
Abstract
During the summer–autumn of 2011, a human outbreak of West Nile virus (WNV) infection occurred in southern Greece, following the first outbreak during 2010 in northern Greece. An investigation was performed to analyze laboratory diagnosis, geographic distribution, and clinical features of WNV cases in southern Greece. Serum and cerebrospinal fluid (CSF) specimens from all patients seeking laboratory diagnosis for suspected WNV infection were tested for the presence of specific WNV immunoglobulin M (IgM) and IgG antibodies. Detection of WNV RNA in CSF and whole blood samples was accomplished by real-time PCR. During August–October of 2011, 31 confirmed or probable cases of WNV infection were identified. In 25 of them, individuals experienced severe neurological manifestations and were classified as WNV neuroinvasive disease cases. Risk factors such as advanced age, hypertension, and diabetes mellitus were identified in most cases with neurological complications. As many as 25 of the WNV cases occurred in the broader region of Athens; the majority of them (17 cases) were identified in municipalities of Eastern Attica, located almost 40 km from the metropolitan area of Athens and 500 km from Central Macedonia, where the 2010 WNV outbreak occurred. The spread of the virus in a newly affected area of the country suggests that WNV has been established in Greece and disease transmission will be continued in the future.
Introduction
W
Since its first isolation in the West Nile district of Uganda in 1937 (Smithburn et al. 1940), a geographic expansion and westward spread of the virus has occurred during the last 20 years (Gubler 2007). Except for the United States, where the virus, after its first identification in 1999 (Nash et al. 2001) extended its distribution and became endemic within the following 10 years (Hayes and Gubler 2006), several sporadic cases and a few WNV outbreaks have been reported in Europe and the Mediterranean basin (Murgue et al. 2002, Gubler 2007, Calistri et al. 2010, Magurano 2012).
In Greece, the first outbreak of WNV infection was reported in the summer of 2010. Overall, 262 probable and confirmed cases of WNV infection were notified, mainly in Central Macedonia, northern Greece. Among them, 197 were neuroinvasive cases and 33 had a fatal outcome (Papa et al. 2010a). The virus re-emerged in July of 2011, and a WNV infection outbreak has been ongoing in regions of Greece that had already been affected in 2010, but also in southern Greece, which had never reported human cases before (Danis et al. 2011). The aim of the present study was to determine the laboratory, epidemiological, and clinical characteristics of WNV infection cases identified during 2011 outbreak in Southern Greece.
Materials and Methods
Clinical specimens
Serum, whole blood, and/or cerebrospinal fluid (CSF) specimens were collected from all patients originating from southern Greece and considered “suspected” for WNV infection during 2011. Patients were presented with febrile illness and/or neurological manifestations ranging from headache to aseptic meningitis and/or encephalitis. For collecting and sending a sample for WNV infection investigation, a high index of suspicion was maintained for elderly patients in whom the majority of WNV-associated cases of central nervous system infection occurred. Serum and CSF specimens were tested for the presence of specific WNV immunoglobulin M (IgM) and IgG antibodies, whereas whole blood and CSF samples were used for detection of WNV RNA.
Case definition
Confirmed and probable WNV cases were defined taking into account a slightly modified 2008 European Union case definition that had also been used in the 2010 WNV infection outbreak in Greece (Papa et al. 2010a). A confirmed case was defined as a patient meeting any of the clinical criteria (e.g., encephalitis, meningitis, fever ≥38.5°C without specific diagnosis) and at least one of the following laboratory criteria: (1) Detection of WNV RNA in whole blood and/or CSF; (2) presence of WNV IgM antibodies in CSF with or without WNV IgG antibodies; (3) detection of increasing levels of IgM and IgG antibodies against WNV in consecutive serum specimens. A case was considered probable if the patient met the above clinical criteria and WNV IgM antibodies, with or without IgG antibodies, were detected in patient's serum specimen. Confirmed and probable cases were notified to the Hellenic Centre for Disease Control and Prevention (HCDCP).
