
Abstract
Malaria has never been endemic in New Zealand, and all cases have been diagnosed in international travelers. In this paper, we describe malaria cases reported from 1997 to 2009 and discuss epidemiological changes compared to a previous report from 1980 to 1992. From 1997 to 2009, 666 malaria infections were reported, with 410 cases (61.6%) in travelers aged 20–39 and 133 (20%) in military personnel. Infections were caused by Plasmodium vivax in 436 cases (72.7%) and Plasmodium falciparum in 163 (27.2%). In the 533 civilians, common countries of infection were Papua New Guinea (24.4%), India (18.6%), the Solomon Islands (8.8%), and Indonesia (6.1%). Most common regions of malaria acquisition for civilians were Papua New Guinea and Western Pacific (39.8%), Africa (24.7%), Indian subcontinent (19.5%), and Southeast Asia (13.6%). Compared to a previous report of malaria in New Zealand from 1980 to 1992, regions of malaria acquisition have changed significantly, with a lower percentage of cases acquired from Papua New Guinea and Western Pacific (from 59.2% to 39.3%), and a higher percentage from Africa (from 8.6% to 21.3%). The ethnic groups affected also differ significantly between the two surveillance periods, with a reduction in the percentage of cases reported in Caucasians (from 80.8 to 45.9%) and an increase in cases in Indians (from 7.0 to 15.7%), Papua New Guineans and Pacific Islanders (from 5.2 to 16.9%), other Asians (from 2.3 to 5.6%), and Africans (from 0 to 8.5%). Common locations of malaria infection have evolved over time and probably reflect changing travel patterns of New Zealanders and the origins of visitors and immigrants. Therefore, local surveillance is important for informing pretravel advice by identifying vulnerable groups and common destinations for malaria infection, so that special attention on malaria prevention can be focused on travelers who are at highest risk. Ongoing surveillance is also essential for monitoring the evolving epidemiology of imported malaria over time.
Introduction
G
Malaria is caused by infection with one of the four classical species of Plasmodium parasites (P. falciparum, P. vivax, P. ovale, and P. malariae) and the recently discovered Plasmodium knowlesi, and transmitted by bites of female Anopheles mosquitoes (Greenwood et al. 2005). Although malaria has never been endemic in New Zealand, it is an important cause of severe and potentially fatal illness and, along with dengue fever, the most common notified vector-borne diseases in returned travelers to New Zealand (Environmental Science and Research 2012). A 1996 report of malaria in New Zealand described 867 cases diagnosed from 1980 to 1992, mostly acquired from Papua New Guinea, the Solomon Islands, and Vanuatu (Kriechbaum and Baker 1996). Here, we describe cases of malaria reported in New Zealand from 1997 to 2009 and discuss epidemiological changes in the countries of malaria acquisition and ethnic groups affected compared to the 1980–1992 surveillance period.
Materials and Methods
In New Zealand, notification of malaria cases is mandatory, and all cases reported to the Notifiable Disease Surveillance System (NDSS) from 1997 to 2009 were included in this analysis. De-identified information on demographics, diagnosis date, travel history, occupation, Plasmodium species, malaria chemoprophylaxis, and notification source were obtained from the NDSS. Travel history included up to three recently visited countries/territories, and any malaria-endemic countries were recorded as the likely infection source. Countries of acquisition were grouped into regions: Papua New Guinea and Western Pacific, Southeast Asia, the Indian subcontinent, other Asia, Africa, and Central and South America.
In this article, we report the number of notified malaria cases per year, age and sex distribution of cases, countries and regions where infection was acquired, method of diagnosis, source of notification, hospitalization and death rates, use of chemoprophylaxis, Plasmodium species identified, ethnicity of cases, and ethnic groups who acquired malaria from each region. Analyses were performed separately for military cases because of differences in demographics and travel destinations. To examine changes in place of malaria acquisition and ethnic groups affected over time, the above findings were compared to a previous report of malaria in New Zealand from 1980 to 1992 (Kriechbaum and Baker 1996).
