
Abstract
Nosocomial salmonellosis continues to pose an important threat to veterinary medical teaching hospitals. The objectives of this study were to describe an outbreak of salmonellosis caused by Salmonella enterica serovar Oranienburg within our hospital and to highlight its unique features, which can be used to help mitigate or prevent nosocomial outbreaks in the future. We retrospectively analyzed data from patients that were fecal culture–positive for Salmonella Oranienburg between January 1, 2006, and June 1, 2011, including historical, clinical, and pulsed-field gel electrophoresis (PFGE) data. Salmonella Oranienburg was identified in 20 horses, five alpacas, and three cows during this time frame, with dates of admission spanning the period from August, 2006, through January, 2008. We consider most of these patients to have become infected through either nosocomial or on-farm transmission, as evidenced by molecular subtyping results and supportive epidemiologic data. Interpretation of PFGE results in this outbreak was challenging because of the identification of several closely related Salmonella Oranienburg subtypes. Furthermore, a high percentage of cases were fecal culture–positive for Salmonella Oranienburg within 24 h of admission. These patients initially appeared to represent new introductions of Salmonella into the hospital, but closer inspection of their medical records revealed epidemiologic links to the hospital following the index case. Cessation of this outbreak was observed following efforts to further heighten biosecurity efforts, with no known cases or positive environmental samples after January, 2008. This study demonstrates that a Salmonella-positive culture result within 24 h of admission does not exclude the hospital as the source of infection, and it underscores the important role played by veterinary medical teaching hospitals as nodes of Salmonella infection that can promote transmission outside of the hospital setting.
Introduction
T
Risk factors for nosocomial Salmonella infection among hospitalized horses include colic as the reason for admission (Hird et al. 1984, House et al. 1999), abdominal surgery (Ekiri et al. 2009), parenteral antimicrobial drug administration (Hird et al. 1984, House et al. 1999), nasogastric intubation (Hird et al. 1984), increased mean daily ambient temperature (House et al. 1999), and shedding of the same Salmonella serovar by other equine patients in the days prior to admission (House et al. 1999). The establishment of Salmonella transmission as nosocomial in origin requires a combination of historical, clinical, and laboratory data. Pulsed-field gel electrophoresis (PFGE) is a valuable molecular subtyping technique that can be combined with other forms of isolate characterization to more expeditiously investigate potential hospital outbreaks and to monitor for persistence of particular Salmonella strains within the hospital environment (Amavisit et al. 2001, Schott et al. 2001, Ward et al. 2005, Dunowska et al. 2007, Dallap Schaer et al. 2010, Steneroden et al. 2010). Controlling nosocomial outbreaks of salmonellosis requires the isolation of infected patients, the identification of subclinical shedders, and vigorous environmental disinfection protocols.
The objectives of this study were to describe a nosocomial outbreak of salmonellosis caused by Salmonella enterica serovar Oranienburg within our veterinary medical teaching hospital and to highlight its unique features, which can be used to help mitigate or prevent nosocomial outbreaks in the future.
Materials and Methods
Study design
We performed a retrospective analysis of patient records from animals presenting to Cornell University's Equine and Farm Animal Hospital (EFAH) between January 1, 2006, and June 1, 2011. Data were gathered for all patients that were fecal culture–positive for Salmonella Oranienburg during this time frame. In addition to historical and clinical data, variables collected from the patient records included the date of Salmonella isolation, antimicrobial susceptibility profile, and PFGE subtype.
Sample collection
For the purpose of Salmonella testing, clinicians and students in the EFAH were asked to routinely collect at least 10 grams of fecal matter from each patient on the day of admission. The fecal sample could be obtained directly from the rectum, during defecation, or from the stall floor. The sample was placed in a plastic specimen cup with a tight lid and transported directly to Cornell University's Animal Health Diagnostic Center (AHDC) for bacteriologic culture. Fecal samples collected after 5:00 PM were refrigerated overnight at 4°C before submission. Sample collection could have been delayed (>24 h past admission) or not performed at all for a variety of reasons, including lack of manure on presentation or emergency situations.