Case laboratory investigation
WNV IgG and IgM enzyme-linked immunosorbent assays (ELISA)
IgG and IgM antibodies against WNV were detected using commercially available WNV IgG DxSelect and IgM capture DxSelect ELISA kits (Focus Diagnostics Inc, Cypress, CA), respectively, approved by the Food and Drug Administration. Patient sera and CSF samples were diluted 1:101 and 1:2, respectively, in sample diluent (Prince et al. 2004). Both ELISAs were performed according to the manufacturer's instructions.
Tick-borne encephalitis virus (TBEV) and dengue virus (DENV) antibodies detection
Specimens found positive for WNV antibodies during the first month (August) of the 2011 WNV outbreak were also tested for specific antibodies against TBEV (TBE/FSME IgG and TBE/FSME IgM ELISA kits; IBL International Gmbh, Hamburg, Germany) and DENV (DENV IgG Dx Select and DENV IgM Capture Dx Select ELISA kits; Focus Diagnostics Inc., Cypress, CA) to exclude possible interference of these viruses with the WNV assays.
Reverse transcriptase real-time PCR for WNV RNA detection
Total RNA was isolated with a High Pure RNA isolation kit (Roche Diagnostics GmbH, Mannheim, Germany) according to the manufacturer's instructions. Using the Transcriptor First Strand cDNA Synthesis Kit (Roche Diagnostics), 3.5 μL of RNA sample was reverse transcribed into single-stranded complementary DNA (cDNA) in a final volume of 20 μL, according to the manufacturer's guidelines. Aliquots of 5 μL of cDNA were used in a commercial real-time PCR (LightMix® Kit West Nile Virus, TIBMolbiol, Germany) performed in a LightCycler® 2.0 Instrument to detect the presence of WNV genome. A 111-bp fragment of the NS5 gene from the WNV genome was amplified with specific primers. The resulting PCR fragment was analyzed with hybridization probes labeled with LightCycler® Red 640. The PCR reaction was monitored by an additional PCR product of 278 bp, formed from the internal control (IC).
Blood donations screening for WNV RNA
According to the National Surveillance Plan, during the 2011 WNV outbreak period, nucleic acid amplification technology (NAT) screening was performed for blood donations that originated from regions where human cases of WNV infection had been notified. Blood donations were screened for WNV RNA using the WNV Transcription-Mediated Amplification (TMA) system (PROCLEIX WNV assay, Chiron, Novartis Diagnostics, Emeryville, CA) performed on individual-donation (ID) NAT. Donors identified as WNV positive were offered enrollment into a follow-up study consisting of sampling at 2-week interval and further testing for the development of WNV-specific IgM and IgG antibodies, as described above.
Results
Between August and October of 2011, 31 confirmed or probable cases of WNV infection were identified and reported to the HCDCP from 202 (15.3%) patients who presented with symptoms and signs compatible to WNV infection. In 25 (80.6%) of these cases, the patients experienced severe neurological manifestations and were classified as West Nile neuroinvasive disease (WNND) cases, while the remaining six (19.4%) cases were characterized as WNF cases.
Laboratory and clinical characteristics of WNND cases
Table 1 shows characteristics of the patients with WNND. Twenty-one of the 25 WNND cases (C1–C21) were considered as confirmed, whereas the remaining four (C22–C25) as probable. In detail, 14 WNND cases (C1–C14) were confirmed because the relevant clinical criteria were met and only WNV IgM antibodies were detected in CSF specimens. Regarding the remaining seven WNND confirmed cases, three (C15–C17) met the relevant clinical criteria, and WNV IgM and IgG antibodies were detected in both serum and CSF samples, whereas four (C18–C21) met the relevant clinical criteria but only serum samples were provided and high titers of WNV IgM and IgG antibodies were detected. Cases 22–25 were considered probable because the patients met the clinical criteria and only WNV IgM antibodies were detected in serum samples. The median index of IgM and IgG antibodies in sera from the 25 WNND cases was 4.26 (range 3.25–6.58) and 1.09 (range 0.27–3.53), whereas the corresponding index values in CSF specimens were 5.16 (range 3.48–6.57) and 0.53 (range 0.04–2.11), respectively.
