
Abstract
In April, 2011, the Q fever bacterium Coxiella burnetii was identified at a Washington farm where an abortion storm took place among goats. Soon after, Q fever cases were reported among visitors to the farm from Washington and Montana. A cross-sectional investigation was conducted among humans and goats associated with the index farm or with 16 other farms that purchased goats from the index farm or housed goats at the index farm for breeding purposes. Questionnaire data were analyzed, along with human and goat specimens collected for evidence of C. burnetii infection. Twenty-one persons (19%) of the 109-person cohort from Washington and Montana met the outbreak case definition of an epidemiologic link to the index farm and a C. burnetii Phase II immunoglobulin G (IgG) titer ≥1:128 by immunofluorescence assay. Seventy-one percent of cases (15 of 21) were symptomatic, compared with approximately 50% during previous Q fever outbreaks. National Q fever surveillance reports increase in frequency with age, but 29% (6 of 21) of cases during this outbreak occurred in children aged <14 years. Goat-specific Q fever risk factors included direct contact with a newborn (prevalence ratio [PR] 10.7; confidence interval [CI] 1.5, 77.4), exposure to a newborn that died (PR 5.5; CI 1.7, 18.2), exposure to a weak newborn (PR 4.4; CI 1.7, 11.6), living on a property with goats (PR 4.2; CI 1.3, 13.9), and direct contact with birth/afterbirth products (PR 2.8; CI 1.1, 6.9). Evidence of C. burnetii infection was detected in all 17 goat herds sampled (13 Washington, 3 Montana, 1 Oregon) by PCR and/or enzyme-linked immunosorbent assay. Following this investigation, Washington and Montana implemented a herd management plan to encourage best-management practices among livestock owners, reduce the potential for future outbreaks, and promote continued communication between state public health and agricultural authorities.
Introduction
Q
Cattle, sheep, and goats are the primary C. burnetii reservoir species linked to human Q fever outbreaks (Marrie and Raoult 1997). Infected animals can shed C. burnetii in their birth products or in other fluids, including feces, urine, and milk. C. burnetii can resist desiccation and survive in the environment for long periods of time before becoming airborne, at which point it can be carried for miles in the wind (Hawker et al. 1998, Tissot-Dupont et al. 1999). The risk of an epizootic is greatest when C. burnetii is introduced to an immunologically naïve herd; during the subsequent one or two birthing seasons, abortion rates within the herd can escalate (Berri et al. 2007). Such “abortion storms” lead to environmental contamination with C. burnetii at high concentrations and increased probability of human infection. In recent years, this sequence of events has led to notable human Q fever outbreaks associated with goat and sheep herds in, for example, Colorado (Bamberg et al. 2007), England (Wallensten et al. 2010), Bulgaria (Panaiotov et al. 2009), and, to a much larger extent, The Netherlands (Schimmer et al. 2008).
In May, 2011, a patient with flu-like symptoms tested positive for Q fever in Washington State and described similar symptoms in other household members. Days later, multiple cases of Q fever were reported in Montana, including the severe case of an 11-year-old child who developed a sudden-onset high fever, along with severe headache, sore throat, myalgias, and severe abdominal pain. The Washington and Montana cases were linked to exposure to goats that had originated from a single farm in Grant County, Washington (WA Farm A), where earlier that year an abortion storm occurred and C. burnetii–positive goat placental specimens were collected. We describe the epidemiologic investigation undertaken to describe the scope of the outbreak and identify the risk factors associated with human infection, and we detail the recommendations resulting from this investigation to help prevent similar outbreaks in the future.
Methods
Preliminary investigation and identification of epidemiologically linked farms
The owners of WA Farm A (the site of the abortion storm) were interviewed by the Grant County Health District (GCHD) about goat sales following the April, 2011 report of C. burnetii–positive goat specimens collected from their farm. No sales were reported at that time. In May, 2011, farms in Washington and Montana were linked to WA Farm A via goat purchases during independent investigations of the initial human Q fever case reports in each state. The owners of WA Farm A were then visited and interviewed by the Washington State Department of Health and the Centers for Disease Control and Prevention (CDC) to obtain a list of potential visitors to their farm since the abortion storm began and to review their sales records over the previous 12 months to identify additional farms that had purchased goats. As the list of farms with goats from WA Farm A grew, a cross-sectional investigation was designed to collect questionnaire data, along with human and goat specimens for laboratory analysis.