Animals that presented as salmonellosis suspects (diarrhea or fever of unknown origin) were admitted directly to the isolation ward, and multiple fecal samples were collected from these patients (up to five negative samples or until found to be Salmonella-positive). Animals that developed clinical signs of salmonellosis while hospitalized were promptly transferred to isolation and repeatedly sampled as described.
Approximately 30 environmental samples were collected monthly by the hospital biosecurity officer for Salmonella culture. Areas of focus included floors and drains throughout the hospital, stall walls and floors, and equipment. During periods of increased Salmonella-positive fecal samples, additional environmental surveillance was conducted. If a patient was found to be shedding Salmonella or was a salmonellosis suspect, samples from the stall (floor, walls, and feed/water containers) and surrounding environment were collected following cleaning and disinfection (Trifectant, Vetoquinol USA, Fort Worth, TX). In the event of a positive Salmonella culture result, the stall would be disinfected and sampled again until negative culture results were obtained. All environmental samples were collected using sterile 4-×4-inch gauze pads saturated in double-strength skim milk.
Microbiologic procedure for Salmonella detection
Personnel at the AHDC used standard bacteriologic culture methods to isolate Salmonella from fecal and environmental samples (Carter and Cole Jr. 1990). Individual swab specimens from each sample were enriched in 10 mL of Tetrathionate Broth (Difco, Detroit, MI) containing 0.2 mL of iodine solution; the mixture was incubated at 42°C for 18–24 h. After incubation, the sample–broth mixture was streaked onto Brilliant Green agar with novobiocin (Becton, Dickinson and Company, Franklin Lakes, NJ) and Xylose Lysine Tergitol-4 (XLT-4) selective media, and both plates were incubated at 35°C for 18–24 h. Red colonies (lactose-nonfermenting bacteria) on Brilliant Green agar with novobiocin and black colonies (hydrogen sulfide–producing bacteria) on XLT-4 were inoculated into Kligler Iron Agar slants (Becton, Dickinson and Company) and then incubated at 35°C for 18–24 h. XLT-4 plates without suspected colonies were reincubated at 35°C for an additional 18–24 h before checking again for characteristic black colonies. Colonies on Kligler Iron Agar slants that exhibited the biochemical properties of Salmonella were then serogrouped by slide agglutination using standard protocols. Those colonies that were positive by slide agglutination were then identified as Salmonella using the Sensititre Automated Microbiology System's A80 panel (TREK Diagnostic Systems, Cleveland, OH). Confirmed Salmonella isolates were sent to the National Veterinary Services Laboratories (Animal and Plant Health Inspection Service, United States Department of Agriculture) in Ames, Iowa, for serotyping using standard protocols (Edwards and Ewing 1972).
Antimicrobial susceptibility testing
Antimicrobial susceptibility of Salmonella isolates was determined by use of the microbroth dilution method (Sensititre, TREK Diagnostic Systems). Minimal inhibitory concentrations (MIC) were established for each isolate against various panels of antimicrobial agents. Clinical and Laboratory Standards Institute (CLSI) guidelines were used to interpret MIC values when available (Clinical and Laboratory Standards Institute 2008). Otherwise, MIC values were interpreted using National Antimicrobial Resistance Monitoring System (NARMS) breakpoints (Food and Drug Administration 2011). Isolates were classified as being resistant or susceptible to each agent; those isolates with intermediate susceptibility were categorized as being susceptible. Quality control was performed weekly using four strains of bacteria: Escherichia coli ATCC 25922, Staphylococcus aureus 29213, Enterococcus faecalis 29212, and Pseudomonas aeruginosa 27853. The MIC ranges for quality control recommended by the CLSI were used, and results were accepted if the MIC values were within expected ranges for these bacterial strains.
