
Abstract
Background:
While several studies conducted on Lyme borreliosis (LB) risk in the United States showed an association with environmental characteristics, most of European studies considered solely the effect of climate characteristics.
Objectives:
The aims of this study were to estimate incidence of erythema migrans (EM) in five regions of France and to analyze associations with several environmental characteristics of the place of residence.
Methods:
LB surveillance networks of general practitioners (GPs) were set up for a period of 2 years in five regions of France. Participating GPs reported all patients with EM during the study period. Data were pooled according to a standardized EM case definition. For each area with a participating GP, age-standardized incidence rates and ratios were estimated. Associations with altitude, indicators of landscape composition, and indicators of landscape configuration were tested with multivariate Poisson regression.
Results:
Standardized estimated incidence rates of EM per 105 person-years were 8.8 [95% confidence interval (CI)=7.9–9.7] in Aquitaine, 40.0 (95% CI 36.4–43.6) in Limousin, 76.0 (95% CI 72.9–79.1) in the three participating départements of Rhône-Alpes, 46.1 (95% CI 43.0–49.2) in Franche-Comté, and 87.7 (95% CI 84.6–90.8) in Alsace. In multivariate analysis, age-adjusted incidence rates increased with the altitude (p<0.0001) and decreased with forest patch density (p<0.0001).
Conclusion:
The marked variations in EM risk among the five regions were partly related to differences in landscape and environmental characteristics. The latter may point out potential risk areas and provide information for targeting preventive actions.
Introduction
The risk of LB is linked to human activities in areas with high densities of infected ticks. Deciduous or mixed woodland, occasionally coniferous, with a substantial understory and a layer of decaying vegetation on the ground, provides sufficient humidity for the development and survival of ticks and supports a range of potential vertebrate reservoir hosts (Stanek et al. 2012).
The role of environmental factors in the spatial variation of incidence of human cases of LB has been thoroughly studied in the United States (Killilea et al. 2008), specifically in Maryland (Glass et al. 1995, Jackson et al. 2006) and in southern Connecticut (Brownstein et al. 2005). These studies found a positive correlation between LB incidence and forest cover and positive or negative correlation between LB incidence and forest fragmentation.
Several epidemiological studies conducted in Europe have considered the effect of climate characteristics (such as precipitation, temperature, climate change) on LB risk (Estrada-Pena et al. 2006, Estrada-Pena 2009a, Jaenson et al. 2009, Jaenson and Lindgren 2011). But environmental variables have been studied by considering their effects solely on the density of infected ticks and not on the risk of human disease (Estrada-Pena 2009b, Halos et al. 2010, Richter and Matuschka 2011). These studies found a positive correlation between acarological risk and forest fragmentation in Europe. Same correlations have been highlighted in the United States (Allan et al. 2003, Brownstein et al. 2005).
In France, the French National Institute for Public Health Surveillance (InVS) classifies LB as an emerging disease and it is therefore a priority for surveillance and action. Since 2001, five regions of France (from west to east: Aquitaine, Limousin, Rhône-Alpes, Franche-Comté, and Alsace) have implemented active surveys of human cases of LB, based on previous local studies and physicians' interest in the topic (InVS 2005, Schmitt et al. 2006). The aims of this study were to estimate incidence of EM in the five regions and to analyze associations between incidence of EM and several environmental characteristics (indicators of topography, landscape composition, and landscape configuration) to provide information that could target preventive actions in potential risk areas.
Material and Methods
Surveillance networks
Between 2001 and 2012, five of the InVS's 17 interregional epidemiology units (which are known as Cellules de l'Institut de veille sanitaire en région or Cire) implemented surveillance networks to monitor regional incidence of LB over a 2-year period. The five surveillance networks were set up using the same design: All physicians who were thought likely to diagnose manifestations of LB were invited to participate and to report every LB case using a standardized questionnaire. They were asked every month for completeness of record. All patients were informed by their physician about the nature and aims of the study and agreed to participate. Each survey was approved by the Commission Nationale de l'Informatique et des Libertés (CNIL), the national ethical authority. For the five regions, a total of 1065 general practitioners (GPs) voluntarily took part in the surveillance, free of charge. GPs participation rates in the surveillance networks were 6.0% in Aquitaine (242 GPs), 17.3% in Limousin (170 GPs), 9.6% in Rhône-Alpes (163 GPs), 19.1% in Franche-Comté (203 GPs), and 14.2% in Alsace (287 GPs).
