
Abstract
Background:
The early diagnosis of asymptomatic, acute, and subclinical Leishmania infections remains a challenge for controlling visceral leishmaniasis (VL). Individuals with acute VL represent <1% of Leishmania infections occurring in active transmission endemic areas. In this cross-sectional study with a prospective follow-up, we explored the risk factors associated with acquisition of Leishmania infection in an area with newly identified endemic VL.
Materials and Methods:
Ninety-four households were randomly selected from the study area, which included a population of 213 individuals (10% of the total population of Pé de Areia, Bahia, Brazil). Clinical and epidemiological surveys were prospectively performed to detect cases of asymptomatic infections, acute VL, and subclinical VL, using the leishmanin skin test (LST), and serological response to two Leishmania-specific antigens: rK39 and rK26.
Results:
Within the 92 households included in the study, the prevalence of Leishmania infection in individuals detected by positive serology was 91/197 (46.2%; 95% CI: 0.3937–0.5316) and by LST was 29/114 (25.4%; 95% CI: 0.1834–0.3414). Reactivity to both antigens was detected in 64/197 individuals (32.5%; 95% CI: 0.2634–0.3931). Among 89 individuals diagnosed with leishmaniasis, we found acute VL in one (1%), subclinical VL in 20 (22.5%), and asymptomatic Leishmania infection in 68 (76.4%) subjects. Use of repellents and bed nets showed no significant protection (prevalence ratio [PR] = 1.01, p = 1.0). Interestingly, individuals residing in houses with a sand backyard had significant protection against Leishmania infection (PR = 1.24, p = 0.049) compared to those with a different type or no backyard. Moreover, the presence of cat or dog at home was also not a risk factor (dog: PR = 1.14, 95% CI: 0.80–1.64; and cat: PR = 1.19, 95% CI: 0.78–1.81). We conclude that in newly discovered areas of transmission of L. infantum infection with sylvatic reservoirs, periodic surveys may be helpful in identifying risk factors for infection and optimizing prevention guidelines.
Introduction
V
In the Americas, the most common cause of VL has been L. chagasi, which has been shown to be genetically the same as L. infantum (Lainson and Shaw 1978). VL occurs following the transmission of Leishmania spp. by sand flies of the genus Phlebotomus (Old World) or Lutzomyia (New World) (Gramiccia and Gradoni 2005, Velo et al. 2005). Other nonvector-borne transmissions have been reported in laboratory accidents, blood transfusions, organ transplantation, and from shared needles between drug users, but these cases are rare (Badaro et al. 1986, Cruz et al. 2002, Cardo 2006, Cruz et al. 2006). Human infections occur in proximity to sylvatic or domestic zoonotic reservoirs, as well as from human-to-human transmissions following the anthroponotic cycle of some sand fly species (Manson-Bahr 1971, Herwaldt 1999, Herrero et al. 2009, Quinnell and Courtenay 2009). Reservoir hosts include a long list of mammals (e.g., domestic dogs, opossums, rodents, and sloths). In the Americas, wild reservoir hosts include foxes (Cerdocyon thous and Lycalopex vetulus) and opossums (Didelphis albiventris) (De Alencar 1958, Sherlock and Guitton 1969, Quinnell and Courtenay 2009). However, domestic dogs are the main reservoirs within the endemic areas of Brazil (Ashford et al. 1998).
The WHO estimates that 400,000–500,000 new VL cases occur annually, resulting in 40,000–50,000 deaths worldwide (Desjeux 2004, World Health 2010). Among the 65 countries reporting cases of VL, 90% of cases are from Bangladesh, India, Brazil, Nepal, Ethiopia, and Sudan (World Health 2010, Alvar et al. 2012). One of the key challenges in the control of VL is the identification of risk factors associated with the occurrence of VL in endemic areas. Environmental, socioeconomic, and host immune risk factors have all been associated with disease in high-transmission areas (Ryan, et al. 2006, Sampaio et al. 2010, Singh et al. 2010, Argaw et al. 2013, Belo et al. 2013, Burza, et al. 2014). The classic acute VL syndrome, characterized by fever, hepatosplenomegaly, and pancytopenia, occurs in <1% of the active Leishmania infections that occur in endemic areas of Brazil (Badaro et al. 1996, Ready 2014). However, early diagnosis of recently infected patients with asymptomatic and subclinical Leishmania infections has been shown to decrease mortality (Badaro et al. 1986, Jeronimo et al. 1994, Bern et al. 2007, Martins-Melo et al. 2014).