Human investigation
A written questionnaire was developed and administered in June of 2011 to a cohort of individuals epidemiologically linked to WA Farm A. The investigation cohort included residents, visitors, and neighbors of WA Farm A or of farms with recent human illness that purchased goats from WA Farm A or temporarily housed goats at WA Farm A for breeding purposes. Each laboratory-positive case and all residents of identified farms (with the exception of two farms for which contact information could not be obtained) were contacted to provide Q fever education, serology, goat testing, and the written questionnaire. They were also asked to provide contact information for additional visitors to their farms to be offered education and the opportunity to complete the questionnaire and provide serum specimens for testing. The questionnaire covered basic demographic information, medical history, and exposure history, including descriptions of contact with goats, sheep, and cattle since September 1, 2010. This date was chosen to include a period of approximately 4 months before the onset of the abortion storm to enable the detection of possible exposure risks associated with any potential human Q fever cases that preceded the abortion storm.
Human serum samples were collected from participants to quantify their Phase II C. burnetii immunoglobulin G (IgG) antibody titers by immunofluorescence assay (IFA), as described by Sawyer et al. (1987). Statistical analyses of questionnaire responses and human serological data were calculated with Epi Info 3.5.3 using the Fisher exact test or the Mantel–Haenszel chi-squared test.
For this outbreak, a case was defined as a person with a direct or indirect epidemiologic link to WA Farm A (e.g., a resident, visitor, customer, or neighbor) since September, 2010, and a C. burnetii Phase II IgG titer ≥1:128 by IFA from a commercial, state public health, or CDC laboratory. The outbreak case definition did not include a requirement for clinical illness, as previous reports indicate up to 50% of persons exposed to C. burnetii are asymptomatic (Dupuis et al. 1987) and the national case definition (Council of State and Territorial Epidemiologists [CSTE] 2009) permits classifying asymptomatic persons as cases on the basis of both confirmatory laboratory evidence and an epidemiologic link to other known confirmed cases.
Goat investigation and follow-up visits
Goat serum was tested for evidence of Phase I and Phase II C. burnetii IgG antibodies by enzyme-linked immunosorbent assay (ELISA) (IDEXX, Switzerland). Goat milk samples, vaginal swabs, and fecal swabs were tested for evidence of C. burnetii infection by quantitative polymerase chain reaction (qPCR). A positive qPCR result provides evidence that an animal was actively shedding bacteria at the time of sampling. The animal samples were tested by qPCR targeting the IS1111 insertion element, as described by Loftis et al. (2006). In most cases, serum and PCR specimens were collected from all goats on a farm; however, as the list of epidemiologically linked farms expanded, it was necessary to collect specimens from a subsample of goats from farms with large herds. A detailed paper describing the animal portion of this investigation is forthcoming.
Following the completion of the laboratory analyses of goat specimens, door-to-door visits were conducted in July and August of 2011 to previously unvisited neighbors within a 1- to 2-mile radius of the infected farms determined by serological and PCR evidence (i.e., farms with high C. burnetii seroprevalence and PCR-positivity detected in goat specimens) to pose a potential risk of exposure for humans (discussed below). These visits were designed to offer Q fever testing, to ascertain additional cases, and to educate the community about Q fever symptoms and prevention. All residences were provided Q fever informational literature and contact information for local health officials should they develop symptoms in the future or wish to discuss Q fever in more detail.
Results
Preliminary investigation, and identification of epidemiologically linked farms
The owners of WA Farm A reported abortions in 14 (28%) of 50 pregnant Boer goats in their herd, beginning in late December, 2010, and continuing into early 2011. C. burnetii was detected by immunohistochemistry on April 22, 2011, prior to any known human cases, in specimens collected at the farm from the placenta of a female goat with two stillborn fetuses. This finding was reported by the Washington Animal Disease Diagnostic Laboratory to the Washington State Department of Agriculture (WSDA), then via the Washington State Department of Health to the GCHD. On the same day, the GCHD issued a health alert instructing healthcare providers to question patients presenting with Q fever–compatible symptoms about their recent history of exposure to goats. Additionally, the owners of WA Farm A began notifying recent goat-purchasing customers of the presence of C. burnetii in their herd.
