
Abstract
Three cases of relapsing fever from southern Israel were diagnosed promptly thanks to vigilance of the hematology laboratory technicians. In this region of Israel, patients presenting with prolonged fever and leukopenia without localizing symptoms are generally suspected of having brucellosis or a rickettsial disease. Pediatric patients with prolonged fever, cytopenias, and negative aforementioned serologies are often hospitalized for further work-up. Because of the policy of performing a manual blood smear when results of the automated blood count demonstrate severe anemia and abnormal platelet and/or white blood cell counts, a diagnosis of tick-borne relapsing fever was confirmed and promptly relayed to the physician. This routine prevented unnecessary examinations and hospitalization days and provided important information to regional epidemiology and public health authorities.
Introduction
T
The number of yearly cases of TBRF in Israel is reported to vary between 6–16/100,000 according to studies conducted in both civilians and soldiers in recent years (Assous and Wilamowski 2009). Although TBRF mandates reporting to the Israeli Ministry of Health (MoH), this rate is probably severely underestimated, as prolonged fever and a cytopenia in the region often generate a differential diagnosis of rickettsiosis and brucellosis.
A blood smear is not among the usual tests requested. Often, doxycycline is initiated empirically with this clinical presentation.
The regional hematological laboratory serves a 1000-bed teaching hospital and the primary care clinics of about 150,000 residents insured by a large managed care organization. In the laboratory, a manual blood smear is routinely performed when the automated complete blood count (CBC) shows at least one of the following parameters: White blood cells (WBC)<3500/μL, absolute neutrophil count (ANC)<1000/μL, hemoglobin (Hgb)<8 grams/dL, and platelets (Plt)<100,000/μL. Typically, several organisms are observed per oil immersion field in routine analysis of fixed blood smears of patients during the acute febrile phase of TBRF, assuming a sufficiently high rate of spirochetemia (Cobey et al. 2001, Dworkin et al. 2008). However, even experienced laboratory technicians might require a search through many fields before detecting spirochetes, and must be mindful of the potential diagnosis. The sensitivity of thick and thin blood smears is reported to average about 80% compared to molecular analysis in studies conducted in Israel (Assous and Wilamowski 2009). Specifically, an assay targeting the glycerophosphodiester phosphodiesterase gene detected TBRF in 19 patients with a positive blood smear and in two additional patients with clinical symptoms and a negative blood smear (Halperin et al. 2006).
Herein, we present three cases, where the diagnosis of TBRF was confirmed by the hematological laboratory before it was considered by the physician and prompted appropriate management of the cases.
Case 1
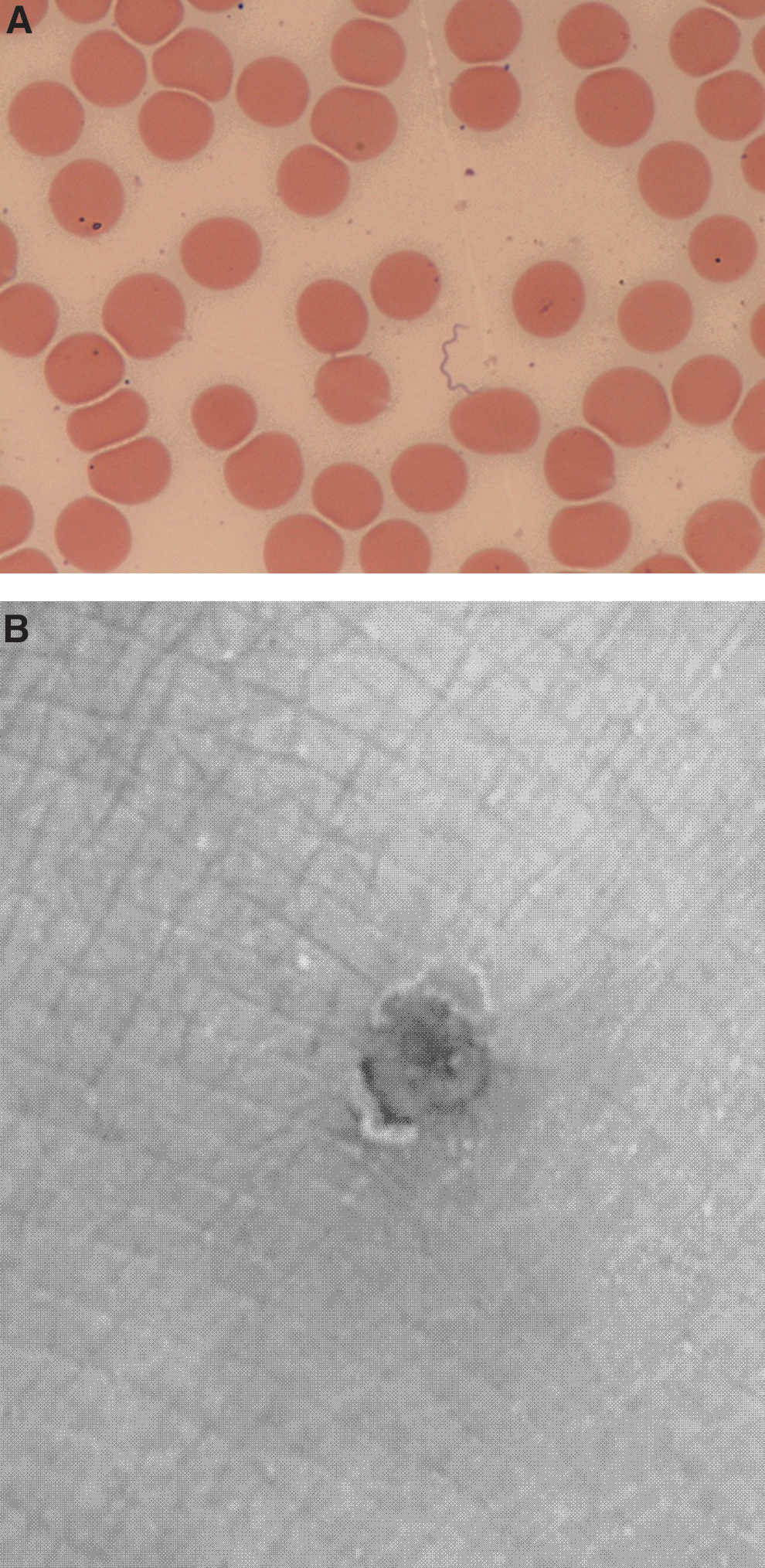
A 29-month-old Bedouin girl living on the outskirts of a rural township in southern Israel was referred to the pediatric emergency room (PER) because of a 2-week-long persistent fever. Three weeks before admission, her mother noticed three bite marks on her right shin. One week later, the child developed a relapsing fever up to 39.3°C accompanied by irritability, a reduced appetite, and a petechial rash on her face. She was treated with amoxicillin. However, the fever recurred daily and responded to paracetamol suppositories. Investigation at her primary care clinic included a normal urine sample and mixed growth on urine culture. There was elevated erythrocyte sedimentation rate (ESR) of 100 mmHg/hr and normal blood chemistry. The day before her admission, the CBC revealed hypochromic microcytic anemia: Hgb 6.6 % g/dL, hematocrit (Hct) 21.2 %, and normal white blood cell and platelet counts. The hematology laboratory contacted the primary care physician, and reported detection of spirochetes on the peripheral blood smear (Fig. 1A).