All variables were categorical, and proportions in each category were reported with 95% confidence intervals. Chi-squared tests were used to assess differences in (1) ethnic groups who acquired malaria in different regions, and (2) changes in the region of acquisition and ethic groups affected between the two surveillance periods. p values of <0.05 were used to indicate statistical significance.
Graphs were produced to show the annual variation in the number of cases, age and sex distribution, distribution of Plasmodium species in cases acquired from different regions, and distribution of ethnic groups in cases acquired from different regions.
Results
Table 1 provides a summary of the main findings. From 1997 to 2009, there were a total of 666 reported cases of malaria infections, equivalent to an average of 51 cases/year. Twenty percent (n=133) of cases were in military personnel. One death (0.2%) associated with P. falciparum was reported in a Somalian refugee who arrived in New Zealand 10 days previously. Although the overall mortality rate was low, of the 557 cases where hospitalization status was known, 51.3% required hospital treatment.
Gender was recorded in 644 cases. Males accounted for 98.3% of infections in military personnel and 71.3% in civilians. Most infections (61.6%) occurred in travelers aged 20–39 years. The largest number of cases (n=111) was diagnosed in 2000, with 70 (63.1%) of cases diagnosed in military personnel, predominantly acquired from East Timor. Figures 1 and 2 show the number of cases reported each year and the age and gender distribution of cases.
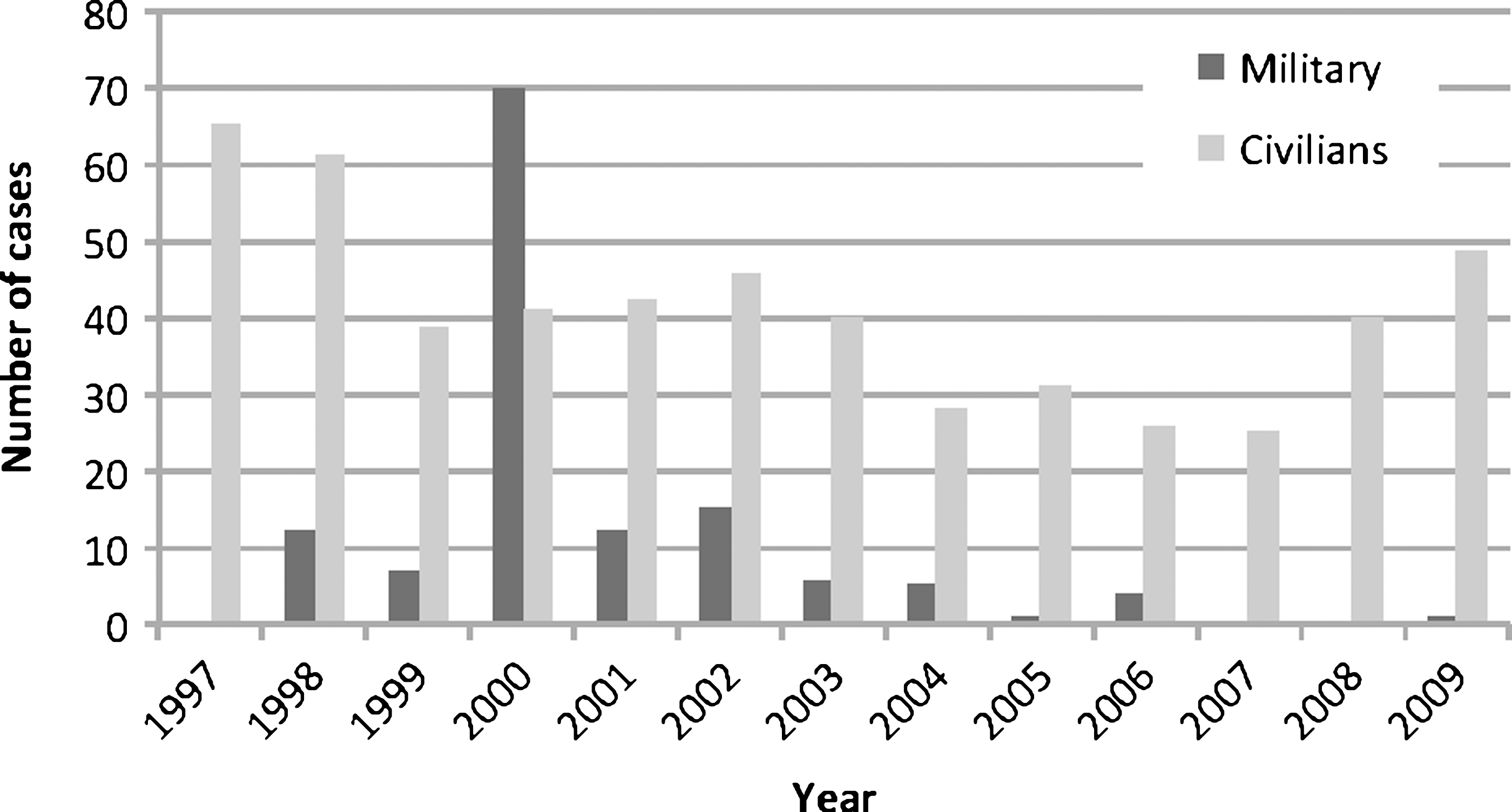
Reported cases of malaria in New Zealand: Years of diagnosis.
