
Abstract
Tick-borne encephalitis (TBE) is a zoonotic disease, transmitted mainly by the bite of ticks. The TBE virus (TBEV) belongs to the family Flaviviridae, genus Flavivirus and is able to cause meningoencephalitis. For serological TBEV detection, the neutralization test (NT) is the most specific assay available. Different NT protocols are used in the laboratories, and until now the performance of these NTs has never been tested in an external quality assessment (EQA). In this EQA, we compared the results of eight European laboratories in detecting 17 samples (11 TBEV positive, five flavivirus cross reactive, and one negative sample) by NT. Furthermore, 14 of these EQA samples and 15 additional samples were tested in different commercial assays: 15 immunoglobulin G (IgG) enzyme-linked immunosorbent assays (ELISAs) and an immunofluorescence assay (IFA). Four laboratories showed a good NT EQA performance, whereas four laboratories had some sensitivity problems. Additionally, two of these laboratories showed a lack in specificity, misidentifying a dengue-positive sample as TBEV positive. The comparison of the commercial ELISAs revealed a high sensitivity in all assays, but as expected for IgG, the ELISAs showed a high degree of flavivirus cross reactivity. The assessment of Vienna Units in some of the ELISAs revealed deviations in the standards used by the different companies. Therefore, these standards should be revised. Generally, in this EQA, we found that reliable NT protocols are used in most of the laboratories, and the evaluation of the IgG ELISAs and the IFA showed a good agreement.
Introduction
T
At least one-third of the infected patients develop symptoms. The disease shows a biphasic course, beginning as an unspecific febrile infection. After an asymptomatic interval, 75% of the symptomatic patients develop a second phase, which is characterized by high fever and neurologic impairment. The patients show signs of meningitis, encephalitis, myelitis, or radiculitis (Kaiser 1999, Kollaritsch et al. 2011). After recovery, permanent central nervous system sequelae are commonly found, mainly in encephalitic patients. The severity of infection and lethality are age dependent (Kaiser 2012).
There is no specific treatment for TBE, but four different TBEV vaccines are available. Two of these vaccines are produced with strains of the European subtype (FSME-Immun® and Encepur®) and two with the Far Eastern subtype (TBE-Moscow and EnceVir®). All four show a very good safety profile and a seroconversion rate of 97–100%. Only a few cases of vaccination failure have been detected since introduction of the vaccines (Kollaritsch et al. 2011).
Because the symptoms of TBE are unspecific, the diagnosis relies on the laboratory analysis of TBEV. RNA is detectable in blood and cerebrospinal fluid (CSF) in the early stages of the disease. At the end of the asymptomatic phase and with the appearance of antibodies, the RNA becomes undetectable. Specific antibodies occur more slowly in CSF, but almost invariably become detectable within 10 days of onset of symptoms. With the beginning of the second phase, when the patients typically seek medical help due to the neurological symptoms, the diagnosis can only be made by serological assays (World Health Organization 2011).
There are different serological assays available. Most of the laboratories use enzyme-linked immunosorbent assays (ELISAs), some immunofluorescence assays (IFAs), and few hemagglutination inhibition assays. The neutralization test (NT), the most specific assay, is performed in special laboratories for confirmation or special questions, such as the immune status after several flavivirus vaccinations and/or infections.
A standard for the quantification of antibodies against TBEV was developed 1983 in Vienna (Hofmann et al. 1983) and has been used by different ELISA manufacturers since then. It consists of a standard serum with an arbitrary value of 1000 Vienna Units (VIEU). According to Holzmann et al., the VIEU correlate with the neutralization titer of the serum. VIEU/mL of ≥127 are considered positive (Holzmann et al. 1996). This correlation is seen as controversial because the ELISA measures neutralizing and non-neutralizing antibodies and this antibody correlation is not present in every person. Nevertheless, VIEU are measured in many laboratories, due to the fact that the NT is labor intensive and that another international standard is lacking.
The first company providing an ELISA with this standard was Immuno GmbH (Vienna, Austria). The production and marketing of the Vienna ELISA was taken over by Progen and IBL when Immuno ceased to trade. Today only these two companies state that they use the original standard. All other Vienna ELISAs available today use either the Progen standard (Mikrogen) or have developed their own standard on the basis of the Progen standard (Euroimmun, Test-Line, and Virotech) or on the basis of the IBL standard (Mast Diagnostica). The serological diagnosis of TBEV is difficult because nearly all serological assays also detect a certain amount of cross-reactive antibodies against other flaviviruses. Therefore, the diagnosis of the disease in patients with a history of flavivirus infections or vaccinations is quite challenging (Holzmann 2003).