Pulsed-field gel electrophoresis
PFGE subtyping of Salmonella Oranienburg isolates was performed in the Food Science Laboratory (FSL) at Cornell University, using the standard Centers for Disease Control and Prevention PulseNet protocol (Ribot et al. 2006). XbaI was used as the restriction enzyme, and XbaI-digested S. enterica serovar Braenderup (CDCH9812) DNA was used as a reference size standard (Hunter et al. 2005). Electrophoresis was performed for 21 h using the CHEF Mapper apparatus (Bio-Rad Laboratories, Hercules, CA). Pattern images were captured with a Bio-Rad Gel Doc and Quantity One 1-D Analysis software (Bio-Rad Laboratories). PFGE patterns were then analyzed and compared using BioNumerics version 5.1 software (Applied Maths, Inc., Austin, TX). Similarity analyses were performed in BioNumerics based on the Dice correlation coefficient with a tolerance of 1.5%, and cluster analysis for generating dendrograms was performed using the unweighted pair group method with arithmetic mean (UPGMA) algorithm. PFGE patterns were also compared to a set of Salmonella Oranienburg PFGE patterns in the FSL database, representing isolates obtained from human and animal (e.g., alpaca, bovine, equine) sources in New York between 2004 and 2010. PFGE data for all isolates are publicly available (
Results
Salmonella Oranienburg was identified in 28 EFAH patients between January 1, 2006, and June 1, 2011, with dates of admission spanning the period from August, 2006, through January, 2008. During this time frame, the EFAH received approximately 3500 patient visits annually. In August of 2006, the index case (8-year-old mixed-breed mare) presented to the EFAH with a chronic draining tract involving the right hind sole. Cultures of both feces and infected hoof tissue (taken aseptically during surgical debridement) were positive for Salmonella Oranienburg. The mare had been walked repeatedly throughout the hospital (e.g., radiology and surgery areas) prior to receipt of these culture results. Over the next year and a half, 27 additional patients were identified as being fecal culture–positive for Salmonella Oranienburg: 19 horses, five alpacas, and three cows. The last patient known to be positive for Salmonella Oranienburg was admitted in January of 2008. The median age among all patients was 3 years (range, 2 weeks to 25 years). The median duration of hospitalization was 6.5 days (range, 2–63 days), and the median number of days hospitalized prior to being identified as fecal culture–positive was 2 (range, 1–15 days). During the course of hospitalization, 46% (13/28) of patients had diarrhea, 46% (13/28) had a temperature in excess of 102.0°F, and 44% (8/18) had a white blood cell (WBC) count <4000 WBC/μL. Nine patients (32%) did not have diarrhea, a temperature >102.0°F, or leukopenia while hospitalized. Five patients (18%) were euthanized.
Salmonella Oranienburg was isolated from six of 1182 environmental samples (0.5%) collected during the 2006–2008 outbreak period. Positive samples were obtained from two isolation stalls that had previously housed Salmonella Oranienburg–positive patients, the floor of the intensive care unit where equine colic patients were housed, the floor of the cattle barn, an equipment cart, and a rope used with down cows.
Antimicrobial susceptibility testing was performed on 40 isolates from the 28 Salmonella Oranienburg–positive patients (Table 1). Of the seven patients from which multiple isolates were tested, six yielded isolates with the same resistance profile each time. Resistance to individual antimicrobial agents ranged from 0% (amikacin and marbofloxacin) to 100% (ampicillin, cephalothin, and tetracycline) of isolates. More than 75% of isolates were also resistant to each of the following agents: ceftiofur, chloramphenicol, gentamicin, and trimethoprim/sulfamethoxazole.
PFGE subtyping was performed on 59 isolates from the 28 positive patients (including the initial isolates from each, plus 25 isolates generated from repeated sampling of 10 patients) and six positive environmental samples (Fig. 1). A total of 21 PFGE types were differentiated. There were four predominant types, with seven to nine isolates corresponding to each type; the maximum band difference between any two types was three. The number of isolates corresponding to each of the other 17 PFGE types ranged from one to four. Patients were typically sampled on repeated occasions (up to seven times) to investigate persistent shedding of Salmonella Oranienburg, and 10 patients yielded multiple isolates. Isolates obtained from the same patient over time did not share the same PFGE type for nine of 10 patients. In most instances (eight of nine), PFGE types of isolates from the same patient differed by one to three bands. PFGE patterns of the 59 EFAH isolates were compared to PFGE patterns of 62 (presumably unrelated) Salmonella Oranienburg isolates in the FSL database, obtained from human and animal sources in New York between 2004 and 2010. A total of 29 PFGE types were differentiated among the comparison isolates, and only four of these were also identified among the EFAH isolates.