Despite the well-known epidemiological characteristics of this zoonotic disease in the Americas and its anthroponotic behavior in India, neither controlling sand fly bites with insecticides nor reservoir elimination has been capable of eliminating Leishmania transmission to humans in endemic areas (Marinkelle 1980, Chappuis et al. 2007, Quinnell and Courtenay 2009). As cities encroach into forests in tropical areas, natural reservoirs are increasingly in contact with humans, making leishmaniasis a growing urban problem (Jeronimo et al. 1994, Cunha et al. 1995, Diniz et al. 2008, Albuquerque et al. 2009). To date, few cohort studies have described the risk factors associated with L. infantum infection (Caldas et al. 2002, Belo et al. 2013, de Araujo et al. 2013). In this study, we explored the risk factors associated with Leishmania infection in a zone centered around a previously identified endemic area in the State of Bahia in Brazil (Cunha et al. 1995).
Materials and Methods
Study design
This is a cross-sectional study with a longitudinal follow-up conducted in an endemic area for VL in the City of Pé de Areia, Municipality of Camaçari, Bahia, Brazil, from January 2011–2013. This study zone is an expansion from a well-studied area in the Municipality of Monte Gordo. A new ecological niche of L. infantum infection was discovered here in 1995. The presence of VL was demonstrated by a cross-sectional epidemiological study, where isolation and identification of L. infantum were documented in dogs and humans (Cunha et al. 1995).
Study cohort
To calculate the appropriate sample size, we assumed an expected prevalence of 10% with a 95% confidence interval. We assumed an error for this expected prevalence of 4% plus 20% for possible losses and an additional 50% for design effect. Based on these calculations, we needed to select 94 households in the city to reach the minimum sample size of 213 people to represent the population of 3364 individuals. For definition of households, we used geometric progression; all individuals of each selected household present for the visit were invited to participate in the study; in the event no residents of the household accepted enrollment, that house was excluded from the study and was replaced by the nearest residence. In cases of equal distances, the nearest home on the left side, based on our maps, was chosen.
Collection of blood samples
After agreeing to participate in the study and providing informed consent, two samples of whole blood (a total of 8 mL) were collected from each participant. Blood samples were collected in Vacutainer™ tubes by peripheral venipuncture and then centrifuged for 10 min at 4000 rpm. Serum was then separated, aliquoted into cryovials, and stored at −20°C until used.
Leishmanin (Montenegro) skin test
To perform the leishmanin skin test (LST), 0.1 mL of leishmanin solution (L. amazonensis antigen, strain BA125, 50 μg/mL) was injected intradermally into the right forearm of individuals as previously reported (Reed et al. 1986). All results were measured 48 h after the application of the leishmanin. Induration ≥5 mm was considered positive.
Serological tests
ELISAs to detect antibodies to the rK39 and rK26 antigens were performed as described elsewhere (Badaro et al. 1986). Briefly, anti-rK39 antibody was detected by indirect ELISA using polystyrene microplates sensitized with rK39 antigen (50 ng/well). Serum from each patient was diluted in phosphate-buffered saline (PBS) with Tween 20 diluted in bovine serum albumin solution at 0.1%. Fifty microliters of diluted serum was placed into the wells from each individual tests. Microplates were incubated for 20 min at room temperature and then washed five times with PBS with 0.05% Tween 20, pH 7.4 buffer, and air-dried. Fifty microliters of peroxidase conjugate (protein A) solution diluted 1:10.000 μL was placed into each well. The microplates were incubated for 20 min and then washed five times with PBS with 0.05% Tween 20, pH 7.4 buffer, and air-dried. After drying, 50 μL TMB peroxidase substrate was added to each well. After a 15-min incubation at room temperature, the reaction was stopped by adding 50 μL of 1N H2SO4 to each well. The microplates were read in a spectrophotometer (ELx800, BioTek Instruments, Inc.) with an absorbance filter of 450 nm. ELISAs following the same protocol used for ELISA-rK39 were performed to detect the anti-rK26 antibodies using plates sensitized with rK26 antigen in the concentration of 200 ng/well. If the ratio of optical density of the individual's sample to the cutoff was ≥1.4, ELISA was considered positive. Both tests were used for screening in this study to optimize detection of cases as results between these two tests are not 100% concordant (Badaro et al. 1986).
Criteria for considering an individual infected with Leishmania
All individuals who were positive by the LST test (i.e., induration >5 mm) or had a positive ELISA either to rK39 or to rK26 were considered to be infected with Leishmania.
Follow-up of infected subjects
All subjects found to have evidence of Leishmania infection during the cross-sectional analysis were monitored at 6-month intervals over a 2-year period to determine the presence and extent of clinical symptoms. If the subject was asymptomatic or only liver enlargement was noted without any other signs and symptoms, treatment was postponed until the next evaluation with the expectation that most individuals would self-heal. If after the second evaluation 6 months later, no progression or regression of symptoms was noted, further monitoring was performed by the local healthcare system with instructions to report the development of VL to the study team.