The most specific assay is the NT, which detects the neutralizing antibodies directed against TBEV. Different protocols for these NTs are available. To determine the neutralization titer, it is either possible to assess the plaque reduction by a plaque reduction neutralization test (PRNT) or to perform a microneutralization assay, assessing the tissue culture infectious dose (TCID). Both titers demonstrate the specific neutralization capability of the serum against TBEV. The neutralization assays are not standardized, and all the laboratories use their own in-house method.
The external quality assessment (EQA) reported here was performed to compare the results of the different laboratories and to assess the quality of the NT protocols. Additionally, the performance of 15 commercial TBEV IgG ELISAs and an IgG IFA was analyzed.
Material and Methods
For the NT EQA, a panel of 17 samples was sent to 10 participating European laboratories. The panel consisted of 10 TBEV-positive sera (four highly, three medium, and three low positive), one monoclonal anti-TBEV antibody, and five sera positive for other flaviviruses (sera infected from patients infected with West Nile Virus [WNV] and dengue virus [DENV], and people vaccinated against Japanese encephalitis virus [JEV], and yellow fever virus [YFV]), plus one negative sample. The laboratories performed the NT according to their in-house protocols, and results were received from eight of the 10 participating laboratories. One of these laboratories (no. 7) sent the results of three different NT protocols.
For the evaluation of the commercial IgG ELISAs and the IFA, 29 samples were tested: 14 EQA samples and 15 additional samples. The panel consisted of 20 TBEV-positive samples (13 highly, three medium, and four low positive, including sequential serum samples from two TBE vaccinees and two TBEV-infected persons), five sera positive for other flaviviruses (WNV, JEV, DENV, and YFV), and four negative samples. Both vaccinees had been vaccinated against TBE years ago but did not develop a detectable TBEV NT titer. Shortly before the new TBE vaccination, they were also vaccinated against YFV.
The samples were tested in duplicate in 15 commercial IgG ELISAs by 14 different companies according to the manufacturers' instructions (Table 1). Standard curves of the different ELISAs were generated with the Sigma Plot standard curve macro, using the four-parameter logistic equation function. Nine ELISAs measured in-house units or positivity index, whereas six ELISAs measured VIEU. The in-house unit results of the TestLine ELISA can also be calculated to VIEU.
TBE, tick-borne encephalitis; IgG, immunoglobulin G; ELISAs, enzyme-linked immunosorbent assays; DU, DRG units; VIEU, Vienna Units; U, units; NTU, NovaTec units; VE, Virotech units.
Additionally, a serial dilution of one sample was analyzed for VIEU/mL in four different assays. This plasma sample of a TBE vaccinee was recalcified and substituted with thrombin to remove the fibrinogen (Castro et al. 2002, with modifications). It will be available as a characterized standard to achieve comparability for the different assays.
The anti-flavivirus IFA (Flavivirus Profile 2, EUROIMMUN AG, Lübeck, Germany) consists of 10 reaction fields with four biochips each. The biochips are covered with cells infected with one of the eight flaviviruses. The serum dilution is incubated on two reaction fields, one reaction field with four biochips for all of the DENV serotypes and one reaction field with four biochips covered with TBEV-, JEV-, YFV-, or WNV-infected cells, respectively. The test was performed and the titer for the different flaviviruses was calculated according to the manufacturer's instructions.
Results
The results of the NT EQA showed a good performance for four laboratories (Table 2). Four other laboratories had some sensitivity problems. Three of these (nos. 2, 9, and 3) misinterpreted one or two low-titer anti-TBEV–positive samples as negative, whereas laboratory no. 5 misinterpreted one highly positive and all three low positive sera as borderline. Two laboratories (nos. 9 and 3) additionally showed specificity problems. Both categorized one of the anti-DENV samples as positive.
Positive results are displayed in bold, borderline results in italic and light grey, and negative results on a grey background. Laboratory no. 7 delivered results with three different NT protocols (a–c).
