, 1/12,800, and 1/25,600 in a constant volume (100 μL) of antigen. Quantitative results were given as International Units of Agglutination (IU/mL). A value equal to or above 100 IU/mL, corresponding to 75% transparency of dilution 1/50, was considered as a positive reaction.
Indirect Enzyme Linked Immunosorbent Assay
The assay was performed according to Godfroid and Boelaert (1995). Smooth B. abortus Weybridge strain 19 lipopolysaccharide (LPS) antigen was incubated on polystyrene plates for 3.5 h at 37°C and overnight at 4°C. Plates were washed five times with a washing solution (NaCl 0.9%+Tween 20 at 0.01%). A 50-μL amount of 1/50 diluted serum in glycine–EDTA–Tween 80 buffer (BB) was added per well and the calibration curve was determined at dilutions 1/270, 1/540, 1/1080, 1/2160, 1/4320, and 1/8640. After 1 h of incubation at ambient temperature, the solutions were discarded, plates were washed five times and 50 μL of conjugate (Protein G-HRPO, Pierce CD47675, diluted at 1/1500 in G-HRPO+fetal calf serum [FCS] at 2%) was added to each well and left to incubate at ambient temperature for 1 h.
The same washing procedure was repeated, and 100 μL of substrate solution (i.e., ortho-phenylenediamine tablets [o-PD], Sigma P-8287; one tablet of 10 mg dissolved in 25 mL of citrate phosphate buffer Sigma P-4809+5 μL hydrogen peroxidase [H2O2] at 30%) was added to each well. Plates were left to incubate for 20 min in the dark at ambient temperature. Subsequently the reaction was stopped by adding 25 μL of H2SO4 (2 M) to each well. Optical densities (OD) were read by a spectrophotometer (STAT FX 2100), with filters between 492 nm and 630 nm. Mean OD values of the samples and the calibration curve were corrected by subtracting the mean BB (background blanco) from the mean OD.
A cut off value above which a sample was considered positive was set at or above 20 units (U)/mL. This cutoff value was established based on local epidemiological conditions and to optimize the compromise between sensitivity and specificity (Franco et al. 2007, Gómez et al. 2008, Soudbakhsh et al. 2009). Calculation of the units was based on the reference values of the curve, i.e., 1.87 U, 3.75 U, 7.5 U, 15 U, 30 U, and 60 U, for dilutions 1/270, 1/540, 1/1080, 1/2160, 1/4320, and 1/8640, respectively.
Isolation and typing of Brucella spp. (according to Alton et al. 1988)
Due to the lack of standardized procedures in Ecuador, the isolation of the causal agent was based on blood cultures: BACTEC (three repetitions with 30-min intervals) from persons with high serotiters (n=22) (Yagupsky 1994, Cetin et al. 2007). Blood cultures were done at the Hospital Vozandes Quito, where they were maintained for 30 days, and after that timespan the cultures were considered as negatives.
Isolated Brucella were identified and typified by CIZ and also by Veterinary and Agrochemical Research Centre (VAR-CERVA) as a reference laboratory using: (1) Macroscopic and microscopic observation of the colonies in cultures, (2) biochemical assays (oxidase, catalase, and urease), (3) production of hydrogen sulfide (H2S), (4) CO2 growth requirement, (5) growth in stained media (thionine, basic fuchsin, safranin), (6) agglutination with monospecific sera A and M, and (7) PCR-AMOS as described by Bricker and Halling (1994).
Statistical analysis
To determine the potential risk factors associated with human brucellosis seropositivity, a two-stage modeling approach was used. In this approach, individuals were considered positive if they tested positive in at least one serological test along with the presence of any of the clinical symptoms suggestive of brucellosis as previously mentioned.
First, a univariate analysis was performed using a random effects logistic regression model. The model was used as response, and the brucellosis status of the individuals (1 for positive and 0 for negative) and each risk factor or indicator variable in turn as the independent variable. The possible effects of variations in brucellosis seropositivity among the different provinces and cantons were accounted for by incorporating province and canton as a random effects in the model (VanLeeuwen et al. 2010).
Second, variables with a p value ≤0.25 in the univariate analysis were further analyzed in a multivariable random effects logistic regression model. A manual forward stepwise model building approach was employed with the Akaike information criterion (AIC) as the calibrating parameter to select the final model. The model with the smallest AIC is considered to be the most appropriate model. All two-way interaction terms of the variables remaining in the final model were assessed for significance. The effects of confounding were investigated by observing the change in the estimated coefficients of the variables that remain in the final model once a nonsignificance variable is included. When the inclusion of a nonsignificant variable led to a change of more than 25% of any parameter estimate, that variable was considered to be a confounder and was included in the model (Dohoo et al. 2003). The intraclass correlation coefficient (ICC), which is a measure of the degree of clustering of individuals belonging to the same province and canton, was computed (Snijders and Bosker 1999).