Statistical analysis
Description of analyzed variables
For households, we analyzed the following variables: presence of backyard, type of the yard, presence of animal pets, specific type of pet, use of repellents, and presence of cohabiting resident with Leishmania infection.
For individuals, we analyzed the following variables: gender, age, serological results of rK39-ELISA and rK26-ELISA, LST, status of Leishmania infection (i.e., treated), and type of infection (asymptomatic, subclinical, or acute).
Descriptive analysis was used for measures of frequency, central tendency, and dispersion. For inferential statistics, prevalence ratio, kappa index, and prevalence-adjusted and bias-adjusted kappa (PABAk) were used to analyze concordance between diagnostic tests; chi-square test, McNemar test, Fisher's exact test, Kruskal–Wallis test, and Mann–Whitney test were used to analyze bivariate relationships between Leishmania infection and risk factors, and Poisson regression multilevel analysis agreement was used to perform multivariate analysis. The exact test applied was dependent on the type of variable tested and adjusted for the type of sampling used. The choice of variables for modeling was based on the theoretical construct of possible associations described in the literature and the greatest relative frequencies found in the bivariate analysis: the presence of a dog in the residence, presence of a cat, type of yard, and use of repellent methods by the study subject. The database was built in Excel (version 2007), and the analysis was performed in R version 3.1.1 software.
Ethical issues
This study was approved by the Institutional Research Ethical Committee of the University Hospital Professor Edgard Santos (HUPES) following the recommendations of the Minister of Health Resolution CNS 466/2012. Individuals who were found to have Leishmania infection by any of the tests were referred for clinical assessment and medical assistance, if necessary, under the care of the Department of Infectious Diseases at the HUPES.
Results