C22–C25 were considered as probable cases.
M, male; F, female; NM, not mentioned; ND not done.
Clinical characteristics of the 25 WNND cases are shown in Table 1; 13 (52%) presented with meningitis, seven (28%) with meningoencephalitis, four (16%) with encephalitis, and one (4%) with acute flaccid paralysis and encephalitis. These illnesses were characterized by acute onset of fever with stiff neck, altered mental status (confusion, disorientation), seizures, limb weakness, abnormal CSF (raised number of lymphocytes and protein levels, and normal to slightly decreased glucose levels), and/or abnormal neuroimaging compatible with clinical presentation of meningitis and/or encephalitis. All patients with neurological clinical picture were hospitalized, and 11 (44%) were admitted to an intensive care unit (ICU), whereas seven (28%) who had several underlying conditions had a fatal outcome.
Demographic data and underlying diseases of WNND cases
The median age of WNND cases was 66 years, ranging from 25 to 86 years, whereas that of WNF cases was 52 years, ranging from 27 to 78 years. The incidence of WNND was higher among males because the male-to-female ratio was 2.6:1 (Table 1). The review of the patients' reporting forms regarding the underlying chronic medical conditions as potential risk factors for severe disease revealed that 15 of the 25 WNND cases had at least one underlying chronic disease (Table 1). The most common chronic diseases were hypertension (n=8) and diabetes mellitus (n=7), followed by coronary artery disease (n=2) and chronic alcohol abuse (n=2). Cerebrovascular disease, chronic obstructive pulmonary disease, kidney transplantation, and thyroid cancer (thymoma) were found in one case each (Fig. 1).
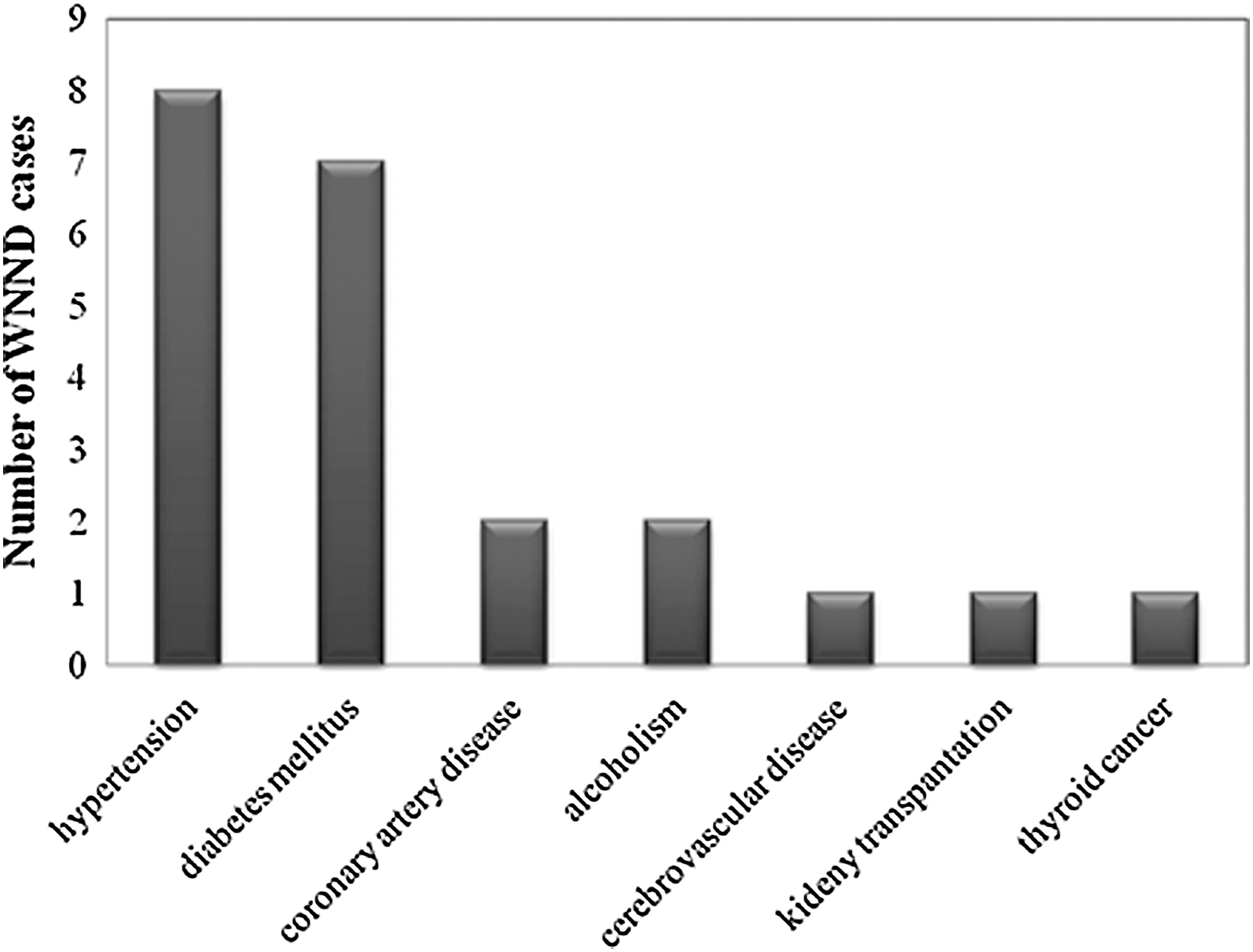