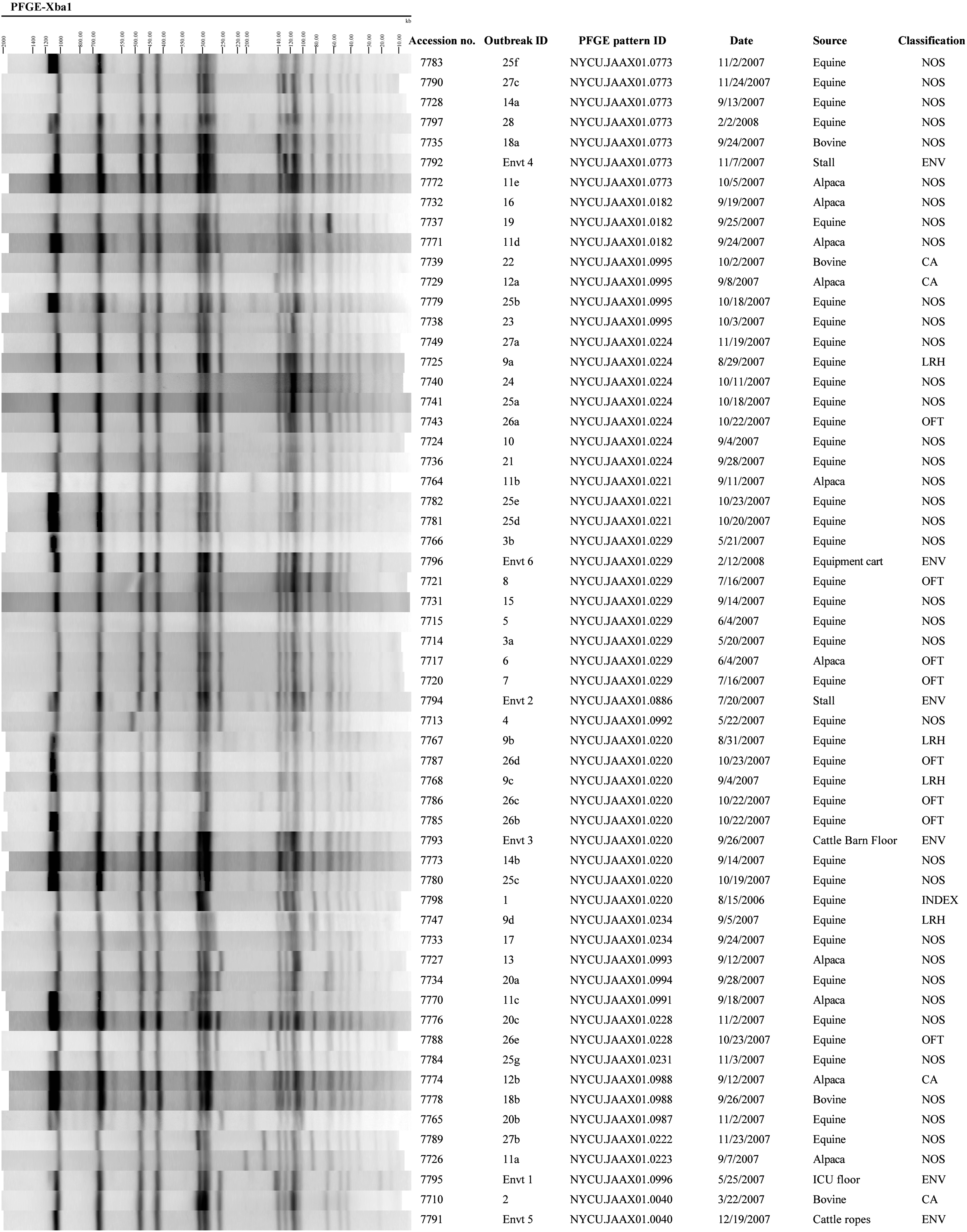
XbaI pulsed-field gel electrophoresis (PFGE) patterns for 59 S. enterica serovar Oranienburg isolates from 28 positive patients (including isolates generated from repeated sampling of patients) and six positive environmental samples. Outbreak ID denotes the patient number (in some cases followed by a letter to indicate sequential isolates from the same patient over time) or environmental sample number. Classification denotes either index case (INDEX), nosocomial transmission (NOS), on-farm transmission (OFT), linked to referral hospital (LRH), community-acquired (CA), or environmental sample (ENV).