Characteristics of the studied area
Figure 1 shows a representative map of the area with the distribution of studied houses (red dots). Figure 2 demonstrates the flowchart of which results were obtained from selected households and individuals by serology, LST, and clinical examination to identify suspected cases of VL. Among the 94 households randomly selected, 2 were excluded as residents of those households could not be enrolled.
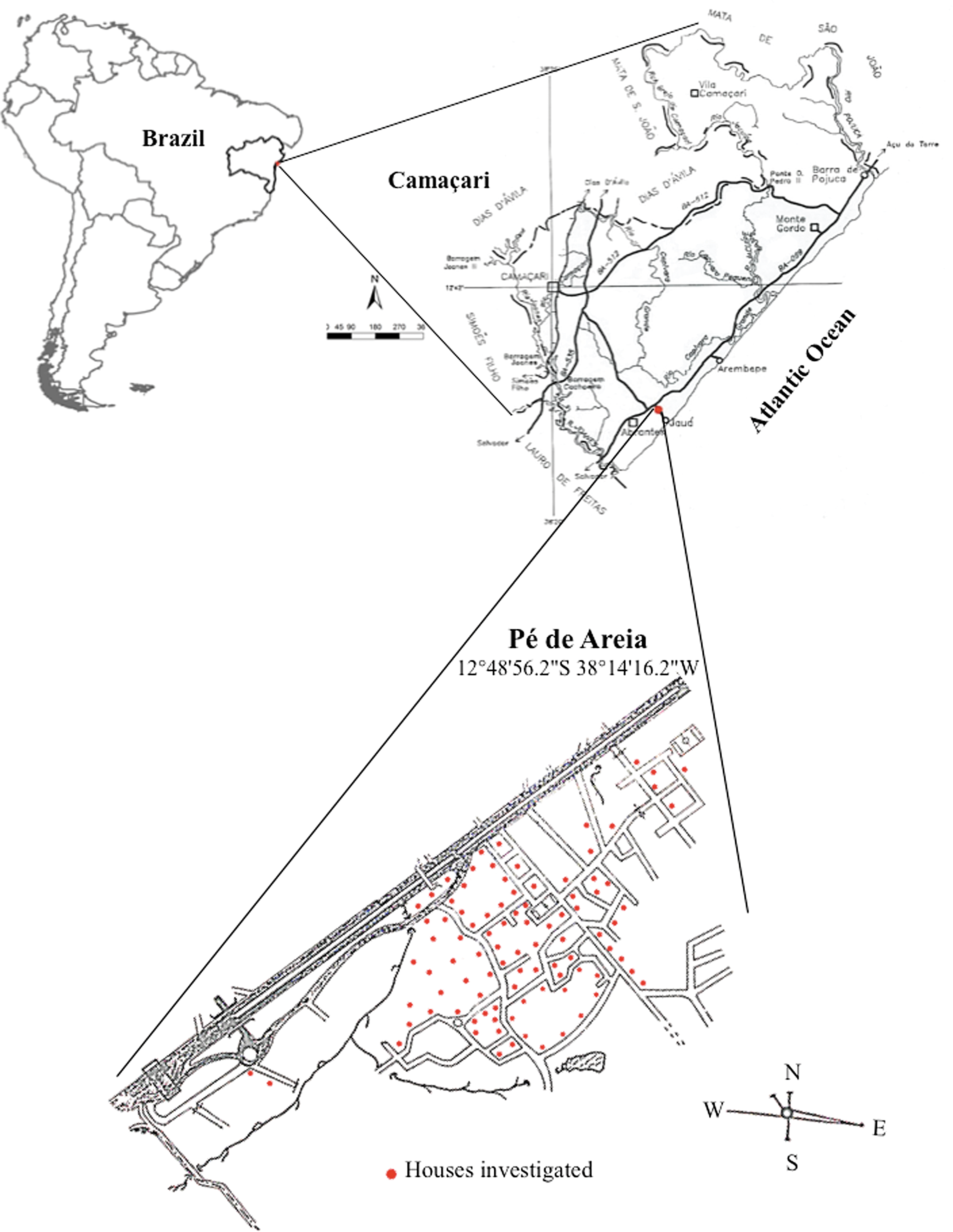
Map of Pé de Areia, village in the Municipality of Camaçari, Bahia, Brazil. This figure illustrates the geographic localization of the studied area of Pé de Areia within the State of Bahia, Brazil. The red dots represent the houses that were studied. The exact latitude and longitude of the village Pé de Areia are shown on the side of the map. Note: Scale: 1/100,000. Source: Funasa.
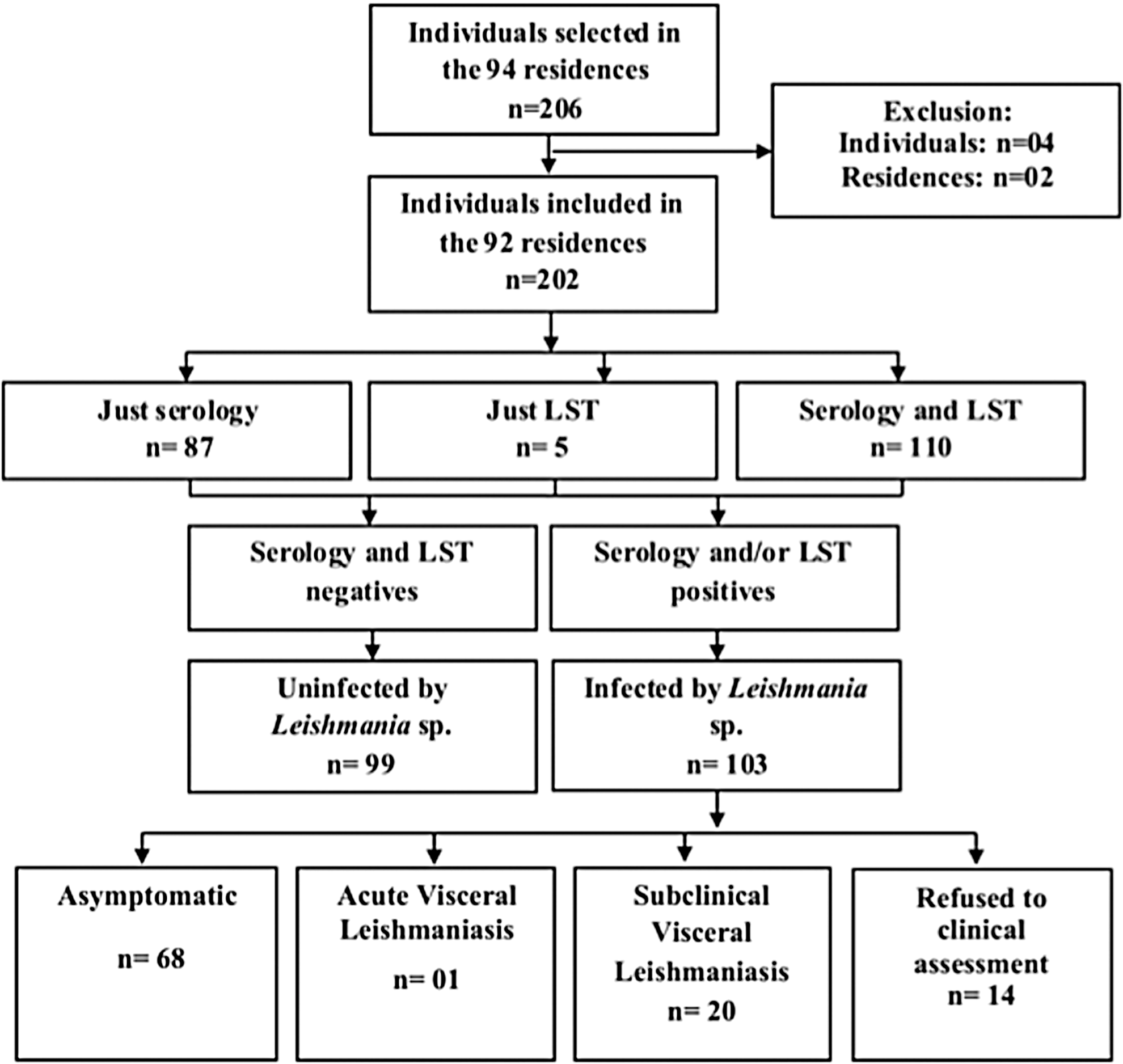
Flowchart of enrolled individuals, testing results, and clinical status of the study population in Pé de Areia, Camaçari, Bahia, Brazil. This figure depicts a flow diagram of the number of households and individuals screened and selected for the study. The first box demonstrates the numbers of screened households and individuals within those households. Next, the number of included and excluded households is shown. Within the included individuals, the next set of boxes depicts the number of individuals who were positive by serology and/or leishmanin (LST) test and the classification of enrolled individuals by these results. The bottom level of boxes demonstrates the clinical classification of the individuals who were diagnosed with visceral leishmaniasis after clinical and physical evaluation. LST, leishmanin skin test.
Clinical and epidemiological data of study population