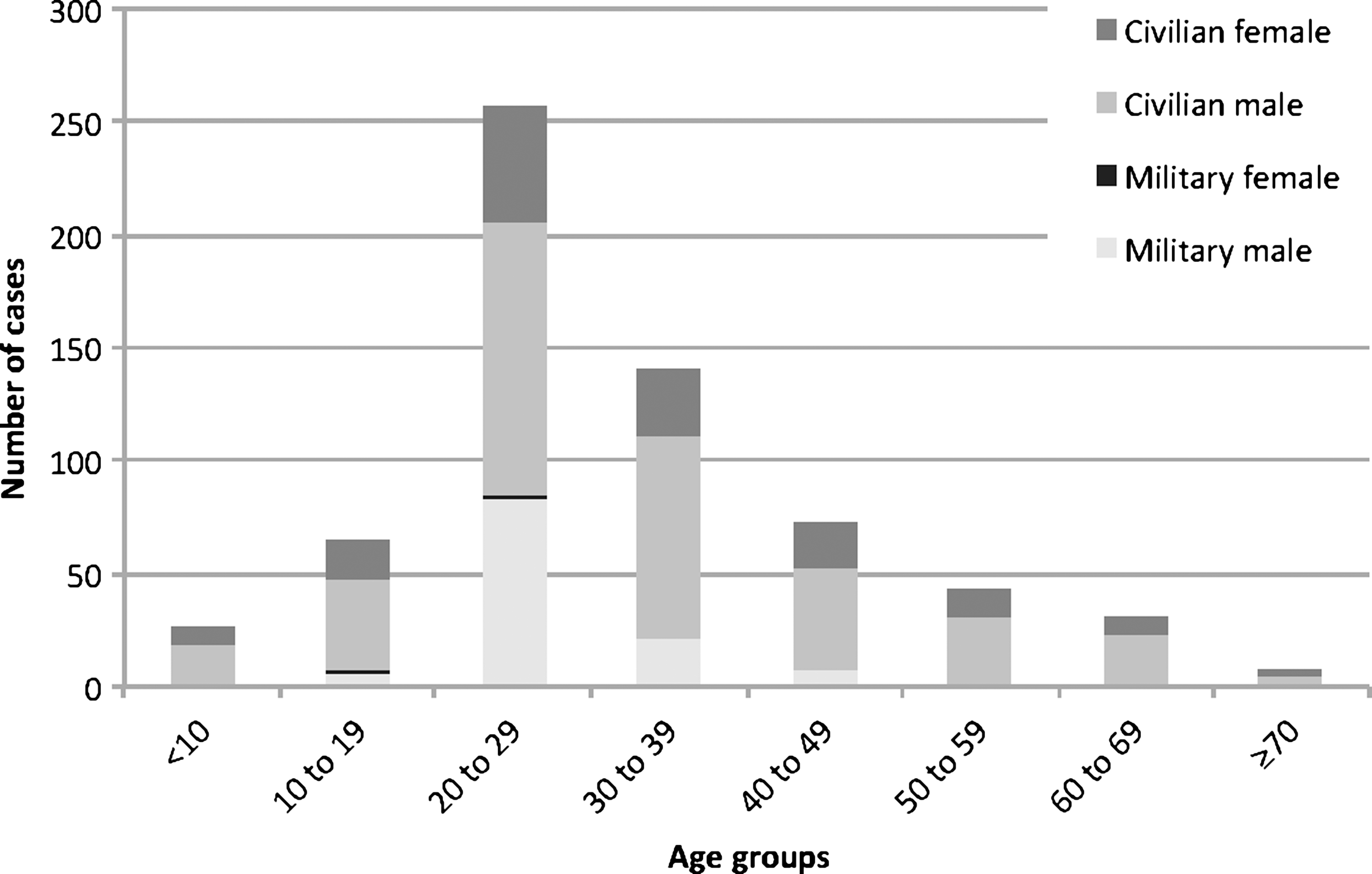
Reported cases of malaria in New Zealand: Age and sex distribution.