The first human Q fever case was reported on May 25 in a symptomatic Grant County patient (from WA Farm B) diagnosed by a physician who was aware of the county health alert. The patient had visited WA Farm A multiple times in recent months, had purchased goats from the farm, and reported illness in other family members. The patient also reported the loss of a female goat with two stillborn fetuses on their farm earlier in the spring. On May 29, the first Montana case was reported in a symptomatic Teton County child (from MT Farm A). The child's family reported purchasing goats from WA Farm A. The family also reported that one of the purchased goats had aborted triplets 2 weeks before the onset of the child's illness. Six additional persons in Montana reported exposure to goats at a Cascade County farm (MT Farm B), and five of these persons reported Q fever-compatible symptoms, with onset dates from late March to mid-May. The owners of this farm had traveled to WA Farm A to purchase goats on multiple occasions.
Interviews with the WA Farm A owners, and review of their sales records, led to an expanded list of epidemiologically linked farms. Goats sold by from WA Farm A were traced to 20 other farms in 14 counties across three states (Washington, Montana, and Oregon). The owners of 17 total farms (13 in Washington, including WA Farm A; three in Montana; one in Oregon) were contacted and agreed to participate in the outbreak investigation. Four farms, all in Washington, were not included in the investigation because the owners could not be contacted (two farms) or because of logistical/scheduling conflicts (two farms).
Human investigation
Overall, 109 persons were tested serologically. A total of 21 Q fever cases were identified (12 in Washinton, nine in Montana), equaling an attack rate of 19% among the cohort. One patient was diagnosed at the time of clinical presentation; all remaining cases were identified through the epidemiologic investigation or by patient-requested testing. Fifteen (71%) of the 21 cases were symptomatic. Four (19%) cases were hospitalized, and no deaths were reported. Fifteen (71%) cases were male and six (29%) were children aged <14 years, including a child with severe illness.
The questionnaire was administered to 105 of the 109 persons tested serologically, including 17 of the 21 cases. The four missing cases provided serum for testing (either to the outbreak investigation team or independently to a healthcare provider) but could not be reached to complete a questionnaire. All individuals approached during this portion of the investigation (i.e., the individuals with direct contact with a case and/or with goats from WA Farm A) agreed to participate, although the majority of