The total studied population was 202 individuals. Among the 92 houses included in the study, the prevalence of Leishmania infection detected by positive serology was 91/197 (46.2%; 95% CI: 0.3937–0.5316) and by LST positivity was 29/114 (25.4%; 95% CI: 0.1834–0.3414) individuals. Individuals positive for antibodies to both rK39 and rK26 included 64/197 (32.5%; 95% CI: 0.2634–0.3931; Fig. 2). Five patients refused to have blood drawn, and 88 did not allow the LST. Serological testing found 76/197 (38.6%; 95% CI: 0.3206–0.4553) reacted to rK39 antigen and 79/197 (40.1%; 95% CI: 0.3351–0.4707) individuals reacted to rK26 (Fig. 3). The analysis of concordance between rK39 and rK26 antigens found good agreement (kappa = 0.713 and PABAk = 0.726) between the results. Hepatomegaly was detected in 20 individuals and splenomegaly in one. Among the 103 individuals in whom we could establish a diagnosis of leishmaniasis, acute VL was established in one (1%), subclinical VL in 20 (22.5%), and asymptomatic Leishmania infection in 68 (76.4%) individuals (after an average of 6 months of monitoring). We could not establish a clinical diagnosis in 14 individuals who tested positive by serological or skin testing because they refused to come to the hospital for clinical and laboratory evaluation. The patient with acute VL was treated with pentavalent antimony. Among the individuals diagnosed with subclinical infection (i.e., evidence of visceromegaly but no symptoms), all were considered to have self-healed at the 6-month follow-up visit due to disappearance of the visceromegaly and no new symptoms detected.
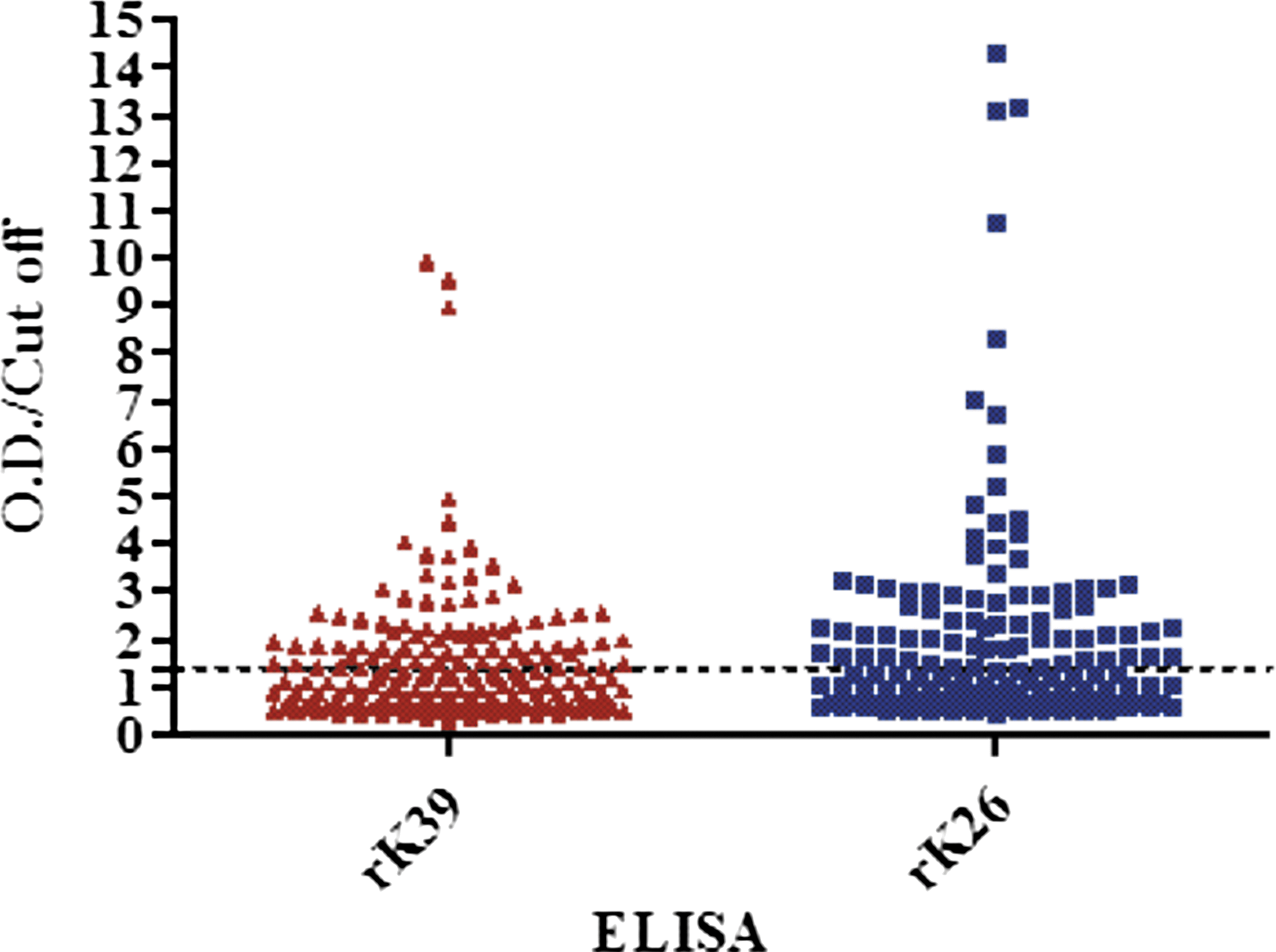
Ratio between OD and cutoff for ELISA-rK39 and -rK26 in individuals living in Pé de Areia, Bahia, Brazil. This figure presents the ratio of OD cutoff for ELISAs using the rK39 and rK26 antigens in subjects. The markers above the dotted line are considered seropositive with an OD/cutoff ≥1.4, and those below the line were considered seronegative with an OD/cutoff <1.4. OD, optical density of individuals.
Bivariate analysis of risk factors associated with human Leishmania infection in the studied area