The country of malaria acquisition was recorded in 517 cases, and, of these, 75 cases were in military personnel and 442 in civilians. Of the military personnel, 24% acquired malaria from Papua New Guinea, 62.7% from East Timor, and 12% from the Solomon Islands. The most common countries from which civilians acquired malaria were Papua New Guinea (24.4%), India (18.6%), the Solomon Islands (8.8%), Indonesia (6.1%), and Vanuatu (5.9%). The most common regions of malaria acquisition for civilians were Papua New Guinea and the Western Pacific (39.8%), Africa (24.7%), the Indian subcontinent (19.5%), and Southeast Asia (13.6%). In 2000, of the 29 cases where country of acquisition was known, 96.6% were reported from military personnel who had traveled to East Timor.
Diagnosis was made on microscopy in 608 cases (91.3%), and the diagnostic method was unknown in the remainder. Of the 600 cases where the Plasmodium species was known, P. vivax was the most commonly identified and accounted for 89.9% of cases in military personnel and 68.4% of cases in civilians. Figure 3 shows variations in Plasmodium species acquired from different regions.
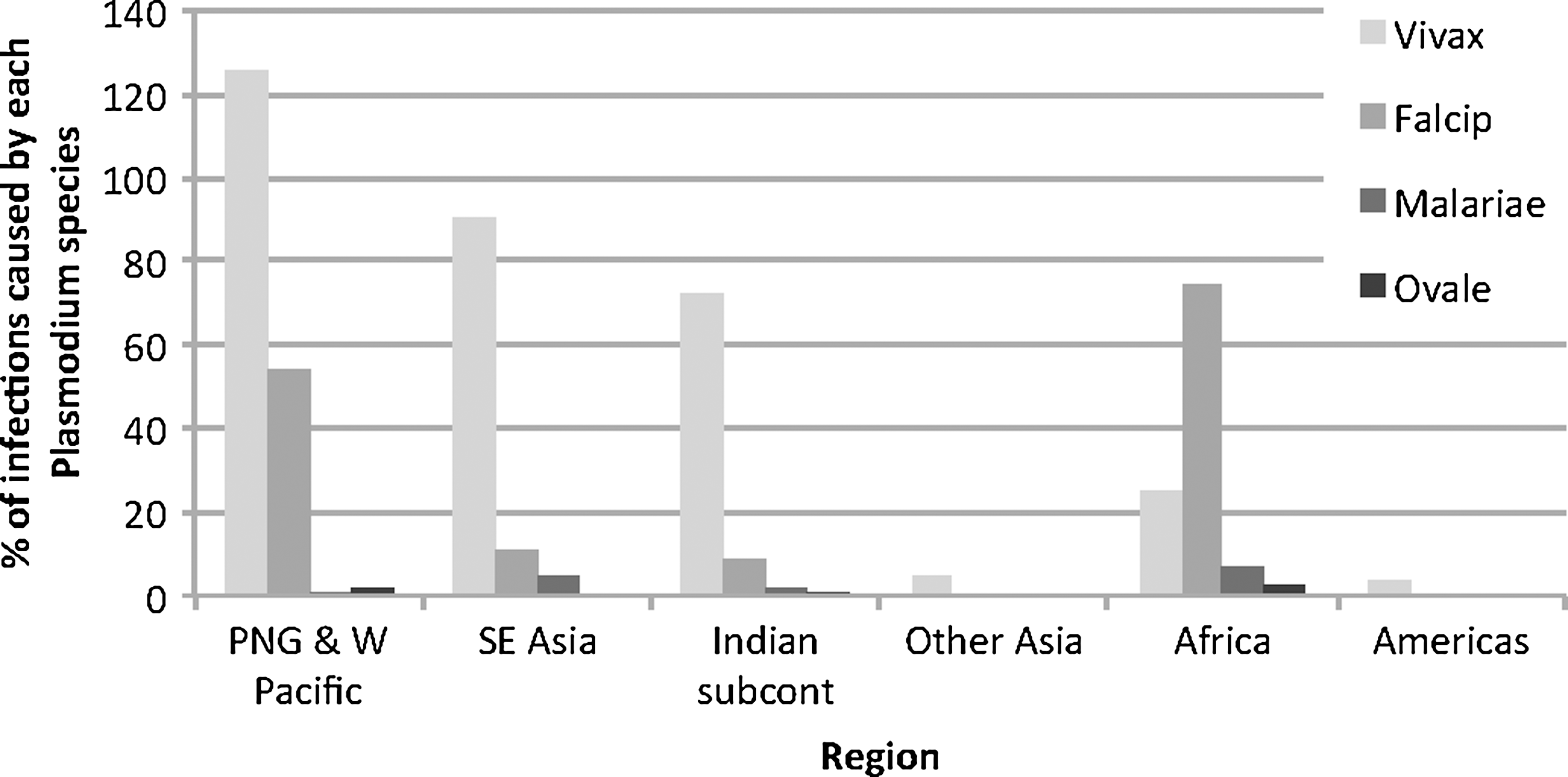
Plasmodium species by region where malaria was acquired.
For military personnel, ethnicity was recorded in 86 cases, and included 53.5% New Zealand Caucasians and 34.9% Māori. For civilians, ethnicity was recorded in 471 cases and included 36.7% New Zealand Caucasians, 18.5% Indians and Pakistanis, 10.2% Pacific Islanders, 10.0% Africans, and 7.9% Papua New Guineans. For civilians, ethnic distributions varied significantly between regions of acquisition (χ=759.5, p=0.00). Figure 4 shows that the majority of Papua New Guineans acquired malaria from Papua New Guinea, Pacific Islanders from the Western Pacific, Indians and Pakistanis from the Indian subcontinent, other Asians from Southeast Asia, and Africans from Africa.
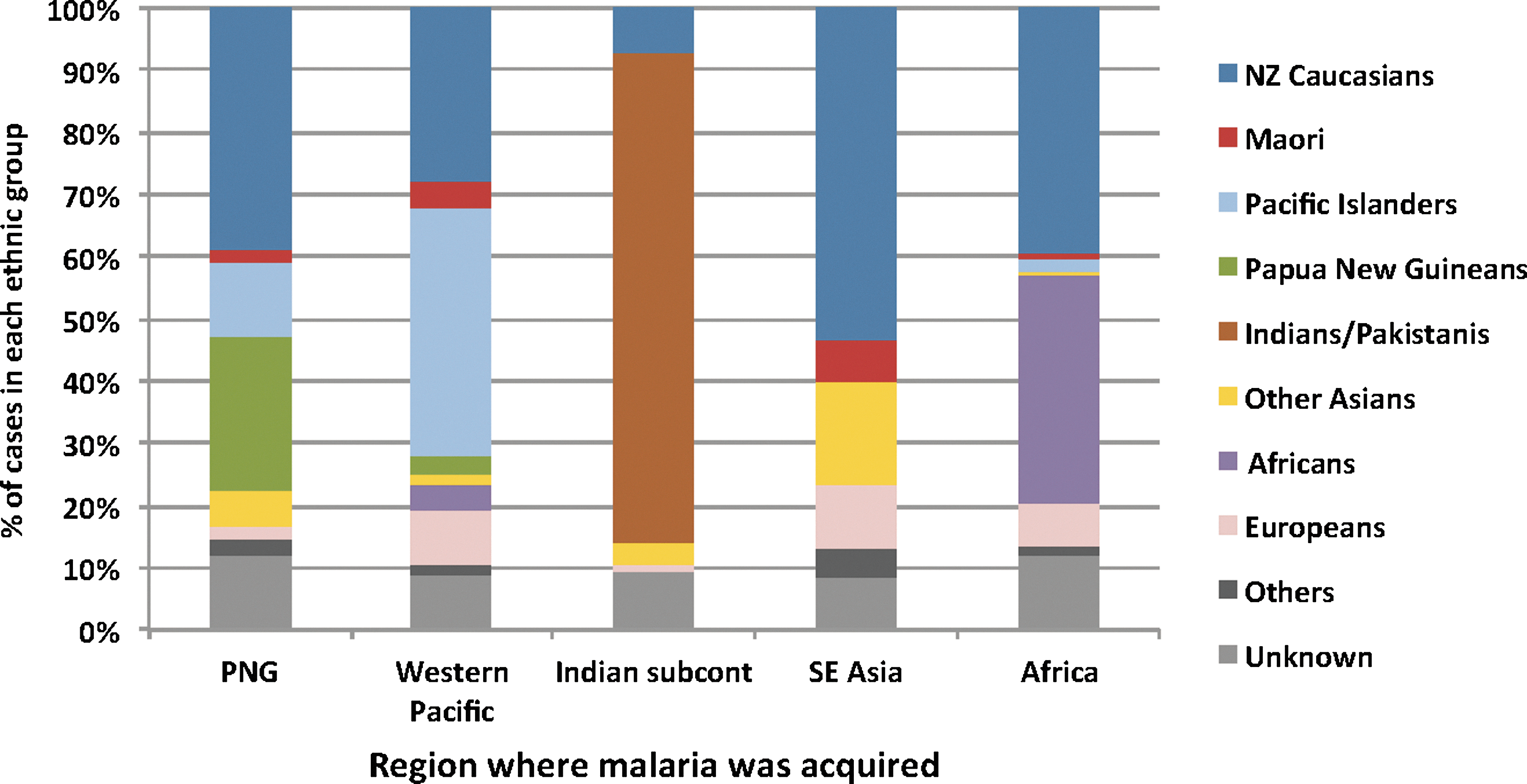
Ethnic distribution of malaria cases acquired from different regions: Civilian cases.
The notification source was known in 656 cases (98.5%). General practitioners reported 63.6% of military cases and 52.9% of civilian cases, and hospital-based practitioners reported 12.1% of military cases and 33.4% of civilian cases. Of 557 cases where hospitalization data were available, 60.3% of military personnel and 50.1% of civilians required hospital treatment. Hospitalization rates varied significantly with Plasmodium species (χ=17.9, p=0.00), with the highest rate was associated with P. falciparum (67.1%, 94 of 140 cases where hospitalization data were available), followed by P. malariae (58.8%, 10 of 17 cases), P. vivax (46.4%, 169 of 364 cases), and P. ovale (44.4%, 4 of 9 cases).
Unfortunately, little data were collected on chemoprophylaxis use or compliance. Data on whether chemoprophylaxis was offered were available for 57 cases, with only 40.4% confirming that they were offered prophylaxis. Data on whether prophylaxis was taken were available for 36 cases, with only 27.8% reporting taking prophylaxis.
