
Abstract
Infective endocarditis and hepatosplenic abscesses are rare manifestations of cat scratch disease (CSD), especially among immunocompetent adults. An otherwise healthy woman who presented with fever and abdominal pain was diagnosed with multiple abscesses in the spleen and the liver, as well as a mitral valve vegetation. PCR on spleen tissue was positive for Bartonella henselae. Prolonged treatment with doxycycline and gentamicin led to complete recovery. Review of the literature revealed 18 cases of hepatosplenic CSD in immunocompetent adults; the majority presented with fever of unknown origin and abdominal pain. In most cases the causative organism was B. henselae and the pathological findings were necrotizing granulomas, similar to the pathological features in classic CSD. Concomitant endocarditis was diagnosed in one case. Because Bartonella is one of the leading pathogens of culture-negative endocarditis, we raise the question of whether a comprehensive evaluation for endocarditis is needed in cases of systemic CSD.
Introduction
C
We describe the case of an immunocompetent adult who presented with fever, hepatosplenic abscesses, and a mitral valve vegetation secondary to B. henselae. Other cases of hepatosplenic CSD in immunocompetent adults are reviewed. The need to rule out endocardial involvement in cases of systemic CSD is discussed.
Case Report
A 50-year-old otherwise healthy woman presented to the emergency department with fever up to 39.4°C, and epigastric and left flank pain. Her illness began abruptly with rigors, vomiting, and malaise. She reported a flu-like illness 2 weeks earlier but denied having gastrointestinal, genitourinary, or respiratory complaints. Her medical history was unremarkable, and none of her family members or friends had been ill recently. She took no medications, did not smoke or use illicit drugs, and denied having direct contact with animals or any arthropod bites. However, she admitted to feeding stray cats.
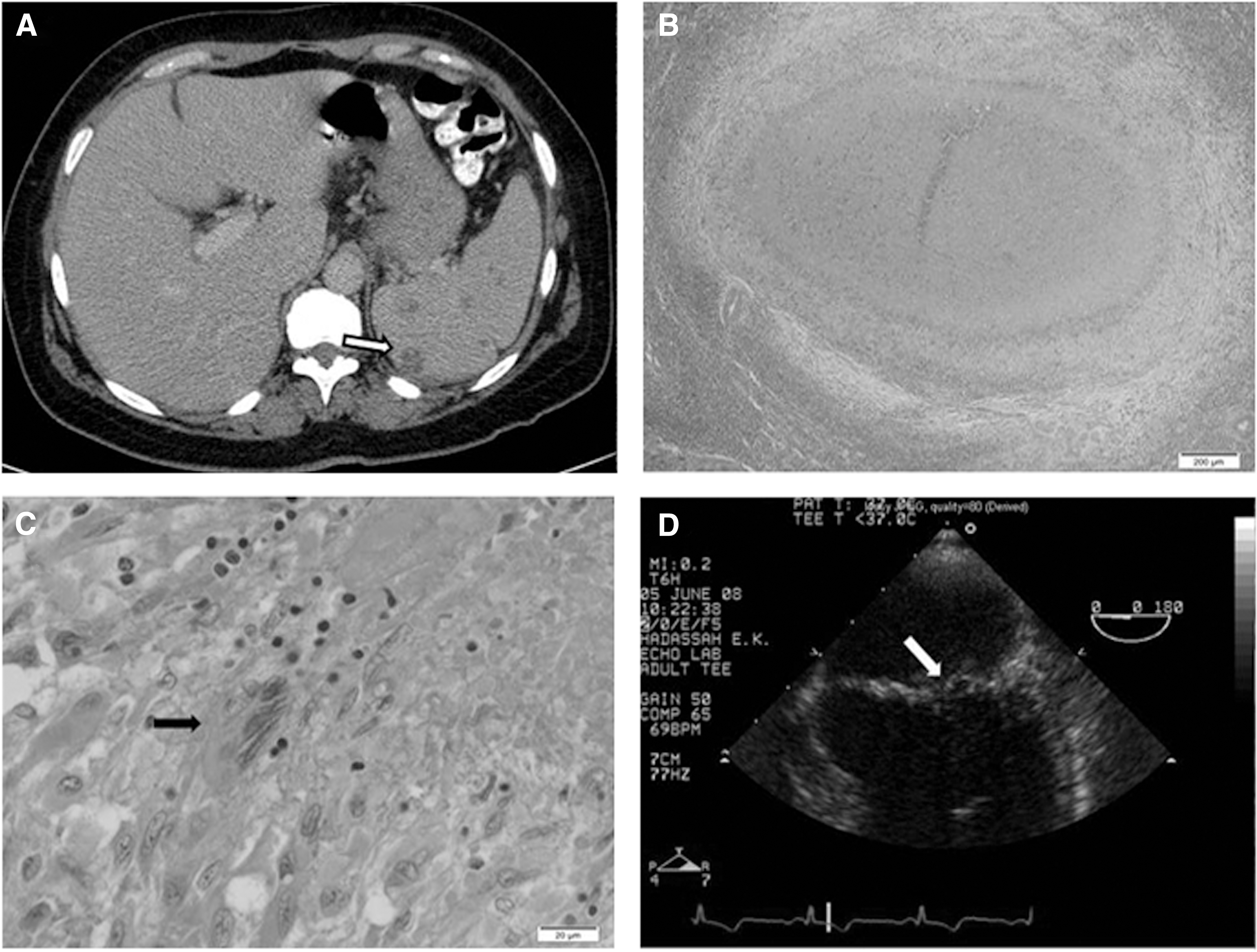
On admission, her blood pressure was 110/70 mmHg, her pulse was 80 beats per minute, her temperature 38.4°C, and her oxygen saturation 95% while breathing ambient air. Heart sounds were normal; there was no murmur. Mild tenderness was present in the upper and lower left abdomen; peritoneal signs were absent. No rash or lymphadenopathy was found; no signs of scratches or insect bites were evident. The remainder of the physical examination was unremarkable. Her white blood cell count was 12,400 cells/mm3 with 91.3% neutrophils; her hemoglobin level was 12.2 g/dL; the platelet count was 365,000/mm3; her coagulation