Table 1 shows all variables that were analyzed in association with Leishmania infection, including demographic data, domiciliary presence of a potential animal reservoir, type of house/yard, and use of sand fly repellents. There was no association of Leishmania infection with specific age group (p = 0.36), but infections trended to be more prevalent in males: 42/76 (55%; prevalence ratio [PR] = 0.77, p = 0.09). The presence of a pet at home was not significantly associated with an increased risk of Leishmania infection (PR = 1.24, p = 0.28). The use of any repellent methods (daily or home insecticide spraying and use of bed nets) was also not associated with protection (PR = 1.01, p = 1.0). Interestingly, comparing houses with and without sand backyards, we found that those with a sand backyard were protected from Leishmania infection (PR = 1.24, p = 0.049).
Chi-square test was chosen for comparison of proportions when at least four observations were present for each category, and Fisher's exact test was used in other situations. Mann–Whitney test was used to compare medians between groups.
Chi-square test.
Mann–Whitney test.
Fisher's exact test.
Poisson regression multivariate analysis for risks associated with Leishmania infection
Results of the three multilevel models constructed to analyze the association between infected individuals and possible risk factors for infection are summarized in Table 2. The type of backyard was associated with 35.2% of the variance for infected individuals among the studied houses. The presence of a sand backyard remained a protective factor against Leishmania infection in the multivariate analysis (PR = 0.61, 95% CI: 0.41–0.90). The presence of a cat or dog at home, independent of type of backyard, was not a risk factor for Leishmania infection (dog: PR = 1.14, 95% CI: 0.80–1.64; and cat: PR = 1.19, 95% CI: 0.78–1.81). Given that the presence of backyard could be a confounding variable, we performed a stratified analysis to correct for this effect. As a result, we identified areas with a high prevalence of infected individuals (clustering) in households without a backyard (Fig. 4). We observed this cluster effect in six of the eight households with infected individuals but without a backyard.