NT, neutralization test; TBEV, tick-borne encephalitis virus; EQA, external quality assessment; YFV, yellow fever virus; WNV, West Nile virus; DENV, dengue virus; JEV, Japanese encephalitis virus; mAb, monoclonal antibody; NA, not available.
The comparison of nine different protocols of the participants (Table 3) showed the wide variety in the neutralization assays field. Only two laboratories performed an “old-style” NT with plaque reduction on six- or 24-well plates, whereas the majority used 96-well plates and assessed the cytopathic effect (CPE) or performed an IFA or ELISA. Interestingly, in two protocols, the serum was not inactivated before testing. The mode of determination of the titer and the cutoffs also varied from laboratory to laboratory.
EQA, external quality assessment; NT, virus neutralization titer; MEM, minimum essential medium; DMEM, Dulbecco modified Eagle medium; TCID, tissue culture infective dose; FFD, focus-forming dose; pfu, plaque-forming units; CPE, cytopathic effect; TBE, tick-borne encephalitis; ELISA, enzyme-linked immunosorbent assay; ED, effective dose; RT, room temperature; CMC, carboxymethyl cellulosis.
In five protocols the titer was determined only from the serum dilution, regardless of the amount of virus added, and in four protocols the titer was determined as the serum dilution plus virus dilution. But also generally, even when recalculated to one dilution method, the titers varied widely among all of the laboratories, depending on the specific protocol used.
The second part of our study was focused on the performance of different commercial anti-TBEV immunoglobulin G (IgG) ELISAs and an anti-TBEV IgG IFA. Nine ELISAs assessed in-house units or a positivity index and seven ELISAs measured VIEU/mL. It was remarkable that the VIEU cutoffs vary between the different assays (Table 4A). The overall performance of all the ELISAs was good. Nearly all ELISAs detected all EQA anti-TBEV–positive samples as positive, and only one low positive sample was categorized as borderline in the Novatec ELISA (Table 4A). All negative samples were negative in all ELISAs, but as expected the situation with sera containing anti-flavivirus antibodies turned out to be more complicated (Table 4B). Both samples of DENV patients were detected as positive by all of the ELISAs, and the anti-WNV sample was detected as borderline by one ELISA and as positive by all the others. The anti-JEV- and the anti-YFV-positive sample were categorized as negative in all ELISAs.
A. Cutoffs of anti-TBEV IgG ELISAs and results with anti-TBEV–positive samples.
B. Results with flavivirus cross-reactive and negative samples and results of sequential serum samples from two vaccinees who had been preimmunized against YFV.
C. Results of sequential serum samples of two TBE patients and the TBE standard serum (Std).
Negative results are displayed in dark grey and borderline results in italic and light grey. Standard curves were calculated with Sigma Plot 4 parameter analysis (with dynamic curve fit).
TBEV, tick-borne tick encephalitis virus; IgG, immunoglobulin G; ELISA, enzyme-linked immunosorbent assay; NT, neturalization test; YFV, yellow fever virus; WNV, West Nile virus; JEV, Japanese encephalitis virus; DENV, dengue virus; dpv, days postvaccination.
Additionally, sequential samples from two TBE vaccinees and two TBEV-infected patients were analyzed (Table 4B, C). The prevaccination serum from both vaccinees showed varying results between the assays. Whereas 13 (vaccinee 1) and 14 assays (vaccinee 2) detected the sera as positive, the other assays showed a negative or borderline result. In the subsequent sera, which were also NT positive, all ELISAs reacted positive. Vaccinee no. 2 showed slightly lower NT and also ELISA titers than vaccinee no. 1, also 60 days postvaccination. The sequential samples of the TBEV-infected patients showed very high titers in all ELISAs.
Selected exemplary samples were assessed with all the ELISAs measuring VIEU and the results were compared. Figure 1 shows the marked differences between the different assays. The values achieved using the IBL test are nearly twice as high as the ones achieved with the Progen assay, showing main deviation of the standards. The values of the other assays either cluster with the Progen assay (Mikrogen, Euroimmun and Virotech) or lie in between (TestLine and Mast Diagnostica).

Comparison of neutralization test (NT) values and Vienna units (VIEU)/mL of exemplary serum samples in seven different enzyme-linked immunosorbent assays (ELISAs).