Recording of underlying chronic diseases/conditions among West Nile neuroinvasive disease (WNND) cases.
Laboratory and clinical characteristics of WNF cases
Demographic and laboratory characteristics of the nonneuroinvasive cases of WNV infection seeking medical attention (C26–C29) are presented in Table 2. All of them were considered as confirmed because two of the patients met the relevant clinical criteria and WNV IgM and IgG antibodies were detected in both sera and CSF specimens, whereas the remaining two patients met the relevant clinical criteria and were provided only with sera with high titers of WNV IgM and IgG antibodies. The median index of IgM and IgG serum antibodies was 6.28 (range 3.04–6.51) and 1.93 (range 1.71–3.68), respectively. Regarding the specific symptoms of these patients, sudden onset of fever was reported by all of them (usually >39°C), followed by headache, myalgias, arthralgias, fine maculopapular or morbilliform rash on the chest, back, and upper extremities, and gastrointestinal symptoms, including anorexia, nausea, and vomiting. All of the patients with WNF (C26–C29) were hospitalized, but none were in an ICU (Table 2).
Blood donors.
M, male; F, female; ND, not done.
All 25 WNND cases and the four hospitalized WNF cases tested with real-time PCR were negative for the presence of the WNV RNA genome in either whole blood or CSF. All WNV-positive specimens were found negative for TBEV IgG and IgM antibodies. Low cross-reactivity was seen with DENV in four cases. These cases gave negative DENV IgM results. DENV IgG index titers ranged from 1.08 to 1.25; they were considerably lower in comparison with the high WNV IgG titers (ranging from 2.32 to 3.53). According to the reporting forms' data, none of the patients had been vaccinated for yellow fever.