Territories and population covered by the surveillance networks
France, excluding its overseas territories, is made up of 22 regions, which are divided into 95 départements. Each département is subdivided into several cantons, made up of one or several municipalities. For the five regions under surveillance, 380 cantons each with at least one participating GP were included in our study, representing 115 of the 232 cantons (50%) in Aquitaine, 68 of 96 (71%) in Limousin, 67 of 111 (60%) in the three départements surveyed in Rhône-Alpes, 72 of 115 (63%) in Franche-Comté, and 58 of 64 (91%) in Alsace. In total, 79% of the population within the five regions, representing 6,927,675 inhabitants (2006 national census) was covered by the surveillance networks.
Patients and data collection
To ensure homogeneity between the five surveillance networks, a case was defined as a person diagnosed with EM equal to or greater than 5 cm in diameter (Stanek et al. 2011), reported by a GP participating in the surveillance networks. Data collected for each case were: Age, sex, clinic form of LB, place of residence, and, only in Franche-Comté, place of exposure.
Environmental data
In all cantons under surveillance, several variables describing the landscape and the environmental context of cantons were considered: Indicator of topography (altitude in meters), indicators of landscape composition (percentage of land covered by forest, percentage of hardwoods in forests), and indicators of landscape configuration [forest patch density (number per 100 hectares), mean size of forest patches (hectares), and forest edge density (meters par hectare)]. Patches are continuous areas of forest. The land cover data were obtained from the CORINE Land Cover 2006 produced by France's Department of Observation and Statistics and the European Environment Agency, available on the website of the French Ministry of Ecology Sustainable Development and Energy. Forest fragmentation data came from the Morphological Spatial Pattern Analysis, available on the website of the European Commission's Joint Research Centre. Relief data were obtained from the Shuttle Radar Topography Mission, available on the website of the Consultative Group on International Agricultural Research Consortium for Spatial Information. All environmental data at the canton level were categorized using tertiles; because mean altitude differed slightly between cantons, the first and the second tertiles of mean altitude were aggregated.
Statistical analysis
Description of reported cases and study of place of exposure
Reported cases were described by age and sex. The concordance between the place of exposure and the place of residence was studied in Franche-Comté.
Estimation of incidence rates
In each surveyed canton, observed cases were defined as all cases reported by a participating GP and living in the surveyed canton. All observed cases in people living in the same canton of residence were aggregated. The extrapolated number of cases by canton was calculated according to the method of the Sentinelles Network, i.e., extrapolated to the whole canton by multiplying the mean number of observed cases per participating GP by the total number of GPs practicing in the canton (Flahault et al. 2006). The extrapolated numbers of cases were tabulated into 25-year age classes and added up in each region. Regional crude incidence rates of EM were calculated using the extrapolated number of cases with the person-years denominators being the sum of population estimates in each canton covered by the surveillance networks for the 2-year period. Age world-standardized incidence rates of EM with their 95% confidence intervals were calculated for the five regions and for each canton group defined by tertiles of environmental characteristics.
Variation of incidence rates between areas
Standardized incidence rates ratios (SIR) and their 95% confidence intervals were also estimated by cantons, comparing the extrapolated number of cases with the expected number. The latter was calculated by applying the age-specific incidence rate, estimated for the whole surveyed population of the five regions, to the number of person-years surveyed in each canton. Cantons were then classified into three groups according to the values and the significance of SIR: Cantons with SIR significantly lower than 1, cantons with SIR not significantly different from 1, and cantons with SIR significantly higher than 1.
Association between environmental characteristics and EM incidence
Analyzed cantons were the cantons of residence of reported cases. Environmental data of studied cantons were compared between regions.
Univariate analysis
All environmental variables, classified into tertiles, were linked with estimated incidence data tabulated by cantons. For each variable, age-adjusted risk ratios (RRs) were estimated using Poisson regression. A population offset weighted by the participation rate of physicians in the surveillance network and a scale parameter taking into account overdispersion were used in modeling. Each environmental characteristic was included as unique explanatory variable in the regression and tested for significance by using the log-likelihood ratio statistics.