studies were normal. Serum electrolytes and tests of kidney and liver function were unremarkable. A urinalysis was normal. An abdominal ultrasound on admission revealed an enlarged spleen (16.5 cm) with multiple hypoechoic lesions up to 1.5 cm in diameter, and a small amount of free fluid in the abdomen. An abdominal computed tomography (CT) scan with intravenous contrast revealed multiple hypodense round nonenhancing lesions in the spleen (up to 2 cm), and few in the liver (up to 0.5 cm) (Fig. 1a). An evaluation for splenic and liver abscesses was performed. Multiple blood cultures, including cultures for mycobacteria, were sterile. Serological tests for Brucella, Coxiella burnetti, Echinococcus granulosus, and Entamoeba histolytica were negative. A transthoracic echocardiogram revealed normal valves without vegetations. Using previously validated assay conditions (Giladi et al. 2001), an enzyme immunoassay (EIA) for Bartonella spp. was positive, with an immunoglobulin G (IgG) titer of 1:800 and negative IgM.
(
The patient was treated with a broad-spectrum antibiotic regimen that included ampicillin and gentamicin, and her fever and abdominal complaints resolved. A repeat CT scan performed 14 days after her admission showed, however, that her splenic and hepatic lesions remained unchanged. As the lesions in the spleen appeared bigger and better defined than those in the liver, a biopsy of her spleen was conducted. Several hours later she suffered from an intraabdominal hemorrhage originating from the spleen and an urgent splenectomy was performed.
Pathological examination of the spleen revealed superficial multiple white nodules (up to 1 cm). Microscopic examination revealed necrotizing granulomas with several multinucleated giant cells (Fig. 1B, C). Ziel–Nielsen, silver, and Gram stains were all negative. A Whartin–Starry stain was equivocal. Bacterial, fungal, and mycobacterial cultures from the spleen were negative. Amplification of 277 bases of the B. henselae heme-binding protein gene pap31 by standard PCR using the primer pair PAPn1 and PAPn2 as previously described (Rolain et al. 2003b) was positive. A transesophageal echocardiogram (TEE) revealed prolapse of the posterior leaflet of the mitral valve with two jets of mild regurgitation and a small mobile echogenic mass (2×4 mm) attached to it (Fig.1D). Thus, the patient had systemic CSD with probable mitral valve endocarditis. Treatment with intravenous gentamicin for 2 weeks and oral doxycycline for 6 weeks was initiated. On a follow-up TEE done 3 months after completion of antibiotic treatment, the mitral valve vegetation was no longer detectable.