The models were built using the xtmelogit () function in STATA, v. 12, software (SataCorp LP, College Station, TX). Model selection was done using Laplacian approximation whereas parameter estimates from the final model were obtained using adaptive Gaussian quadrature (Twisck 2003). The robustness of the final model was assessed by increasing the number of quadrature (integration) points and monitoring changes in parameter estimates (Frankena et al. 2009).
Ethical considerations
The protocol was thoroughly reviewed and approved for ethics by the Bioethics Committee of the Biomedical Center, Central University of Ecuador. Prior to being included in the study, all participants provided informed written consent. For minors, parents/guardians provided consent on their behalf.
Results
Descriptive statistics
A total of 3733 persons, with a mean age of 30.03±16.26 years (min=3, max=89 years) were sampled in five provinces in the northwestern part of Ecuador—Carchi, Imbabura, Esmeraldas, Manabí, and Pichincha. Seventy people with mean age 37.86±14.81 years (min=10, max=79 years) reacted positively to at least one of the three diagnostic tests, representing an overall seroprevalence of 1.88% (confidence interval [CI] 1.48–2.38). The proportion of seropositive people between groups (slaughterhouse workers vs. other people) was 4.8% (26/542) and 1.4% (44/3,191), respectively. This suggests a preferential repartition of seropositive people in slaughterhouse workers (Pearson chi-squared test=29.4; p<0.001).
The distribution of the number of individuals tested, the number and percentage of seropositives are presented in Table 1. Teenagers and children represented 20.84% (778/3733) of the sample, with only six of them being seropositive (three originating from farms). The information about this subpopulation is presented in the Table 2. This suggests a preferential repartition of seropositive cases among older people (Pearson chi-squared test=6.50; p=0.01).
RB, Rose Bengal; SAT-EDTA, Wright's slow agglutination test with EDTA; iELISA, indirect enzyme-linked immunosorbent assay; SLA, people working in a slaughterhouse; OTH, other people.
RB, Rose Bengal test; SAT-EDTA, Wright's slow agglutination test with EDTA; iELISA, indirect enzyme-linked immunosorbent assay.
Risk factors for human brucellosis seropositivity based on the univariate random effects logistic regression analysis
On the basis of the results of the univariate random effects logistic regression analysis with random intercepts for both province and canton, the factors age, sex, contact with livestock, contact with fetal secretions, consumption of fetus and placenta, and involvement in activities at risk were all statistically significantly associated with human brucellosis seropositivity (p<0.05) (Table 3). On the other hand, consumption of raw cow milk and consumption of fresh blood were not significant at the 5% level but because their p values were ≤0.25, they were considered as potential risk factors and were thus included in the multivariate random effects logistic regression analysis.
The p values are based on the likelihood ratio test comparing the random intercepts-only model and the random effects model with each covariate in turn.
See definition in Materials and Methods section.
This variable was used as a random effect in the logistic regression analysis.
CI, confidence interval; Ref, reference category.
Final model based on multivariate random effects logistic regression analysis
Out of the potential risk factors initially considered in the multivariate random effects logistic regression model, three were included in the final model (i.e., consumption of fetus and placenta, contact with livestock, and occupational hazard group). In addition, the results were not confounded by any of the variables not included in the final model. Increasing the number of quadrature points had no influence on the estimated fixed effects and the variance component parameters, indicating that the model is robust. The estimated odds ratios and their 95% CI are presented in Table 4. There was no variability in brucellosis seropositivity among provinces but rather a higher variability among people within provinces.
95% Confidence interval was not estimated by the model.
OR, odds ratio; CI, confidence interval; Ref, reference category; SE, standard error.
Typifying of circulating Brucella spp. in northwestern Ecuador
Detailed information about persons with positive blood cultures (n=22) is given in Table 5 with the characteristics of the isolates, bacteriological data and PCR in Table 6 and Figure 2, respectively. From three positive cases, B. abortus biotype 4 was isolated and typified. Blood cultures were only positive for patients with higher levels of immunoglobulin M (IgM) antibodies (SAT-EDTA) suggesting an acute brucellosis.

PCR-AMOS of Brucella from blood cultures, isolated from positive persons. Lanes MP, molecular weight marker; B2, control Brucella abortus biotype 2; H1, human sample 1 (Ec-CIZ-Hum-1); H2, human sample 2 (Ec-CIZ-Hum-2); (*) samples from complementary studies at CIZ; CB, blank control.
RB, Rose Bengal test; SAT-EDTA, Wright's slow agglutination test with EDTA; iELISA, indirect enzyme-linked immunosorbent assay.
Blood culture.