Multivariate analysis
Only variables with a p value lower than 0.20 in univariate analysis were retained for multivariate analysis. A backward selection procedure was applied using the log-likelihood ratio statistic to assess the independent effects of factors on EM incidence. A final model was retained through the minimization of deviance and overdispersion scale parameter. Model simplicity has been considered using the Akaike Information Criterion (AIC) (Diuk-Wasser et al. 2012). Validation of the final model was analyzed by estimating sensibility and specificity for identifying cantons at high risk of EM.
Analyses were performed with the SAS 9.3 software for Windows (The SAS Institute Inc., Cary, NC, USA). Mapping was carried out using a geographic information system (Arc GIS-ESRI).
Results
Description of reported cases and study of place of exposure
In the five regions, participating GPs reported 1453 cases of EM equal to or greater than 5 cm in diameter during the study period. Gender and age characteristics of reported cases are shown on Table 1. Gender ratio did not significantly differ between regions, but there were significant differences in age distribution (χ2=35.4; p<0.001).
Gender unknown for 6 patients (Rhône-Alpes 4, Franche-Comté 2).
Age unknown for 20 patients (Limousin 12, Franche-Comté 2, Alsace 6).
Among the 277 cases in Franche-Comté, the place of exposure was known for 169 persons. This place was the canton of residence for 78% of them. The places of exposure were dispersed for the others.
Estimation of incidence rates
The extrapolated number of cases was 8127. For men and women, estimated incidence rates of EM varied according to age (Fig. 1) and peaked between 60 and 64 years. Crude estimated incidence rates of EM in the five regions varied from 9.3 in Aquitaine to 100.2 cases per 105 person-years in Alsace. The world population's standardized incidence rates of EM varied from 8.8 in Aquitaine to 87.7 cases per 105 person-years in Alsace (Table 2).
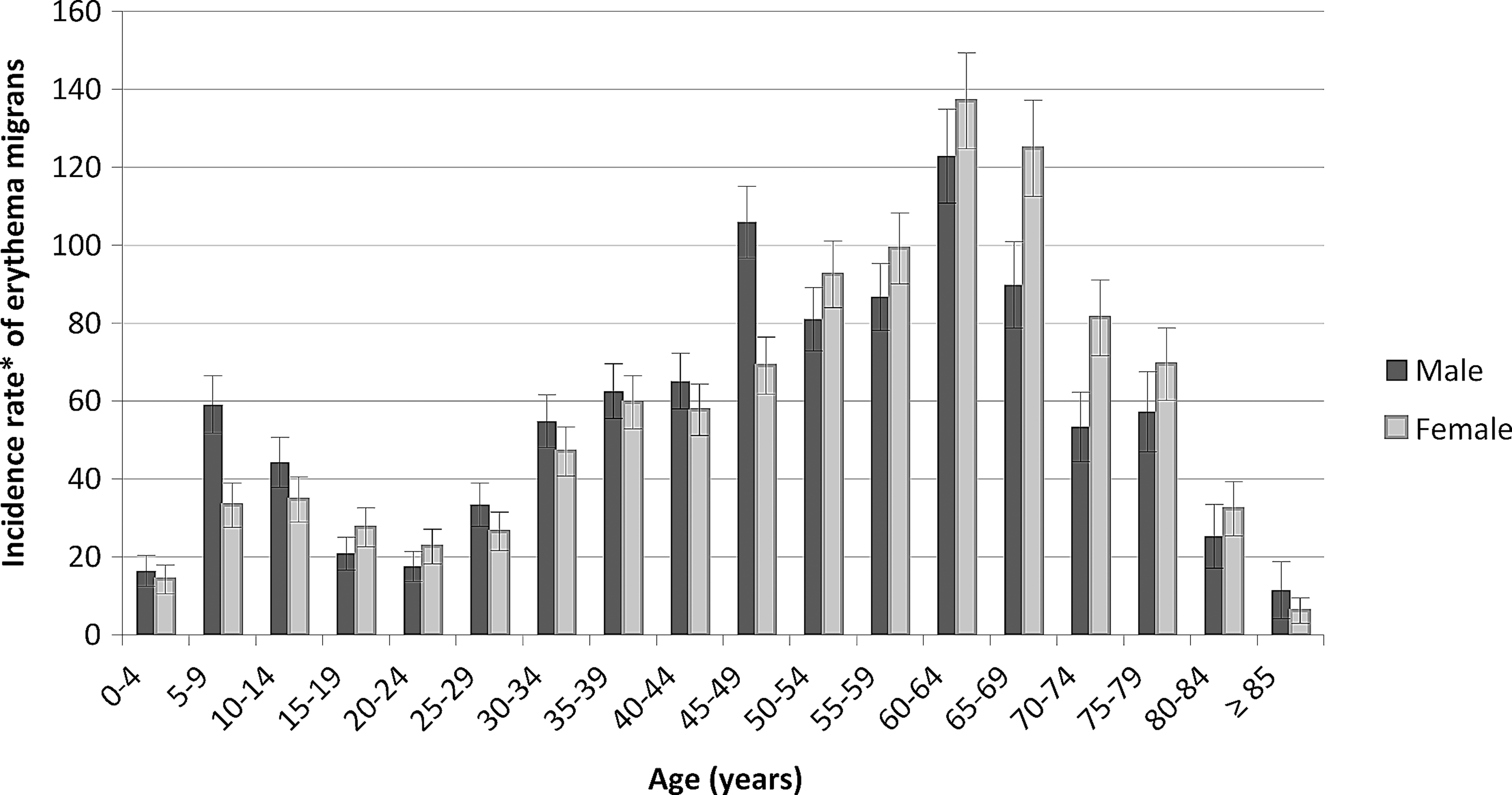
Age and sex-specific estimated incidence rates of erythema migrans in the studied areas. (*) Cases per 105 person-years. Bars are 95% confidence intervals.
Only three out of eight départements were included in the network.
Obtained by extrapolating based on rates of GP's participation in the network.
World population.
CI, confidence interval.
Variation of incidence rates between areas
The SIR distribution at the canton scale for each region is shown on Figure 2. More cantons with significantly high SIR were found in Alsace (n=33) and Rhône-Alpes (n=28) than in Franche-Comté (n=18), Limousin (n=11), or Aquitaine (n=6).