Laboratory and clinical characteristics of cases found positive in blood donations screening for WNV RNA genome
Serum specimens from six WNV-positive blood donations were received and tested for the presence of WNV IgM and IgG antibodies. The first sample from each donor was from the day of blood donation, whereas the second sample was submitted at least 2 weeks later. Testing of paired sera from acute and convalescent phases led to the identification of WNV IgG and IgM seroconversion only in two paired serum specimens (C30, C31; Table 2). This was not the case in the other serum pairs, where WNV IgG and IgM reactivity was not observed after serological testing of the relevant samples. All blood donors whose samples were collected and tested stated that they felt well at the time of donation. However, the two patients with WNV seroconversion later reported mild symptoms, compatible with WNV infection, such as body aches, drowsiness or fatigue, and muscle or general weakness.
Geographic distribution of WNV infection cases
Figure 2 shows the geographic distribution of WNV infection cases during the 2011 outbreak in southern Greece. According to patients' demographic data, 25 of the WNV cases occurred in the prefecture of Attica, in the broader geographic region of Athens. The majority of them (17 cases) were identified in the municipalities of eastern Attica, which are located almost 40 km from the metropolitan area of Athens and 500 km from Central Macedonia, where the 2010 WNV outbreak was localized. More specifically, these cases were reported from the municipalities of Marathon (10 cases), Artemis (3 cases), Oropos (1 case), Rafina (1 case), Spata (1 case), and Drossia (1 case). Eight additional cases were reported from the rest of the prefecture of Attica: Megara (2 cases), Melissia (1 case), Vrilissia (1 case), Kamatero (1 case), Acharnes (1 case), Piraeus (1 case), and Elefsina (1 case). Apart from Attica, five cases were reported in the prefecture of Viotia (4 cases in the city of Thebes and 1 case in Tanagra) and one case in the island of Andros (Fig. 2).
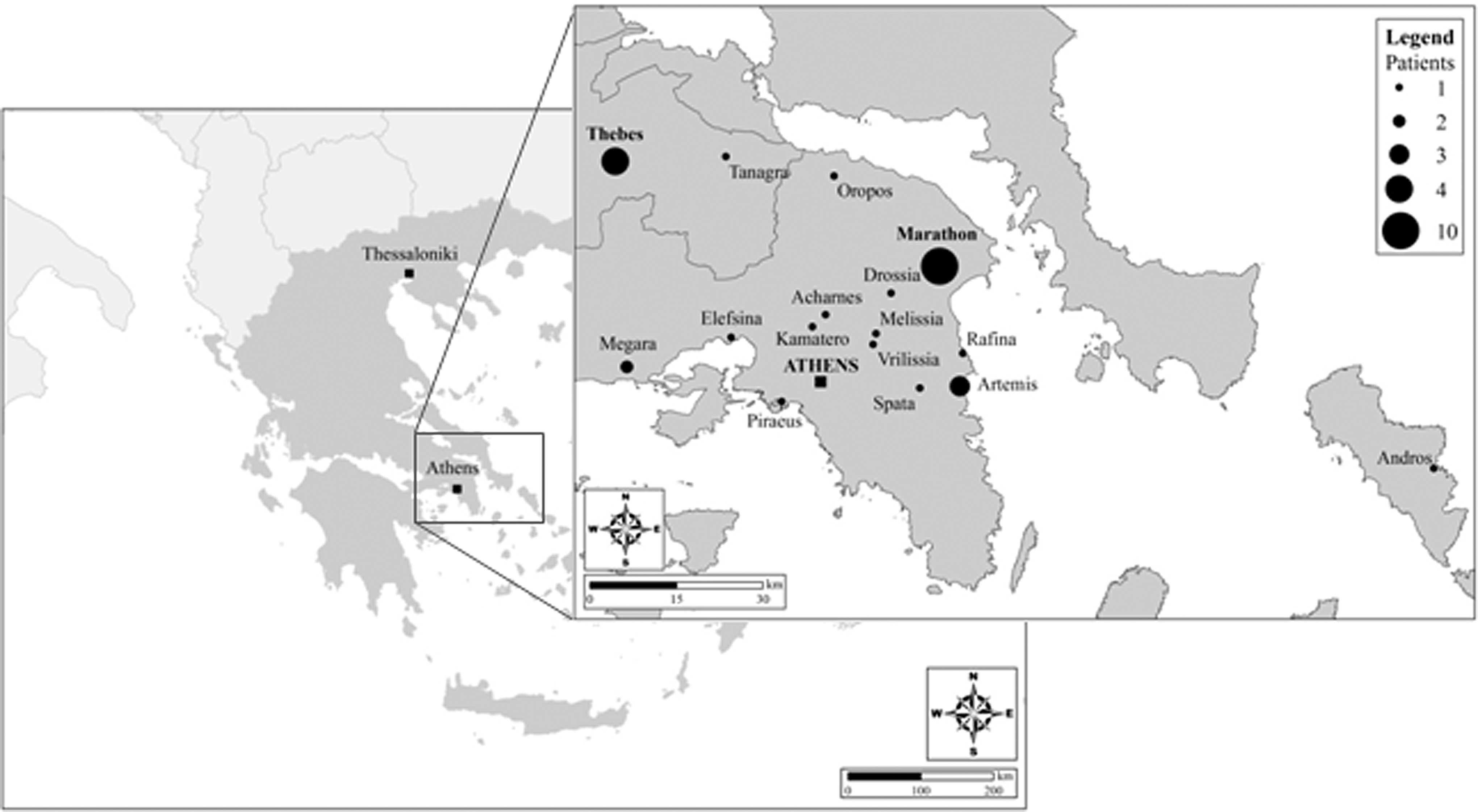
Geographic distribution of reported Wet Nile virus (WNV) infection cases during the 2011 outbreak in southern Greece.
Discussion