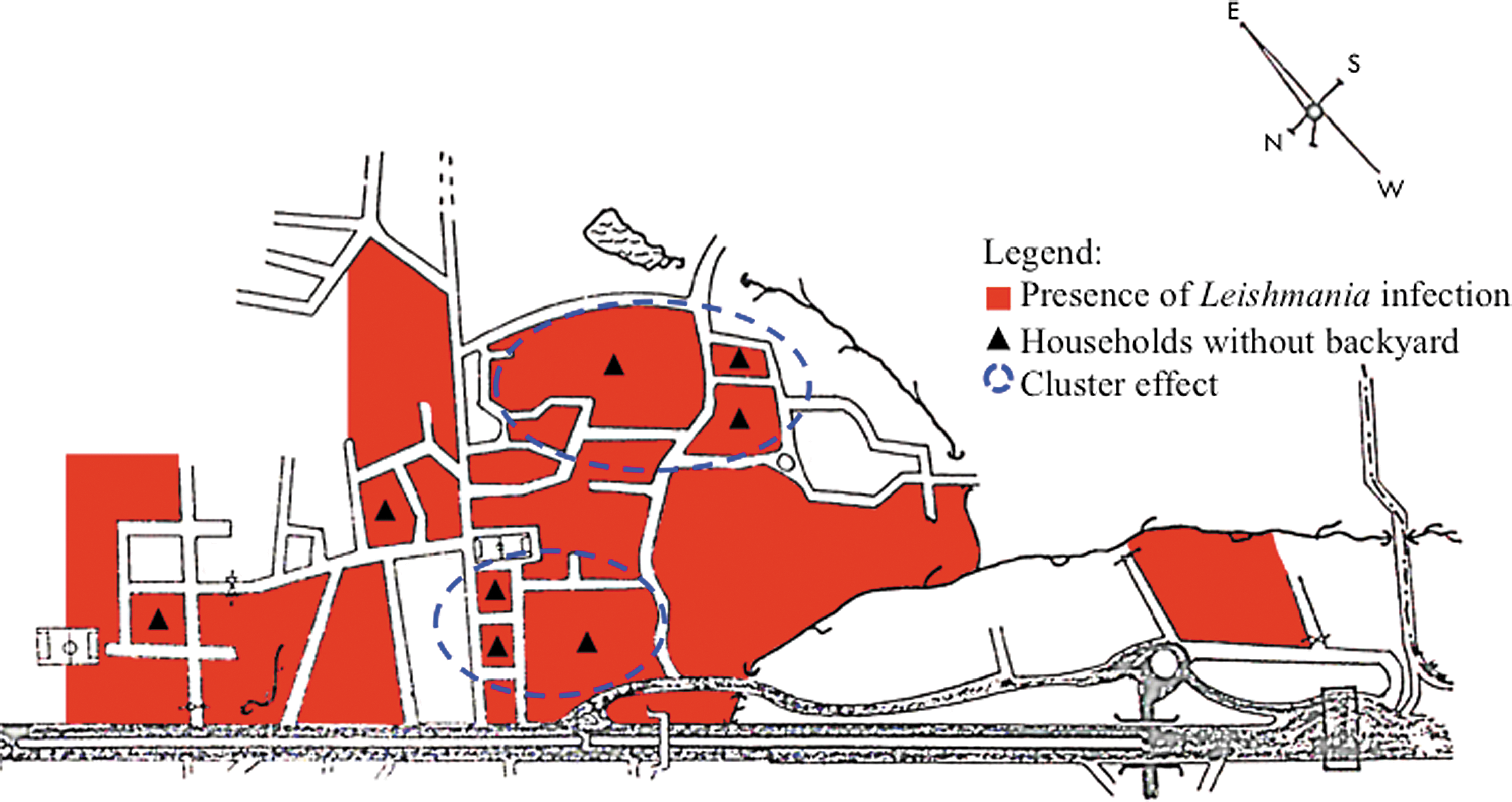
Presence of Leishmania infection in households without backyard and cluster effect in Pé de Areia, Bahia, Brazil. This figure represents areas where Leishmania infection was identified (red) within the study area. We identified two clusters of cases corresponding to houses without a backyard. The black line is the paved road BA099.
AIC, Akaike information criterion; CI, confidence interval; ICC, intraclass correlation coefficient; PR, prevalence ratio.