Discussion
CSD is a relatively common and benign infection caused by the fastidious Gram-negative bacillus B. henselae, and, much less commonly, by Afipia felis or Bartonella clarridgeiae (Giladi et al. 1998, Kordick et al. 1997). Typically a disease of children and young adults (Zangwill et al. 1993), its telltale features are an erythematous, papular, or pustular skin lesion at the site of inoculation (usually from a cat scratch or a flea bite) and regional lymphadenopathy (Dolan et al. 1993). Approximately 5–24% of cases present with an atypical form (Carithers 1985, Brunetti et al. 2013), mainly Parinaud oculoglandular syndrome, as well as less common presentations, including neuroretinitis, encephalopathy, musculoskeletal manifestations, fever of unknown origin, visceral abscesses, or endocarditis.
Visceral manifestations of B. henselae infection appear in two forms. The first is the more common bacillary peliosis hepatis/splenitis (BP/BS) type, described primarily in immunocompromised patients (Dolan et al. 1993). In this form, the characteristic pathological findings are vascular proliferative lesions, similar to the cutaneous lesions of bacillary angiomatosis (BA) described in patients with advanced acquired immunodeficiency syndrome (AIDS). The second, less common, form of visceral B. henselae infection is the one diagnosed in our patient. Here the pathological hallmark is necrotizing granulomas that are indistinguishable from the pathological picture found in the lymph nodes of those suffering from classic CSD. This form has been described mainly in immunocompetent children; however, in some cases, clear T cell dysfunction has been demonstrated (Kahr et al. 2000). Only a handful of cases of visceral CSD in adults have been published, most of them in patients with various degrees of immunodeficiency (Liston et al. 1996).
Eighteen cases of hepatosplenic CSD in immunocompetent adults (ten of them in the English literature) have been reported and are summarized in Table 1 (Delahoussaye et al. 1990, Tappero et al. 1993, Bouchard et al. 1996, Okamoto et al. 2001, Zaccala et al. 2001, Gilad et al. 2003, Le Tallec et al. 2003, Rolain et al. 2003a, Durupt et al. 2004, Family-Pigne et al. 2006, van der Veer-Meerkerk et al. 2008, Renou et al. 2010, Zenone 2011). Review of the previous reports shows that the majority of the cases presented with fever of 1–8 weeks duration before patients sought medical attention. In most cases, the presenting symptoms included abdominal pain, constitutional symptoms, and weight loss, similar to the presentation of our patient. Peripheral lymphadenopathy, suggestive of classical CSD, was evident in one-third of cases (6/18). Lesions in the liver and or splenic compatible with abscesses were diagnosed by abdominal imaging, or after exploratory laparotomy as part of an evaluation of fever of unknown origin (FUO). In three cases, an unusual and rare clinical picture was evident and it included a combination of FUO, hepatic/splenic abscesses, and either Parinaud syndrome (Bouchard et al. 1996), vertebral osteomyelitis (Rolain et al. 2003a), or infective endocarditis (Family-Pigne et al. 2006), as in our patient. In all but three cases, the causative organism was identified as B. henselae. In five, a molecular diagnosis (PCR from spleen or liver) was positive for B. henselae, and in ten the diagnosis was based on a positive serology for B. henselae (that may have cross reactivity with other Bartonella species). In one case, B. quintana was identified with high certainty (positive EIA verified by western blot, and negative B. henselae serology) (Durupt et al. 2004). CSD caused by B. quintana was previously described in a pediatric case with hepatosplenic involvement (Laham et al. 2008). In the remaining two cases, a diagnosis of Bartonella infection without identification of the species was done based on histology and a positive Warthin–Starry stain (Delahoussaye et al. 1990) or by serology (Zaccala et al. 2001). In ten cases, a tissue sample was available for histopathological examination, and in all but one the characteristic picture of CSD was evident—necrotizing granulomas and lack of vascular proliferation. In all but two cases, an exposure to cats was documented, and in five cases (28%) a history of cat scratch was elicited.