A report of malaria cases in New Zealand from 1980 to 1992 (Kriechbaum and Baker 1996) found similar results, with an average of 67 cases/year, mostly in males (69.9%) and travelers aged 20–39 years (60.2%), hospitalization rate of 63.8%, mortality rate of 0.3%, and a predominance of P. vivax infections (70.9% of cases where species was known). However, there were statistically significant differences in the regions of malaria acquisition (χ=44.6, p=0.00) and the ethnic groups affected between the two surveillance periods (χ=189.7, p=0.00). Table 2 shows that from 1980 to 1992, the percentage of cases acquired from Papua New Guinea and Western Pacific significantly reduced from 59.2% to 39.3%, whereas the percentage of cases from Africa significantly increased from 8.6% to 21.3%. Cases from Southeast Asia and India were not significantly different between the surveillance periods. From 1980 to 1992, 80.8% of malaria cases were reported in Caucasians. From 1997 to 2009, the percentage of cases reported in Caucasians dropped significantly to 45.9%, while cases increased from 7.0% to 15.7% in Indians, 5.2% to 16.9% in Papua New Guineans and Pacific Islanders, 2.3% to 5.6% in other Asians, and 0% to 8.5% in Africans. To put the findings in context, New Zealand's population in 2006 consisted of approximately 77% Caucasians, 15% Māori, 10% Asians, 7% Pacific Islanders, and <1% other ethnicities (Statistics NZ 2006). Unfortunately, the surveillance data available did not provide sufficient information on travel details to allow calculation of the incidence of malaria in travelers, or differences in incidences between countries, regions, or ethnic groups.
Statistically significant differences between the two surveillance periods.
CI, confidence interval.
Discussion
Although malaria is not endemic in New Zealand, it is an important cause of severe illness in returned travelers. Findings in this study corroborate global reports that posttravel malaria is more commonly diagnosed in males and young adults (Leder et al. 2004). Males and young adults more often participate in outdoor activities, including military operations, and studies have found them to be less compliant with chemoprophylaxis (Cobelens and Leentvaar-Kuijpers 1997, Laver et al. 2001, Landry et al. 2006).
The predominance of P. falciparum in cases from Africa and P. vivax in cases from Papua New Guinea, Western Pacific, Southeast Asia, and India (Fig. 3) is consistent with known regional differences in Plasmodium species distribution (World Health Organization 2011). P. falciparum is known to cause more severe illness and deaths than the other species (World Health Organization 2011) and was responsible for one death and a higher rate of hospitalization in this study.
The most common acquisition countries (Papua New Guinea, India, East Timor, the Solomon Islands, Indonesia, and Vanuatu) and regions (Papua New Guinea and Western Pacific, Africa, Indian subcontinent, and Southeast Asia) reflect New Zealand's geographic location, travel destinations of New Zealanders, country of origin of New Zealand's visitors and immigrants, and military operational locations. Countries of origin of immigrants also influence the number of arrivals already infected with malaria, as well as future travel destinations when immigrants return home to visit families and friends. For example, the significant increase in the proportion of malaria cases diagnosed in Africans and/or acquired in Africa is likely to be directly related to the increase in immigrants arriving from Africa and the Middle East from 940/year for 1980–1992 to 4710/year for 1997–2009 (Statistics NZ 2012).
Findings in this study differ from a GeoSentinel report of malaria in returned travelers, where 75% of infections were acquired in Africa, with a predominance of P. falciparum (60%) (Leder et al. 2004). However, the GeoSentinel cases were predominantly diagnosed in Europe (50%) and North America (31%), where ethnicity of immigrants and destinations of travelers would differ from those in New Zealand. Therefore, local surveillance is important for providing country-specific data on common destinations for malaria infection.
In neighboring Australia, similar changes in the epidemiology of imported malaria have been noted, with increasing numbers diagnosed in immigrants (including those in detention centers) and cases acquired in Africa, and high risk of infection in military personnel (Boreham and Relf 1991, Robinson et al. 2001, Charles et al. 2005, Walker et al. 2005).