Serum #32 was also detected as very highly positive by all ELISAs. To demonstrate the possibility of using this serum as a standard serum, serial dilutions of this serum were made and analyzed together with a serial dilution of the Progen standard samples using four different ELISA assays. The Progen standards were used for all of the VIEU/mL calculations for all four assays (Fig. 2). The results were comparable in higher dilutions, but varied for the lower dilutions with very high VIEU/mL. For the very high VIEU/mL (>1000 VIEU/mL), the results of the Virotech and Euroimmun assay were approximately 25% higher than those of the other assays.
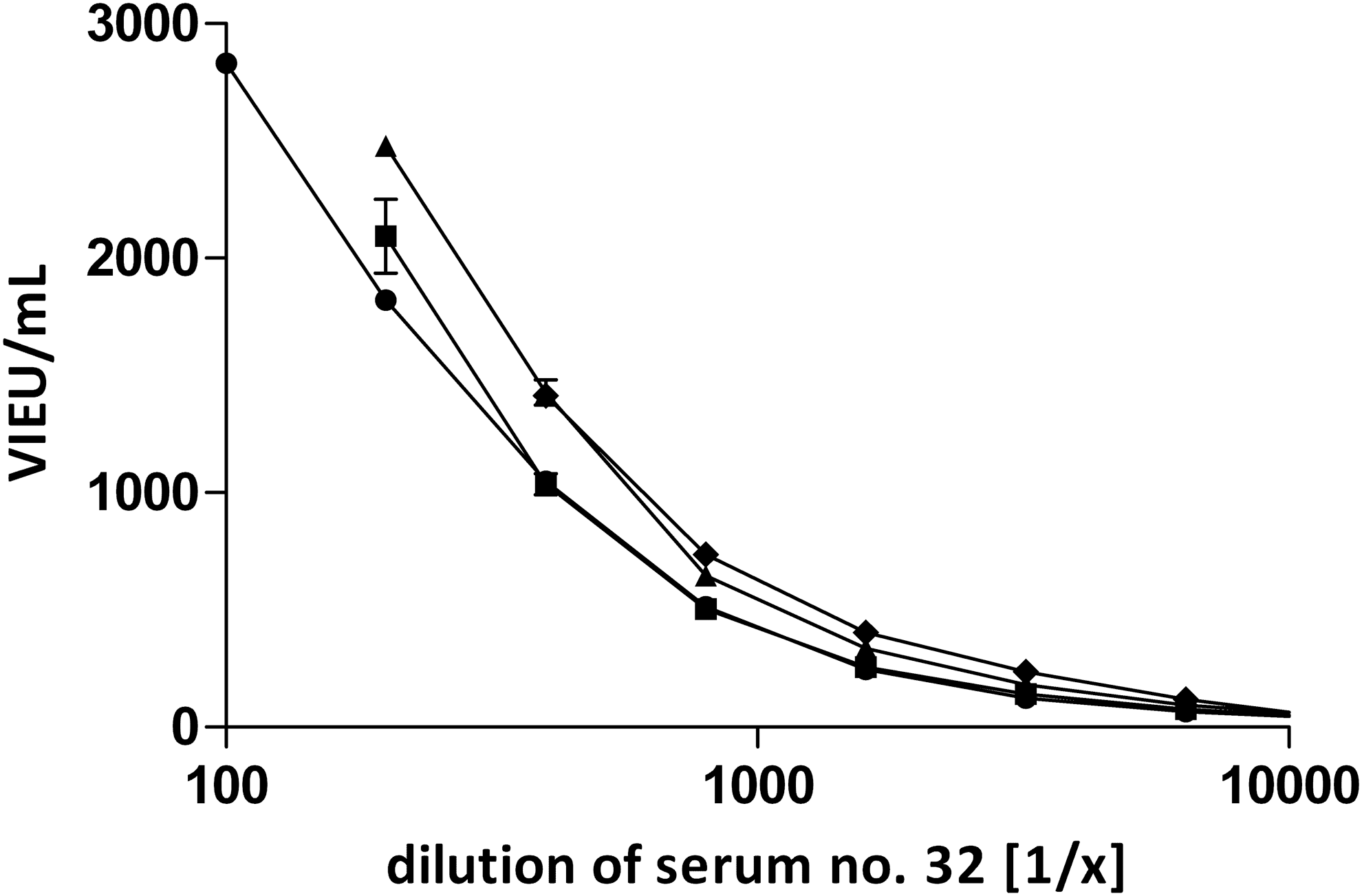
Vienna units (VIEU)/mL analysis of standard serum dilutions on different tick-borne encephalitis virus (TBEV) enzyme-linked immunosorbent assays (ELISA). For the calculation of the standard curve, a serial dilution of the Progen standard was assessed in all assays. The VIEU/mL calculation was performed with Sigma Plot 4 parameter analysis (with dynamic curve fit). (▲) Virotech assay; (□) IBL assay; (●) Virion/Serion assay; (◆) Euroimmun assay. The 1:100 serum dilutions for IBL and Virotech assay were >3000 VIEU/mL.