Discussion
The increase of VL in urban areas in Brazil has become a major challenge for the control of this zoonotic disease. In this prospective study, we analyzed the risk factors associated with Leishmania infection in a vicinal area of the village of Monte Gordo, in which we had previously reported a new ecological niche of the transmission of L. infantum (Cunha et al. 1995). Over the past 25 years, the VL epidemic was expanded into new areas in this municipality. The area under study, Pé de Areia, has the same ecological characteristics as the previously reported area of Monte Gordo in Bahia, a typical Atlantic deforested region located 1–2 km from the ocean. Settlement in this area began in the 1930s during the construction of the airport in the Municipality of Camaçari, Bahia. This area developed rapidly with migration of populations from the capital city of the Bahia State and other nearby municipalities. Urbanization of these villages, through increases in population density, has occurred since 1960, as shown in Figure 1. Our examination of this area revealed that 30% of the population was LST positive and 14% was seropositive. This seropositivity rate was three times higher (46%) than that reported in Monte Gordo, while the rate of positive LST was slightly less (25%) than that reported in Monte Gordo. A possible explanation for this discrepancy in rates is that we have detected Leishmania infection earlier in Pé de Area than in Monte Gordo. These results also highlight the importance of screening for infection using both serological and cell-mediated immunity approaches. Finally, these high rates of subclinical and asymptomatic infections are consistent with previous reports from Bahia (subclinical infection 60% in Jacobina, Bahia vs. 22.5% in Pé de Areia; asymptomatic cases 20% vs. 76%, respectively; Badaro et al. 1986).
Several studies have been performed to identify the risk factors associated with the rates of Leishmania infection and disease in many endemic areas in the world. In the first prospective study performed in Bahia, age and nutritional status were strongly correlated with progression to the classic VL disease (Cerf et al. 1987). Also in this area, the dog was found to be the main reservoir host of L. infantum (Ashford et al. 1998). In a meta-analysis of 51 studies, investigators found that the presence of dogs in the household was positively associated with VL (Belo et al. 2013). Cats have also been demonstrated to be infected with L. infantum in Italy (Maroli et al. 2007). In a meta-analysis published by Quinnell and Courtney (2009), none of the other accidentally infected animals were found to be important reservoirs of Leishmania infection. In our study, we did not find an association between the presence of dogs or other pets and the presence of infected individuals in the studied houses. In our study, we could not analyze either gender or socioeconomic status as risk factors because most included persons were women and children. This limitation was likely due to the fact that we could only include individuals who were physically present in the house during the survey. The limited number of households in this study may have limited our ability to identify the risk associated with having one of these pets. Interestingly, individuals without a backyard were at higher risk, suggesting that having backyard may protect the house from having indoor sand flies. This is somewhat in contrast to the work of others that has shown that the presence of trees within a 10-m radius of a home is associated with higher rates of infection (Caldas et al. 2002). Finally, impregnated bed nets, curtains, and spraying interior walls of houses are recommended control measures to avoid Leishmania infections (Ready 2014). In our study, the presence of bed nets was not associated with protection, possibly because the bed nets were not impregnated with insecticide as demonstrated elsewhere (Gonzalez et al. 2015).
Early diagnosis and complete treatment are essential for the management of VL as treatment delay can adversely affect prognosis (Chappuis et al. 2007, de Araujo et al. 2012). The major goals of this study were to actively detect recently infected individuals in the area and provide treatment. In our study, we found that none of the individuals with subclinical infection progressed to the complete VL. All became asymptomatic and were considered self-healing similar to what we have described in other areas previously (Badaro et al. 1986).
Conclusions
We conclude that in newly discovered areas where transmission of L. infantum to humans is seen, periodic surveys of Leishmania infection in the exposed population may discover high rates of infection. As demonstrated in this study, use of serology and skin testing to identify cases of acute and subclinical infections early will allow more accurate monitoring, will lead to less complicated treatment in local health units, and thus have a significant impact on the morbidity and mortality of VL. In addition, careful investigation of the risk factors associated with leishmaniasis by periodic surveys may be helpful in optimizing prevention guidelines.
Footnotes
Acknowledgments
The team was assisted by Marcos Nogueira and his team from the Department of Epidemiological Surveillance Camaçari-BA, Steps Sandra and her team at the Center for Zoonosis Control Camaçari-BA, the staff at the Health of the town of Pé de Areia-BA, the staff at the Health Jauá-BA, Steve Reed, Edgar Marcelino Carvalho, Andrea Santos Magalhães, the Immunology Service/HUPES, and Maria Nakatani (Laboratory of Tropical Medicine/HUPES). Financial support: this work was supported by the Fundação de Amparo à Pesquisa do Estado da Bahia (FAPESB).
Author Disclosure Statement
No competing financial interests exist. The Ethical Committee of University Hospital Professor Edgard Santos, Federal University of Bahia, Brazil, approved the study.