Travelers returning to home countries to visit family and friends (VFRs) have a higher risk of malaria and other tropical infections compared to tourists (Leder et al. 2006, Pistone et al. 2007, Pavli and Maltezou 2010, Checkley et al. 2012), and are therefore a major risk group for imported malaria to developed countries (Schlagenhauf et al. 2003, Pavli and Maltezou 2010), with children being at particularly high risk (Stager et al. 2009, Arnaez et al. 2010). A GeoSentinel survey of returned travelers found that immigrants and VFRs had 8.3 times the odds of malaria infection compared to tourists (Leder et al. 2006). Many factors contribute to the higher risk of illness in VFRs (Pavli and Maltezou 2010). They are less likely to take chemoprophylaxis and more likely to travel to rural areas, villages, and less developed areas where infection risks are higher, stay for extended periods of time, and exposed to local living conditions and hygiene standards. Some are unable to afford recommended chemoprophylaxis and vaccines, particularly when many family members are traveling. However, VFRs often perceive themselves to be at low risk because they are “just returning home,” and are less likely to seek pretravel advice. Many have had malaria while living in endemic areas, but are unaware of their waning immunity after living in nonendemic countries. In this study, data on the purpose of travel were not available, but Fig. 4 shows that ethnicity is strongly related to place of acquisition, suggesting that many cases are likely to be immigrants or VFRs. The number of New Zealand residents who traveled overseas as VFRs increased from 26,721 in 1999 to 46,183 in 2011 (Statistics NZ 2012), and VFRs are likely to continue to be an important group of travelers at risk of malaria.
Malaria is known to be a significant problem for military personnel due to the high exposure risk of their activities (Porter 2006, Elmes 2010). Factors associated with malaria risk in military personnel include compliance to chemoprophylaxis and other preventive measures, side effects from medications, perception of susceptibility to mosquito bites and malaria risk, lack of preventative medicine support, involvement in night operations, location of platoon positions, and general compliance within the group (Anonymous 2001, Peragallo et al. 2002, Kitchener et al. 2003, Resseguier et al. 2010).
Other factors influencing malaria risk include inaccurate pretravel advice from medical practitioners and the common problem of noncompliance with chemoprophylaxis across the full spectrum of travelers including tourists, backpackers, expatriate workers, military personnel, and VFRs (Boreham and Relf 1991, Behrens et al. 1998, Laver et al. 2001, Robinson et al. 2001, Landry et al. 2006, Jute and Toovey 2007, Pistone et al. 2007, Namikawa et al. 2008, Ropers et al. 2008, Piyaphanee et al. 2009, Resseguier et al. 2010). A survey of doctors in New Zealand found that prescriptions for malaria chemoprohylaxis were often inappropriate (Leggat et al. 1997), and recommendations were made to improve dissemination of up-to-date information to doctors.
Many cases of malaria are preventable with accurate pretravel advice, appropriate chemoprophylaxis, and mosquito avoidance. Information on the geographic distribution of malaria and appropriate chemoprophylaxis are available from reliable and regularly updated web-based resources, including the Centers for Disease Control and Prevention (Centers for Disease Control and Prevention 2012), Tropimed (Tropimed), and Travax (Shoreland). Local surveillance is important for providing clinicians with up-to-date information on vulnerable groups and common destinations for malaria acquisition, so that special attention on malaria prevention can be focused on travelers who are at highest risk. High-risk travelers should also be educated on the importance of mosquito-avoidance measures, urged to comply with chemoprophylaxis, and seek prompt diagnosis of fevers after visiting malaria-endemic areas.
Limitations of the study include incomplete data on some variables (as shown in Table 1) and very limited data on the use of chemoprophylaxis, immigrant status, and purpose and duration of travel. Therefore, it was not possible to calculate the incidence of malaria in New Zealand travelers. Improvements in the details collected for malaria notifications would provide valuable information on the incidence of imported malaria and high-risk groups. Some New Zealand travelers might also be diagnosed with malaria while overseas, and therefore not included in the surveillance data.
Conclusions
Malaria is an important cause of severe illness in returned travelers in New Zealand, especially from Papua New Guinea, Western Pacific, Africa, Sotheast Asia, and the Indian subcontinent. Common places of infection have changed over time and are likely to be a reflection of changing travel patterns of New Zealanders and the origins of visitors and immigrants. Local surveillance is therefore important for informing pretravel medical advice by identifying vulnerable groups and common destinations for malaria infection so that special attention on malaria prevention can be focused on travelers who are at highest risk. Ongoing surveillance is also essential for monitoring the evolving epidemiology of imported malaria over time.
Footnotes
Acknowledgments
This work was supported by funding from the New Zealand Foundation for Research, Science & Technology (contract C03X0801).
Author Disclosure Statement
No competing financial interests exist.