Standardized incidence rate ratios (SIR) of erythema migrans by cantons in the five regions of France.
Association between environmental characteristics and EM incidence
There were noticeable differences in environmental characteristics between the cantons and between the five regions. The mean of percentage of land covered by forest per canton ranged from 29.8% in Aquitaine to 42.3% in Franche-Comté. The mean percentage of hardwoods in forests ranged from 45.9% in Rhône-Alpes to 72.1% in Franche-Comté. There were also disparities in forest fragmentation; there were between 1.5 and 24.7 forest patches per 100 hectares, whereas the forest edge density ranged between 8.8 and 117.8 meters per hectare (Table 3).
Only three out of eight départements were included in the network.
Cutoffs are tertiles.
Univariate analysis
There were important variations in age-standardized estimated incidence rates according to environmental characteristics (Table 4). The risk of EM increased with the percentage of land covered by forest (p<0.0001), the altitude (p<0.0001), and the mean size of forest patches (p<0.0001). The risk of EM decreased with the percentage of hardwoods in forests (p<0.0001) and the forest patch density (p<0.0001). The risk of EM increased in the second category of forest edge density and decreased in the third category (p<0.0001).
Cut-points are tertiles, for altitude the two first tertiles are merged into the same category.
Log likelihood ratio statistics from Poisson regression.
IR, age-standardized incidence rates (world population); RR, adjusted incidence rate ratios, from Poisson regression including age; CI, confidence interval.
Multivariate analysis
Only the mean altitude and the forest patch density remained significant in the final model (Table 5). Using this model, sensibility/specificity percentages to identify EM incidence higher than 30 cases per 105 inhabitants were respectively 61%/74%; 60 cantons were found to be at high risk when forest patch density was lower than 1.5 patches per 100 hectares and altitude was higher than 393.5 meters, representing no cantons in Aquitaine, four in Limousin, 26 in Rhône-Alpes, 19 in Franche-Comté, and 10 in Alsace. Because of correlations between configuration and composition variables, other alternative models such as model using age, altitude, and mean size of forest patches per canton can be retained with AIC=246 but scale parameter=2.3.
Cut-points are tertiles, for altitude the two first tertiles are merged into the same category.
Log likelihood ratio statistics from Poisson regression: p≤0.001.
RR, adjusted incidence rate ratios, from Poisson regression including age; CI, confidence interval; AIC, Akaike information criterion.