H2S, hydrogen sulfide.
Retrospectively, seropositive persons (n=70) were queried about possible symptoms related to brucellosis. A summary of the outcome based on the questionnaire is presented in Table 7.
Discussion
The current study aimed to provide a reliable estimation of the seroprevalence based on the detection of antibodies against Brucella spp., the isolation and the identification of the circulating strain of Brucella spp., and the identification of possible risk factors related to the transmission and spread of brucellosis among people in the northwestern part of Ecuador.
Prevalence of human brucellosis in the northwestern part of Ecuador
In the current study an overall seroprevalence of 1.88% (CI 1.48–2.38) was found, which may be in sharp contrast with the official data of the Ecuadorian Ministry of Health (MSP), i.e., only 67 cases between 2003 and 2007 (EPI-2 2008). The results of the present investigation, and additional observations described by Ron-Román et al. (2012) in humans, as well as a seroprevalence of 2% in bovines from the same study area, and numerous isolations of Brucella spp. from different animal reservoirs (bovines and canine; unpublished data), suggest an underreporting of human brucellosis in Ecuador, considering that 36% of the population lives in rural areas (Organización Panamericana de la Salud 2008).
Based solely on clinical symptoms, a correct diagnosis of brucellosis is not possible (Abdoel and Smits 2007, Saegerman et al. 2010), and even microbiological blood cultures are sometimes unreliable because sensitivity is too variable and too dependent on the stage of infection (i.e., acute stage) and the Brucella species concerned (Casao et al. 2004). The difficulties related to the diagnosis and the often ambiguous or even absent clinical symptoms, also noted in the present study, are probably the principal reasons for the subnotification (Serra and Godoy 2000, Agasthya et al. 2007). The nonexistence of a vaccine against brucellosis in humans or the difficulty to access a safe and efficacious vaccine implies that controlling this zoonotic disease in animals will directly benefit its prevention in humans especially to improve the biosecurity. A joint work between the Ecuadorian Ministries of Public Health (MSP) and the Livestock, Aquaculture and Fisheries (MAGAP) is needed to consolidate a “One Health” initiative.
Risk factors for human brucellosis in the northwestern part of Ecuador
The occupations that expose people to the infection are male dominated in this study region, thus the apparent increased risk for infection. Several other studies have indicated gender as a significant risk factor for brucellosis (Wassif et al. 1992, Shehata et al. 2001, Mantur et al. 2007, Meky et al. 2007). The apparent elevated risk associated with older age groups could be explained simply by the fact that older people had more occasions to contract the disease (Cooper 1992, Kalaajieh 2000). Nevertheless, it is important to mention that three cases were also found in children below 15 years old, confirming the findings of Guevara et al. (2009) that children are indeed at risk and also do get the infection, e.g., due to direct or indirect contact with animals when accompanying adults handling livestock (Minas et al. 2007) or through consumption of nonpasteurized dairy products (Issa and Jamal 1999).
Brucellosis is mainly an occupational disease, and the multivariate analysis indicated that the odds of brucellosis seropositivity among those working in slaughterhouses were higher than those of people in the general population. This is in line with the results of other studies (Omer et al. 2002, Rahman et al. 2012). The higher seroprevalence among slaughterhouse workers confirms the proposition that intimate contact with animals is more important than consumption of infected dairy products (McDevitt 1971).
According to the World Health Organization (2006), temperatures for pasteurization or boiling milk should be sufficiently high to eliminate bacteria and to render it fit for consumption. Nevertheless, the relation between transmission of brucellosis and raw milk consumption in the present study was not statistically significant, which is in line with Serra and Godoy (2000), who reported no link between the presence of antibodies against Brucella spp. and the unhygienic consumption of milk. This lack of an association between consumption of milk or dairy products and infection may also be due to the low number of seropositive people found in our study that consumed these products.
The nonsignificance of the consumption of cheese squares with findings from Barroso-García et al. (2007), where it was observed that the consumption of cheese is not necessarily a source of infection of brucellosis because processing takes a few days or even weeks, affecting the number of bacteria, which was also indicated in this study. However, this information depends largely on the maturation process of each cheese considered and thus caution is recommended.
In general, the shedding of B. abortus in cows naturally infected is lower (<103 colony-forming units [cfu]/mL for several weeks but decreasing after the partum) than for Brucella melitensis in small ruminants (in general>103 cfu/mL during all the lactating period) (Carpenter and Boak 1928, Grilló et al. 1997, Hamdy and Amin 2002, Saegerman et al. 2010). In addition, the human pathogenicity of B. abortus appears lower than B. melitensis (Godfroid et al. 2010). These elements are other possible explanations for the lack of evidence found in this study considering the link between consumption of milk and dairy products and brucellosis infection.