Of the 27 patients that were admitted to the EFAH following the index case, 19 (70%) were believed to have become infected via nosocomial transmission. Fourteen of these patients, representing a wide range of chief complaints, were found to be fecal culture–positive for Salmonella Oranienburg between 3–13 days past their admission date, following an initial negative Salmonella culture at the time of admission. The other five patients believed to have nosocomial infections were fecal culture–positive for Salmonella Oranienburg at admission; two of these presented with a chief complaint of diarrhea. However, all had been previously hospitalized at the EFAH following the index case, and some overlapped temporally with other patients known to be positive for Salmonella Oranienburg. These five patients likely became infected during their previous hospital visit. Four of the 27 patients (15%) originated from farms that were regular clients of the EFAH and that had been the source of multiple admissions to the hospital following the index case. Two of these patients presented with a chief complaint of diarrhea, and all four were fecal culture–positive for Salmonella Oranienburg at admission. Thus, these patients were believed to have become infected on their home farms via transmission from herd mates that had recently visited the EFAH during the outbreak. One of the 27 patients (4%) had previously been treated at a private referral hospital (approximately 100 miles away) that frequently referred patients to the EFAH. Several animals that visited the EFAH during this time frame, including the index case, had been treated and in some cases hospitalized at this referral facility beforehand. This patient presented with colic signs and was fecal culture–positive for Salmonella Oranienburg at admission. Therefore, it is likely that this patient became infected through nosocomial transmission at the private referral hospital.
The final three of 27 patients (11%) appeared to have community-acquired infections that were not epidemiologically linked to the EFAH. A cow admitted for a cesarian section, a calf with diarrhea, and a cria with otitis media/interna were fecal culture–positive for Salmonella Oranienburg at admission. None had been previously hospitalized at the EFAH following the index case, and none had originated from farms that sent other animals to the hospital following the index case. The PFGE type of the cow isolate differed from that of the index case isolate by more than three bands, but it matched a PFGE type that was evident among 20 of the 62 external comparison isolates. The PFGE types corresponding to the calf and cria isolates did not match any PFGE types among the external comparison isolates.
Discussion
The reported Salmonella outbreak among horses, alpacas, and cows was caused by a serovar that appears to be uncommon in these species based on previous large-scale prevalence studies in the United States (Traub-Dargatz et al. 2000, Centers for Epidemiology and Animal Health 2009). To our knowledge, this is the first outbreak caused by Salmonella Oranienburg in a veterinary medical teaching hospital. One of the hurdles associated with the investigation of this outbreak was the high degree of genetic diversity displayed by the isolates. Although PFGE has been shown to be a valuable method for analyzing veterinary hospital outbreaks (Cummings et al. 2010), interpretation of PFGE results in this outbreak was challenging because of the identification of several closely related Salmonella Oranienburg subtypes. Isolates that differ from each other by up to three bands are generally regarded as closely related, because these differences can arise from a single genetic event (van Belkum et al. 2007). Isolates with this level of genetic similarity can therefore be implicated in a given outbreak if supportive epidemiologic data are available. A comparable degree of PFGE variation was detected in a recently reported outbreak of Salmonella Oranienburg among calves on a dairy farm (Kaneene et al. 2010). In another recent study, isolates obtained over time from a Salmonella Oranienburg–positive horse following hospital discharge yielded four PFGE types that differed from the initial isolate subtype by one to three bands (Jay-Russell et al. 2014). The presumably rapid diversification of Salmonella PFGE types during outbreaks among humans or during environmental persistence in production or farm environments has also been reported previously (Tassios et al. 2000, Martinez-Urtaza and Liebana 2005, Dunowska et al. 2007, Ethelberg et al. 2007, Uesugi et al. 2007). However, the high genetic diversity observed in our study, with multiple PFGE types associated with isolates collected from the same animal over a period of days, exceeds that reported in most studies. Potential mechanisms of Salmonella Oranienburg diversification over the course of this outbreak include loss or acquisition of mobile genetic elements (e.g., plasmids, phages, or transposons), nonhomologous recombination events, chromosomal rearrangements (e.g., inversions), or point mutations (Cooke et al. 2008). While rapid diversification of Salmonella Oranienburg during this outbreak provides the most likely explanation for the observed range of PFGE types, especially for isolates collected from the same animal, co-infection by multiple circulating Salmonella Oranienburg subtypes or reinfection by closely related strains cannot be excluded as causing or contributing to the PFGE diversity detected within this outbreak.