Discussion
Our study, based on networks of physicians, is the first exploration to analyze EM incidence and environmental factors in France. We highlighted that incidence of EM was higher in eastern than in western France. The Sentinelles Network, based on 1313 French GPs (2.2% of all GPs in 2011) and covering the entire state, found that the four regions with the highest incidence of LB in 2011 were Alsace, Rhône-Alpes, Franche-Comté, and Limousin (Réseau Sentinelles 2011). No cases were reported in Aquitaine. Our estimates were lower than those of the Sentinelles Network. However their estimates were calculated from just 64 cases declared by the Sentinelle GPs of the five regions, and their case definition was different. While we retained only EM, the primary form of LB, they retained all cases of LB.
Our work presents several limitations. We assumed that the case's canton of residence was the same as canton of exposure. This hypothesis seemed reasonable on the basis of questionnaires collected in Franche-Comté, but was not assessed in the other regions. Moreover, in Glass's study, cases were referenced to their place of residence because 87% of them declared a place of exposure identical to their place of residence (Glass et al. 1995).
We did not study spatial autocorrelation because the nonparticipation of GPs in some cantons results in a noncontiguous study area. Furthermore, participation rates of voluntary GPs differed between regions without being correlated with EM incidence.
We believe that mean altitude summarizes data better than minimum and maximum values because the intercanton variability and the intracanton variability of altitude are high. In our work, the altitude variable in two classes leads us to separate cantons globally at low altitude and cantons globally at high altitude with a threshold of 393.5 meters.
The final multivariate model revealed significant positive correlation between incidence of EM and altitude, and negative correlation between incidence of EM and forest patch density in France. This result is consistent with previous studies performed in the United States and in Italy in which the increase in altitude was associated with an increased risk of LB, except for altitude higher than 1300 meters (Glass et al. 1995, Rizzoli et al. 2002, Rizzoli et al. 2011). Moreover, previous works studied the effect of forest fragmentation. In southern Connecticut, LB incidence rates were negatively correlated with forest fragmentation (Brownstein et al. 2005). However, another study in 12 counties of Maryland found significant positive links between LB incidence and fragmentation (Jackson et al. 2006).
Our study revealed discrepancies between our results and acarological models. First, in Jouda's study and Diuk-Wasser's studies, acarological risk decreased with elevation (Jouda et al. 2004, Diuk-Wasser et al. 2010, Diuk-Wasser et al. 2012). We can explain this difference because altitude was modeled differently between our study and these three studies. In our work, altitude was categorized in two classes, with a cutoff at 393.5 meters. In Jouda's study, ticks were collected in three altitude thresholds (of 620, 740, and 900 meters), all being higher than our study cutoff. In Diuk-Wasser studies, altitude was modeled as a continuous variable. Second, density of infected nymphs increased with fragmentation in the United States and in France (Allan et al. 2003, Halos et al. 2010). Brownstein found a positive correlation between acarological risk and fragmentation on one hand, and a negative correlation between LB incidence rates and fragmentation on the other hand (Brownstein et al. 2005). He concludes that human disease incidence in the southern region of Connecticut is driven more by human exposure than by entomologic risk.
Because landscape structure is associated with both entomologic risk (tick density and tick infection prevalence) and human exposure (recreational activities) (Brownstein et al. 2005), environmental characteristics help us to appreciate the LB risk as a combination of the two components. Relationships between environment, vectors, and humans remain complex and have to be studied more in Europe to develop available strategies of prevention of LB.
Conclusion
Our estimations of age-standardized incidence revealed a high incidence in the regions located in the east of France. We confirm that in France a part of EM incidence can be explained by environmental characteristics. As suggested by the international literature, further simulation studies or spatial modeling will help to improve understanding of tick-borne disease in France within Europe and the design of further studies. Pointing out risk areas in which entomologic risk (tick density and tick infection prevalence) and individual behavior should be studied can contribute to targeting preventive actions.
Footnotes
Acknowledgments
We would like to thank the managers of interregional epidemiology units of the InVS: Christine Meffre in Lorraine-Alsace, Patrick Rolland in Aquitaine, Claude Tillier in Bourgogne/Franche-Comté, and Nathalie Encrenaz who collected the data in Rhône-Alpes. We also thank the regional agency of health of Franche-Comté, and all the physicians who participated in Lyme disease surveys. Finally, we thank Dr. Elisabeth Ferquel from the Pasteur Institute in Paris for helping us to understand LB ecology.
Author Disclosure Statement
No competing financial interests exist.