individuals contacted during the subsequent door-to-door portion of the investigation refused (described below). The median age of the 17 cases completing questionnaires was 36 years (range, 7 months to 60 years). Median illness duration was 29 days (range, 2–135 days). The predominant clinical presentation among the 17 patients questioned was a flu-like illness. Fatigue and muscle pain were reported in 13 cases, followed by fever in 12 cases, and chills, cough, headache, stiff neck, back pain, and diarrhea each reported in 11 cases (Table 1). Severe headache was reported for a patient misclassified as a new-onset migraine sufferer and a patient who sought care for a possible infected tooth due to headache pain radiating to the jaw. Illness in five patients progressed to pneumonia. Onset of the earliest human Q fever case occurred in January, 2011, and onset peaked in May with six cases (Fig. 1). The number of cases then declined substantially, with two cases reported in June.
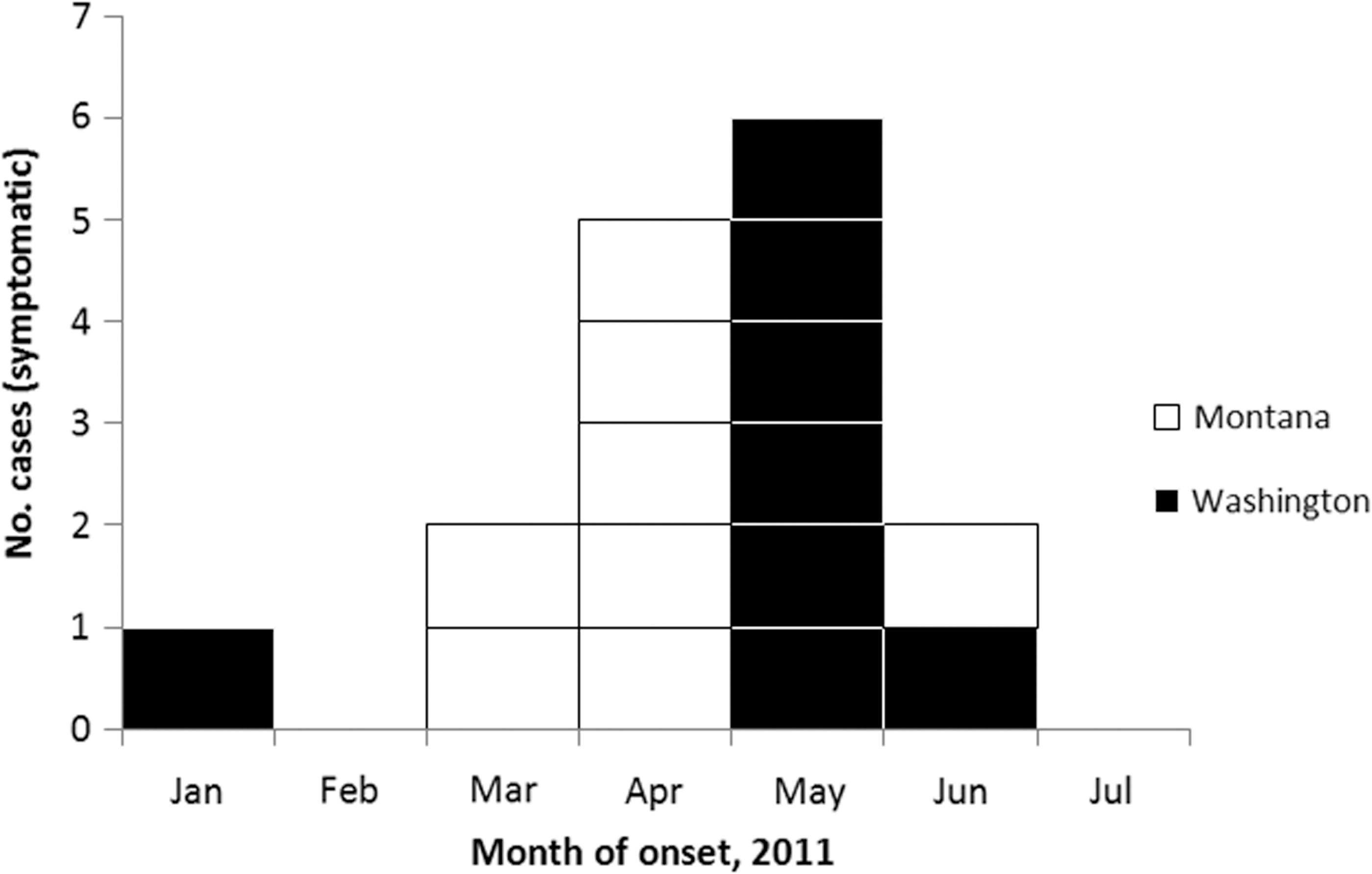
Epidemic curve of symptomatic cases during 2011 Q fever outbreak, by state. Note that only the 16 symptomatic cases are presented. The four Washington and one Montana asymptomatic cases are not presented in this figure because they lack a clinical date of onset.
Analysis of risk factors (Table 2) revealed that case status was significantly associated with male sex (prevalence ratio [PR] 2.74; confidence interval [CI] 1.0, 7.2) and with multiple goat-specific risk factors, including direct contact with a newborn (PR 10.7; CI 1.5, 77.4), exposure to a newborn that died (PR 5.5; CI 1.7, 18.2), exposure to a weak newborn (PR 4.4; CI 1.7, 11.6), living on a property with goats (PR 4.2; CI 1.3, 13.9), and direct contact with birth and/or afterbirth products (PR 2.8; CI 1.1, 6.9). Living on a property with cows was also significantly associated with C. burnetii seropositivity (PR 6.2; CI 2.6, 15.0). However, this is an unlikely source because 83% of cow owners also owned goats and there was no indication that cows were the source of transmission to humans during this outbreak. No other statistically significant cow-specific exposures were identified. Due to the small number of cases and high correlation between exposure variables, multivariate analysis was not feasible. Similarly, 16 of the 17 cases that completed questionnaires reported direct contact with a newborn goat. Statistically identifying less well-defined exposures (e.g., inhalation without direct contact) was therefore not possible.
Coxiella burnetii Phase II IgG IFA titer ≥1:128.
During September–June, 2011.
Sheep results are not shown because no significant results were found for sheep-specific risk factors.
CI, confidence interval.