Moreover, another commercial assay, the anti-flavivirus mosaic IFA from Euroimmun, was analyzed with the same study samples. On this IFA one sample is incubated simultaneously with eight different flaviviruses (Table 5A). For most of the anti-TBEV–positive samples, the titer against the TBEV substrate was higher than the titer against the other flavivirus substrates. Only one sample (#14) showed a titer of 1:100 against TBEV and against YFV. Eight of the 10 anti-TBEV–positive samples showed also some reactivity against some other flaviviruses, but the titer was lower than that against TBEV. Only one medium-titer (#2) and one low-titer serum (#1) showed no sign of cross-reactivity in the IFA. The other flavivirus cross-reactive samples were also analyzed on the IFA. In the anti-YFV, -WNV, -JEV, and in one anti-DENV sample, the antibodies were detected correctly as directed against the respective flavivirus. Only one sample (anti-DENV positive) reacted very strongly with all the flavivirus substrates, and a differentiation was not possible. The sequential samples of the two TBE vaccinees showed an interesting pattern. Sample #18 was positive with a titer of 1:10 for several flaviviruses. Thirty days after TBE vaccination, the subject reacted against all tested flaviviruses, but the strongest response was directed against TBEV. Sample #20 showed an antibody response against different flaviviruses, but the highest titer was against YFV. Thirty days after TBE vaccination, a reaction against all flaviviruses (except for DENV-4) was detected, with the strongest response against TBEV, YFV, and DENV-2/-3. Thirty days later, the highest titer was directed only against YFV and TBEV. The sequential samples after TBEV infection and the standard sample showed very strong responses using the IFA. In all samples the anti-TBEV titer was the highest compared with the other flavivirus titers measured.
Highest antibody titer for each serum is in bold; negative results and lower antibody titer are in light grey.
IgG, immunoglobulin G; IFA, immunofluorescence assay; TBEV, tick-borne encephalitis virus; YFV, yellow fever virus; WNV, West Nile virus; DENV, dengue virus; JEV, Japanese encephalitis virus.
Discussion
Our study consisted of two parts: The EQA for TBEV NTs and the evaluation of 15 anti-TBEV IgG ELISAs and an anti-TBEV IgG IFA. In the TBEV NT EQA sensitivity, problems were discovered in four of the laboratories, but in most cases only very weakly positive samples were detected as negative. For the everyday diagnosis, these sensitivity problems are of minor relevance, whereas the specificity problems should be taken seriously, especially because the NT is often seen as the gold standard (Holzmann 2003) and many people are not aware that specificity problems may occur in NTs.
The comparison of the NT protocols showed major differences and the possible varying of NT protocols in general. But when comparing the NT protocols, we could not identify a single factor that could be determined to predict the performance of the assay. For example, the two protocols (Table 2, no. 3 and no. 9) showing a specificity problem by detecting an anti-DENV–positive sample as positive had very diverse reaction conditions. While no. 3 was a protocol measuring the CPE on a 96-well plate, protocol no. 9 measured the plaque reduction on six-well plates. Both assays used different cell lines, viruses, and serum/virus incubation conditions.
Two NT protocols were performed without prior serum inactivation at 56°C. It is recommended the inactivation be performed before testing, because this eliminates other possible pathogens and the complement system and therefore guarantees that only the neutralizing activity of the antibodies without the influence of the complement system is measured (Roehrig et al. 2008, Thomas et al. 2009). However, when skipping this procedure, the titers are higher in the presence of complement (Thomas et al. 2009), and the results more resemble the neutralization reaction expected in the human body. Our results show that two of the six protocols showing the best sensitivity and specificity did not perform the inactivation step before. One reason for the high sensitivity without inactivation can be that some antibodies might be destroyed by the heat of the inactivation step. But it could also be that the complement, which is still intact without inactivation, increases the neutralization of the virus, resulting in higher neutralization titers and therefore better sensitivity (Linscott et al. 1969, Mozdzanowska et al. 2006, Mehlhop et al. 2009).