WNV is a re-emerging zoonotic pathogen of public health importance. During the summer–autumn of 2010, an outbreak of WNV infection occurred in Greece mainly localized in Central Macedonia (Papa et al. 2010a). This was the first time that WNV infection was documented in humans in Greece, although earlier serological surveys have detected WNV antibodies in approximately 1% of the population, suggesting that WNV or a related flavivirus was circulating in the country (Pavlatos and Smith 1964, Antoniadis et al. 1990, Papa et al. 2010b). Following the 2010 WNV outbreak, WNV human infections were notified in Greece for a second consecutive year. Although cases reoccurred in the same districts as in 2010, a new geographic pattern of WNV spread was observed during the summer of 2011. WNV dispersed southward to the newly affected areas of Thessaly region and further south to the prefectures of eastern Attica, especially in the municipality of Marathon, the fifth largest municipality of Attica in terms of land area (total area of 22.17 thousand hectares) (Fig. 2). This region contains the wetland of Schinia, a biotope that belongs to the Natura 2000 network (The Greek Biotope/Wetland Centre or EKBY by its Greek initials,
From August to October, 2011, serum, whole blood, and CSF specimens were collected from all individuals originating from southern Greece with signs and symptoms compatible to WNV infection. The preliminary diagnosis of WNV infection was based on the patient's clinical features, places and dates of travel. More detailed information was collected if the patient was from an area where WNV cases were not previously reported, activities, and epidemiologic history of the location where infection occurred. Standard laboratory diagnosis of WNV infections was generally accomplished by using an IgM antibody capture ELISA, which detects WNV IgM antibodies in the serum or CSF from individuals with clinically compatible illness. The presence of WNV IgM in the CSF was considered as an indication of intrathecal IgM synthesis and WNV central nervous system infection (Tardei et al. 2000).
Of the 31 detected cases, 25 experienced severe neurological manifestations and were classified as WNND cases. Twenty-one of these were considered confirmed whereas the remaining four were probable. Cases C1–C14 were confirmed because they exhibited meningeal and/or brain inflammation, and only WNV IgM antibodies were detected in all CSF and serum specimens (Table 1). Flaviviruses such as TBEV and DENV, which may cause cross-reactivity, are not endemic in Greece, and none of the tested patients had traveled in countries with TBEV or DENV endemicity.