Goat investigation and follow-up visits
C. burnetii infection was detected by PCR and/or serology in goats from 100% (17 of 17) of participating farms, including PCR confirmation of bacterial shedding in milk, feces, or vaginal mucus in 161 (24%) of 667 goats tested and seropositivity in 131 (21%) of 615 goats tested by ELISA. All identified human cases in Washington lived on, had visited, or had purchased goats from WA Farm A. The three Montana farms all had goats purchased from WA Farm A. Seven of the nine Montana cases lived on or had visited MT Farm B. The herds on WA Farm A and MT Farm B each had >70% C. burnetii seroprevalence and PCR evidence of bacterial shedding in >50% of goats. It is impossible to identify all potentially exposed persons during this outbreak given the airborne nature of C. burnetii and the inability of farm owners to recall all visitors to their farms. It was not feasible to visit all neighbors of all farms identified during this investigation, but the evidence suggested a higher risk of exposure for neighbors of WA Farm A and MT Farm B than of the other farms. For this reason, a return trip was made to visit all houses within a 1-mile radius of these two farms. All of these households received Q fever educational materials and contact information for local health officials if they wished to ask questions or participate in the investigation at a later date. This information was left on the doorstep when nobody was home. In Washington, 105 houses were visited, 65 within a 1-mile radius and 40 within a 1- to 2-mile radius of WA Farm A. No residents of these households volunteered to complete the questionnaire or accepted the offer to be tested for Q fever antibodies. In Montana, 67 houses were visited within a 1-mile radius of MT Farm B. Thirteen neighbors in Montana completed a questionnaire and provided serum for Q fever testing and are included in the analyses described above. All 13 individuals tested negative. Furthermore, no Q fever cases have been reported at or near any of the farms identified during this investigation since the 2011 outbreak, including WA Farm A or MT Farm B.
Discussion
This paper describes one of the largest Q fever outbreaks reported in US history and is the first documented multistate Q fever outbreak. Twenty-one human Q fever cases were identified among 109 persons known to be exposed to goats from WA Farm A. The male-biased prevalence of symptomatic Q fever observed in this outbreak is similar to previous studies and might result from the protective role of female sex hormones in limiting infection and granuloma formation (Roberts et al. 2001, Leone et al. 2004). In this outbreak, 75% of recognized cases reported symptoms compatible with Q fever, which is higher than the 50% level of symptomatic cases usually referenced in the literature (Dupuis et al. 1987). The observed higher symptomatic rate could be a result of having a small number of cases or a reluctance of healthy-appearing (though asymptomatically infected) individuals to be sampled. Another possibility is that the strain in this outbreak might have been more virulent, although there is currently no laboratory evidence to support this.
This outbreak warrants close attention for several reasons. First, national surveillance reports of Q fever increase in frequency with age, and cases in the literature and in national surveillance data are less commonly reported in children. Because of this, it has been postulated that children are less frequently symptomatic than adults if infected and may experience milder disease (Maltezou and Raoult 2002, McQuiston et al. 2006). However, 6 (29%) of the 21 cases from this outbreak occurred in patients under 14 years, and children presented with the most severe illnesses during the outbreak. Children might have been overrepresented among cases because the exposing animals were goats, specifically Boer goats, which are anecdotally popular “starter” animals for children learning how to care for livestock. A number of the farms investigated had purchased goats for their children's 4-H projects, for example. Second, this outbreak demonstrates the potential for disease transmission associated with interfarm transport of animals. Many states, including Washington and Montana, require an entry permit and certificate of veterinary inspection for imported goats. This is critical information needed during an animal outbreak response, but this was not obtained for any goats transferred to Montana that were investigated as part of this outbreak investigation.
Third, while only 21 cases were identified from Washington and Montana, the goat-associated outbreak that occurred in The Netherlands during 2007–2009 has demonstrated how quickly the scale of a Q fever outbreak can grow. In 2007, there were 168 notified cases in The Netherlands. In 2008, there were 1000 cases, and, in 2009, there were nearly 2500 notified cases (van der Hoek et al. 2010). The outbreak in The Netherlands was related to dairy goats rather than meat goats, and the environmental factors and industry farming practices that contributed to the spread of disease within The Netherlands are likely different compared with the Washington and Montana farms. Nonetheless, the current outbreak provides evidence that larger, multistate outbreaks of Q fever are possible in the United States. Risks may be difficult to minimize in an industry characterized by close human–animal contact and extensive inter- and intrastate animal movement, especially if these movements frequently occur without livestock owners maintaining accurate sales logs and required veterinary health documents.