Another main difference was how titers were calculated. Some laboratories only used the serum dilution, whereas others included serum and virus dilution in the calculation of the titer. The second method is the most definite way because it gives the serum dilution present during the critical step of the protocol, the incubation period of serum and virus. For other viruses, the usage is not consistent between the laboratories performing NTs; therefore, it is recommended to always report the calculation method of the final titer together with the NT results (Roehrig et al. 2008).
The results of the different protocols varied strongly, and this fact is important to consider in case NT titers should be compared between different laboratories using different NT protocols. In case a comparison is important, a standardized protocol should be used in both laboratories.
The evaluation of the commercial serological methods showed generally good sensitivity and specificity for all assays. As expected, some cross-reactivity was detected with samples positive for other flaviviruses. The results differed depending on whether the samples were samples from flavivirus vaccinees or patients. A higher proportion of ELISAs was able to discriminate antibodies against TBEV from cross-reactive antibodies after YFV or JEV vaccination than after DEN or WNV infection. The reason for this might be the generally higher titer after flavivirus infection than after vaccination. In consequence, the absolute amount of cross-reactive antibodies is also higher and is therefore detected by the ELISAs.
The two vaccinees were prevaccinated against TBE and YF, but in the first serum both were TBEV NT-negative and reacted negative or borderline in one-fourth of the TBEV ELISAs. Interestingly, the ELISAs by DRG, Technoclone, Vidia, and Virotech (Vienna) detected these prevaccination sera as well as the WNV-positive serum as borderline or negative, illustrating their higher cutoff values and better specificity with no decrease in sensitivity. But these multiple flavivirus antibody-positive sera show the difficulty of exact diagnosis in cases of vaccination against or exposure to different flaviviruses (Holzmann et al. 1996). In this case, no reliable statement regarding the immune reaction against the different vaccines can be made by ELISA.
The IFA offers a good alternative method in case of questionable or borderline results in ELISA. The main advantage is the simultaneous measurement of eight different flaviviruses. This provides the possibility of directly comparing the fluorescence intensity for each flavivirus and finding the one against which the strongest antibody response is directed. This kind of differentiation is not that easily possible with ELISA. But the evaluation of the fluorescence intensity requires ample experience with the technique and, in the case of multiple flavivirus exposure, the results are also difficult to interpret.
Our study showed differences in results of the ELISAs using Vienna standards, even though the IBL and Progen standards are based on the same original standard. For the low-positive sera, the results with the IBL assay were nearly twice as high as the results of the Progen assay, suggesting that the standards changed over time. Unfortunately, it was not possible to obtain the information regarding which standard still corresponds to the original standard produced in Vienna because both companies state that they never made major changes in the standard preparation.
Furthermore, it is remarkable that the cutoffs of the assays using VIEU vary. These assays measuring VIEU all refer to the Vienna standard, which means that the results as well as the cutoffs should be comparable. The original cutoff of the Vienna Units was 50 VIEU/mL (Hofmann et al. 1983). Later all samples with ≥127 VIEU/mL were rated as positive with protective immunity (Holzmann et al. 1996, Kiessig et al. 1993), and many ELISA companies rely on this cutoff. But there are also laboratories using higher cutoffs (Kunz 2003, Hofmann 2005).
In view of all these differences between the companies, it would be advisable for the companies to revise their VIEU to standardize the assays. To improve the comparability of the different diagnostic assays for TBEV, we extensively analyzed serum #32. Because we have a larger volume of this serum available, we could provide aliquots of this material to interested laboratories as standard preparation (niedrigm@rki.de). This serum is highly positive, can be further diluted, and showed good results even in higher dilutions in the different assays.
Footnotes
Acknowledgment
We would like to thank Petra Kreher for excellent technical assistance and Ursula Erikli and Axel Ronald Schulz for copyediting. This work was supported financially in part by funds from the Robert Koch-Institute for TBE reference center activities and by the ECDC for the ENIVD Collaborative Laboratory Response Network (ENIVD-CLRN) under the contract no. ECDC/2008/011.
Author Disclosure Statement
The position of Nadine Litzba was partly funded by EUROIMMUN AG, Lübeck, Germany.