(
Upon admission, the patient was afebrile with no signs of dehydration or respiratory distress. Hepatomegaly and splenomegaly were noted, and repeat ESR was 110 mmHg/h. Blood cultures were negative, and thick smear performed on the blood sample collected in the PER revealed spirochetes, confirming the oupatient blood smear findings. Upon directed questioning, her mother reported frequent family visits to caves in the hills close to their home. Treatment with erythromycin 250 mg 3×/day was initiated. In light of the rapid diagnosis, the patient was observed in the hospital for only 1 day and discharged home to complete 10 days of treatment. She recovered uneventfully. The Ministry of Health was notified of the case.
Case 2
A 31-year-old Bedouin man presented to his primary care physician with fever and muscle ache. The physician noted three bite marks on the patient's left shin with no eschar or cellulitis (Fig. 1B). A CBC, serum chemistry, and serological tests for Brucella and Rickettsia were ordered. The following day the CBC parameters were: Hgb 13.6 grams/dL, Hct 38.0, Plt 52,000/μL, and WBC 8900/μL. The hematology laboratory technician contacted the clinic to inform the physician that the peripheral smear was positive for Borrelia spirochetes. Upon requestioning, the patient remembered he had hiked to a dry creek bed and rested in a shaded enclave where he experienced an insect bite 10 days before symptom onset.
The patient received doxycycline 100 mg b.i.d. for 7 days with no evidence of the Jarisch–Herxheimer reaction. The following day he was feeling better and his serum creatinine normalized.
Case 3
A 12-year-old girl was admitted to the pediatrics ward due to a week-long fever of 40°C and recurrent vomiting. A CBC at the PER showed Hgb 12.3 grams/dL, WBC 9900/μL, and Plt 77,000/μL. Her peripheral blood smear was positive for spirochetes. She received intravenous fluids and doxycycline 100 mg 2×/day. She was discharged the following day after her fever remitted and vomiting subsided to complete 10 days of antibiotics.
Conclusions
Moderate-to-severe thrombocytopenia, with or without anemia, in a febrile patient is a typical finding in acute TBRF (Cobey et al. 2001). None of the physicians caring for the patients presented requested a blood smear to rule out borreliosis, although all of the patients described herein lived in endemic areas, reported outdoor exposure, and presented with fever and cytopenia. The cases reiterate the appropriateness of the hematological laboratory's practice to perform a manual smear when certain parameters appear in the automated CBC. The laboratory diagnosis promptly ascertained the cause of the cytopenia and prevented prolonged untreated illness, a battery of unnecessary investigations, and additional preventable medical costs. This study emphasizes the need for both: (1) Increased awareness among local clinicians of a diagnosis of TBRF in the appropriate clinical scenario, and (2) the contribution of blood smear microscopy or the available molecular analysis in the reference laboratory if TBRF is suspected. Finally, although Israel has been declared malaria free, a thick blood smear is indicated as part of the investigation of fever in a returning traveler to rule out malaria, babesiosis, human ehrlichioses, and other borrelioses depending on the destination (Gallien et al. 2007, Nackos and DeSancho 2014).
Footnotes
Acknowledgments
The authors would like to thank and commend the staff of the SUMC hematology lab for their vigilance.
Author Disclosure statement
No competing financial interests exist.