Finally, the long median duration of illness and the previously undiagnosed symptomatic infections that were identified during this outbreak demonstrate the importance of promoting awareness among physicians. When patients present with compatible symptoms, the timing of diagnostic tests and treatment is crucial, although treatment should never be delayed pending laboratory results. Treatment is most effective if given with the first 3 days of symptoms and has been shown to decrease the duration and severity of illness (Powell et al 1962). Many patients in this outbreak suffered through longer illnesses than they would have if doxycycline had been prescribed promptly. For instance, an 11-year-old child from Montana with high fever, severe headache, sore throat, myalgias, and severe abdominal pain was first treated with amoxicillin/clavulanate but failed to improve. The illness became intermittent over the next 2 months, resulting in several visits to a healthcare provider. Then, after another episode of high fever and abdominal pain, the child was referred for a surgical consult, and an appendectomy was performed. The appendix was normal on pathological examination. After the appendectomy, the patient's symptoms continued, including high fever, for 2–3 weeks, and the patient was prescribed trimethoprim/sulfamethoxazole before finally recovering. The diagnosis of Q fever was not considered until the family was informed by the WA Farm A owners of the detection of C. burnetii in their goat herd. Immediate treatment with doxycycline could have accelerated recovery, reduced the severity of illness, and avoided an unnecessary appendectomy.
This investigation had the following limitations. First, background C. burnetii seroprevalence among humans or goats in Washington and Montana for comparison with the results obtained during the outbreak investigation was unknown. However, public health surveillance data shows that typically only zero to three human cases are diagnosed and reported annually in both states. Second, the majority of human Q fever cases identified during this outbreak would be classified as probable, not confirmed, according to the CSTE case definition criteria. Serological confirmation depends upon the demonstration of rising antibody titers between acute and convalescent specimens. Only one patient had a detectable four-fold rise between acute and convalescent samples and was therefore able to be classified as a confirmed case. Acute specimens were not drawn for most of the other cases because the majority of patients had already convalesced when identified. Third, the sales records reviewed for show goats were well maintained; however, the same was not true of goats sold for meat. This is typically a much more informal transaction, and the farm owners were unable to provide contact information for any of these potentially exposed customers, resulting in lost opportunity for follow-up. There were also two sales of show goats for which we were unable to obtain contact information for follow-up with the purchasers. Finally, due to the variable incubation time for Q fever, as well as the time that had elapsed since symptom onset for most cases, recall bias may be present in the questionnaire portion of this investigation.
Specific guidelines can be followed to decrease the risk of Q fever in humans and increase Q fever awareness in the medical and veterinary communities and the general public (see
Footnotes
Acknowledgments
We would like to thank the Q Fever Outbreak Response Group for their contributions to this investigation, including: Jill Boetcher, Trixie Smith, Alicia Thompson (Cascade City-County Health Department); Adam Beard, Scott Dahlgren, Kelly Fitzpatrick, Meagan Kay, Aubree Kelly, Rob Massung, Jennifer McQuiston, Jamie Perniciaro, Rachael Priestley, Joanna Regan, Josh Self, Joseph Singleton, and Sonja Weiss (CDC); Alex Brzezney, Jefferson Ketchel, Amber McCoy, and Lois Swenson (Grant County Health District); Carol Ballew, Tammy Buckley, Steven D. Helgerson, Jennifer Lowell, Jim Murphy, Walter Walsh, and Anne Weber (Montana Department of Public Health and Human Services); Emilio DeBess (Oregon Department of Human Services); Kim Bailey (RiverStone Health); Elaine Sedlack and Lora Weir (Teton County Health Department); Tom Brignole, Tom Gomez, Kammy Johnson, Yvette Leidorf, Eileen Ostlund, and Rolf Westly (United States Department of Agriculture, Animal and Plant Health Inspection Service, Veterinary Services); Leonard Eldridge, Jerry Pospisil and Ben Smith (Washington State Department of Agriculture); Tony Marfin and Ron Wohrle (Washington State Department of Health); and Sara Smith (Washington State University).
The findings and conclusions in this article are those of the authors and do not necessarily represent the official position of the funding agencies.
Author Disclosure Statement
No competing financial interests exist.