The onset of symptoms is preceded by a period of viremia, which persists for only a short period, and disease usually manifests after the virus is no longer detectable. Due to low viremia at the time of clinical onset, WNV nucleic acid detection methods, despite their high specificity, are not recommended for diagnosis of WNV infection because of their limited sensitivity (Lanciotti et al. 2000). In that respect, all of the CSF and whole blood specimens tested for WNV RNA detection were found negative.
Previously, it has been shown that WNND incidence increases with increasing age, particularly among individuals older than 70 years of age, whereas higher incidence is observed among the male population (O'Leary et al. 2004; Danis et al. 2011). In our study, the median age of WNND cases was 67 years (range 25–86 years) with a higher incidence among males older than 70 years of age. The percentage of WNV-infected patients aged 60 years or older (79%) was approximately 20 times higher compared to that of individuals younger than 30 years.
Except for advanced age, increased risk in the development and severity of WNND is more often observed in immunosuppressed recipients of transplanted organs than in immunocompetent individuals (Jean et al. 2007, Centers for Disease Control and Prevention 2010). Hypertension and diabetes mellitus are also identified as possible risk factors for developing neuroinvasive disease rather than WNF (Jean et al. 2007). Diabetes may lead to an increase in the magnitude and duration of WNV viremia, whereas hypertension may cause disruption of the blood–brain barrier, promoting viral entry into the central nervous system (Colpitts et al. 2012). In the present study among WNND cases, eight had high blood pressure and seven were diagnosed with diabetes mellitus. Other underlying chronic conditions, such as coronary artery disease, alcoholism, and cerebrovascular and lung disease were less frequently observed. It is of note that the risk of WNND in solid organ transplant patients infected with WNV has been estimated to be as high as 40% (Kumar et al. 2004). In the present survey, there was one case of encephalitis in a kidney transplant patient. Most patients with WNND recover completely within days to months. However, patients with West Nile encephalitis have a poorer outcome than those with West Nile meningitis (Kramer et al. 2007). In accordance with this, all patients of the present study with unfavorable outcome suffered from encephalitis or meningoencephalitis.
In 2003 throughout North America, NAT of blood donors for WNV RNA was introduced as a screening tool for the identification of viremic donors during the preseroconversion phase of infection, avoiding transmission of WNV infection to patients via blood transfusion (Kleinman et al. 2005, Montgomery et al. 2006). In two of the six WNV-positive blood donors, development of IgM antibodies and IgG seroconversion occurred in both serum samples of the convalescent phase, over 2 weeks following the viremic donation, supporting serological testing during the seroconversion as a tool to confirm WNV infection among donors. WNV antibodies were not detected in the sera of the remaining four blood donors. This is not surprising because almost half of NAT-positive subjects may not be confirmed by subsequent serological testing (Colpitts et al. 2012). More specifically, a recent study has showed that from 1436 donors whose donations had initial WNV-positive molecular testing, 615 (42.82%) were unconfirmed cases or determined to have false-positive results (Zou et al. 2010). Moreover, it is probable that these sera were collected during the window period, a transient viremic phase between the time of WNV infection and the production of measurable anti-WNV antibodies.
In conclusion, the reoccurrence of human WNV infection cases in 2 consecutive years and the spread of the virus in newly affected areas suggest that WNV has been established in Greece and its transmission may continue to occur in the future. The identification of a human WNV infection is an important event that usually triggers public health alerts, mosquito control measures, and media attention. Laboratory test results should be interpreted accurately taking into account clinical manifestations, previous travel history, flaviviral vaccination history, and evidence of WNV activity in the area of interest.
Footnotes
Acknowledgment
This study was partially supported by the Hellenic Centre for Disease Control and Prevention.
Author Disclosure Statement
The authors declare no conflict interests.