Another challenging aspect of this outbreak investigation was the high percentage of cases that were fecal culture–positive for Salmonella Oranienburg within 24 h of admission. These patients initially appeared to represent new introductions of Salmonella into the hospital, but closer inspection of their medical records revealed epidemiologic links to the EFAH through previous hospitalization of themselves or herd mates following the index case. Many veterinary medical teaching hospitals have traditionally defined nosocomial cases as patients found to be shedding Salmonella 48–72 h after admission, following an initial negative culture result; however, this is based on limited scientific evidence (Aceto et al. 2011). This study demonstrates that a Salmonella-positive culture result within 24 h of admission does not exclude the hospital as the source of infection. Furthermore, the conventional definition of nosocomial cases is limited by the imperfect sensitivity of bacteriologic culture for detecting Salmonella in feces (Smith et al. 1978, van Duijkeren et al. 1995). A single negative culture result at admission does not rule out Salmonella shedding at that point in time, and this can result in misclassification. Thus, it is possible that some of the 14 cases found to be negative within 24 h of admission were in fact shedding Salmonella at that time, although none of these patients had known previous links to the EFAH during the outbreak period.
Few data have been published regarding the risk of Salmonella transmission from hospitalized patients to herd mates following discharge (Hartnack et al. 2012). Widespread environmental contamination can result from fecal shedding of Salmonella Oranienburg (Jay-Russell et al. 2014), and Salmonella has been found to persist in farm environments for more than 9 months (Toth et al. 2011). In this study, there was evidence that animals became infected on their home farms via transmission from herd mates that had recently visited the EFAH during the outbreak. This underscores the important role played by veterinary medical teaching hospitals as nodes of Salmonella infection that can promote transmission outside of the hospital setting.
Cessation of this outbreak was observed following efforts to further heighten biosecurity efforts at our veterinary medical teaching hospital, with no known cases or positive environmental samples after January, 2008. Additional measures have included biosecurity training sessions for hospital personnel, additional restrictions on human traffic, disinfectant footbaths containing Trifectant in front of every stall and at the entrance to each hospital ward, an increase in hand disinfection stations throughout the hospital, twice-weekly (Monday and Thursday) fecal Salmonella cultures performed on all hospitalized patients (with samples being obtained directly from the rectum or during defecation), and fecal Salmonella cultures performed on all outpatients. An electronic mailing list was also established to notify the hospital director, biosecurity committee, clinicians, technicians, and barn manager of any suspicious Salmonella cultures before the official laboratory report is confirmed. The patient in question is considered a Salmonella suspect and immediately placed in temporary isolation until final culture results are confirmed, generally within 24 h of the initial notification. Temporary isolation involves the application of Tyvek (DuPont, Wilmington, DE) coveralls, exam gloves, and plastic boots prior to entering the stall, with removal and disposal upon exiting; access to such patients is limited to those directly involved in their care. Floors throughout the hospital continue to be disinfected with Trifectant or a similar product at least twice daily, using an industrial walk-behind scrubber (Advance Convertamatic, Nilfisk-Advance, Inc., Plymouth, MN). Finally, PFGE subtyping continues to be performed at the time of Salmonella isolation from fecal and environmental samples to facilitate assessment of epidemiologic relatedness.
Footnotes
Acknowledgments
We thank Linda Caveney, Cameron Gurney, Paula Sharp, and Julie Siler for their assistance.
Author Disclosure Statement
No competing financial interests exist.