Echo, echocardiogram; M, male; F, female; RUQ, right upper quadrant; LFT, liver function tests; WS, Warthin Starry stain; ND, not done; INH, Isoniazid; RIF, rifampin; US, ultrasound; MGC, multinucleated giant cells.
Antibiotic treatment was administered in all but three cases; the patient with endocarditis was treated for a prolonged period (Family-Pigne et al. 2006). Treatment was usually started before a diagnosis of bartonellosis was made. Thus, the antibiotic regimen was not necessarily directed against Bartonella. Clinical recovery and radiographic improvement or resolution (in the 12 cases in which follow-up imaging was done) was the rule. Clinical recovery was also achieved in the three cases in which no antibiotics were administered, and in one following splenectomy (Gilad et al. 2003). The combination of hepatosplenic CSD and endocarditis has been described once before, and the diagnosis was then based on positive serology for B. henselae (Family-Pigne et al. 2006). The diagnosis of B. henselae infection in our patient was confirmed with high certainty by a combination of methods—characteristic histopathological findings, positive serology, and a positive PCR specific for B. henselae from the spleen. Failure to visualize the bacteria directly in the splenic specimen is not unusual. In a series of cases of hepatosplenic bartonellosis, the chances of directly visualizing the bacteria were higher in immunocompromised patients compared to immunocompetent individuals (Perkocha et al. 1990), possibly due to the higher organism load in the absence of an effective immune response.
Our patient was exposed to cats, but did not recall being scratched. Lack of exposure to cats or other animals is not unusual. In a prior series, lack of exposure to any animal was documented in 5–7% of cases (Daniels et al. 1954, Murakami et al. 2002). Additional animals can serve as reservoirs for B. henselae, and the organism has been also isolated from several arthropod vectors (Mosbacher et al. 2011). In addition, there might be some other routes of transmission still not fully understood.
Bartonellae are a leading cause of culture-negative endocarditis. In a large series of definite culture-negative endocarditis, 348 patients were assessed using serology for a wide range of atypical pathogens, cultures, and PCR from valve specimens. In this series Bartonella spp. were second only to Coxiella burnetii infection, and accounted for 28% of the cases (Houpikian et al. 2005). Of those cases, 75% were identified as B. quintana and 24% as B. henselae. The case fatality rate has ranged from 7% (Houpikian et al. 2005) to 27% (Raoult et al. 1996). One of the reasons for the high mortality rates in older series was the delayed diagnosis and the need for cardiac surgery in up to 95% of cases (Fournier et al. 2001). Antibiotic treatment that included an aminoglycoside for at least 2 weeks was associated with a favorable outcome and a greater likelihood of a full recovery compared to patients treated with doxycycline alone (Raoult et al. 2003). The combination of early diagnosis and proper treatment might be the key for a successful outcome.
Similar to other cases of Bartonella endocarditis, our patient was infected by B. henselae, and the vegetation on the mitral valve was small (Family-Pigne et al. 2006, Gouriet et al. 2007). In fact, the diagnosis of endocarditis in our patient could easily have been missed. TEE was performed before the diagnosis of Bartonella infection was established because she presented with fever and splenic lesions suspicious of abscesses, an uncommon complication of infective endocarditis. In a recent publication by the French group that reported the majority of Bartonella endocarditis cases, the history of classic CSD was retrospectively elicited in a case in which Bartonella endocarditis was incidentally diagnosed on a valve that was removed during a valve replacement surgery (Gouriet et al. 2007). The authors hypothesized that, as an asymptomatic and hard-to-detect Bartonella bacteremia might appear in a nonnegligible number of patients with CSD, routine screening by echocardiography should be performed to rule out valvular lesions. Our case supports that approach, but larger studies are needed before echocardiography is routinely done for patients with CSD.
In summary, we described a previously healthy woman who suffered from combined hepatosplenic abscesses and mitral valve endocarditis caused by B. henselae that was diagnosed by serology, pathology, and PCR from an infected tissue. Full recovery followed 6 weeks of antibiotic treatment. We urge further research on the need for echocardiographic evaluation and for prolonged antibiotic treatment for cases of Bartonella infection in which signs of systemic seeding are apparent.
Footnotes
Acknowledgments
We would like to thank Prof. Theodore A. Stern, MD, from the Massachusetts General Hospital, Boston, for kindly reviewing the manuscript.
Author Disclosure Statement
No competing financial interests exist.