Traditionally, milk and dairy consumption without any sanitary measures has been considered the most important route of transmission. However, recent reports stress the prominent role of transmission by direct contact with animal reservoirs (Barroso-Garcia et al. 2007, Godfroid et al. 2010, Saegerman et al. 2010). A national program exists in Ecuador. The main objective is to obtain brucellosis-free farms on a voluntary basis. In fact, this program is restricted to some farmers that are able to pay for the vaccination of calves with the B19 or RB51 vaccine, to test animals every 6 months, and to eliminate infected animals without compensation (most often at the slaughterhouse). In addition, no control of animal movements is performed and control of dairy farms by milk ring test (MRT) is not systematized and suffers from the lack of availability of antigen. However, the milk marketed in the cities by companies is usually pasteurized. However, raw milk is sold frequently in rural and periurban areas. This study has not demonstrated the importance of raw milk consumption in the human brucellosis transmission in Ecuadorian conditions. However, serial isolation of B. abortus (n∼100) from bovine raw milk of the same area (Ron-Román et al., unpublished data) indicates that the risk exists and needs future additional investigation.
Not surprisingly, the consumption of fetus or placentas was significantly associated with brucellosis seropositivity. This alimentary tradition, although largely obsolete, is still commonly used by rural families, and even in public restaurants that offer Ecuadorian typical dishes called fetus (locally known as “ville”) or placentas (locally called “guagua mama–huagra mama”). This meat is cooked, but handling of this food item increases risk of exposure to Brucella spp. Unfortunately, the consumption of blood was not significantly associated with brucellosis seropositivity in Ecuadorian context. However, this practice can be at risk, but necessitates a donor in the acute phase of brucellosis, which is not frequent (Thiange et al. 1992).
Education and health campaigns should target the elimination of such practices. It has indeed been observed in the population of the northwestern part of Ecuador that risks related to eating habits are mostly due to a lack of basic knowledge about brucellosis and the modes of transmission.
Typifying of circulating Brucella spp. in northwestern Ecuador
Biotyping Brucella is important for the epidemiological knowledge, because it can reveal geographical characteristics (FAO and OMS 1986) and allows a better understanding of the spread of the disease (Roux 1979). Unfortunately, isolating and typing of Brucella spp. is not always possible because it requires high biosecurity laboratories and trained personnel. Furthermore, the low number of successful isolations in the present study is mainly due to the low number of patients with acute brucellosis (i.e., with high levels of IgM antibodies) and also partly due to the localization of the bacteria in specific tissues and organs like bone marrow, cerebrospinal fluid (CSF), liver, kidneys, and spleen, which renders isolation from blood very unlikely (Doganay and Aygen 2003).
In the present study, 24.29% of the persons with a positive seroreaction showed no apparent symptoms at all. This is lower than the 45.6% reported by Pila-Perez et al. (1997) and the 99% found in a retrospective study of the symptomatology by Hernández et al. (1999). Although according to Pappas et al. (2006), based only on few reported data, Ecuador was not considered an endemic country for human brucellosis, the present results based on factual data contradicts this statement, especially in rural areas where 36% of the population lives. A recent report presented a systematic review of the scientific literature published between 1990 and 2010 relating to the frequency of human brucellosis in the world indicated that underestimation of the disease could be related to barriers in accessing health care or to case mismanagement and misdiagnosis (Dean et al. 2012). In Latin America, according to the previous report, reliable information was found only for Argentina and Mexico at the subnational level.
Conclusions
The absence of a National Policy and differential diagnostic tests hinders the development of surveillance and control programs in high-risk areas for human brucellosis (especially in rural areas). Thus, it is difficult to have a realistic idea about the incidence of this disease. In the past, little attention was given to brucellosis in Ecuador. It is necessary to develop programs to control (and eventually eradicate) brucellosis in the identified risk areas; highly sensitive diagnostic methods should be used both for humans and for animals with the objective of obtaining an early warning system and determining the correct prevalence at national level.
In view of the results of this study, there is an urgent need for information campaigns, especially in rural areas, about the risks involved following direct contact with livestock and consumption of fetus and placenta, and equally about the preventive care as to avoid infection. Also, more investigations to isolate and identify the biotypes of Brucella spp. circulating in Ecuador should take place. Finally, it is of utmost importance that evidence-based information be given to national and international donor organizations involved with future prevention and control and research programs on brucellosis.
Footnotes
Acknowledgments
We thank the patients for their willingness to participate in this study. This work was supported by the Belgian Cooperation in the framework or the Institutional Collaboration between the Institute of Tropical Medecine in Antwerpen, Belgium and the International Centre for Zoonoses (CIZ) of Central University of Ecuador.
Author Disclosure Statement
The authors declare that there are no competing financial interests.