
Abstract
Infections of humans with the tick-borne Crimean–Congo hemorrhagic fever virus (CCHFV) can cause a severe hemorrhagic fever with case fatality rates of up to 80%. Most humans are infected by tick bite, crushing infected ticks by hand or by unprotected contact with blood of viremic mammals. Next to the notified human CCHF cases, the real distribution and the situation in animals in Southeastern Europe are nearly unknown. Since domestic ruminants play a crucial role in the life cycle of the vector ticks and the transmission and amplification of the virus, the antibody prevalence in those animals is a good indicator for the presence of CCHFV in a region. Therefore, the prevalence of CCHFV-specific antibodies was investigated in domestic ruminants of different regions of Bulgaria and Turkey. Sera of 1165 ruminants were tested and a prevalence of up to 90% was identified. The overall prevalence for Bulgaria was 26% and for Turkey 57%. The results highlight the risk of human infections in those regions and the importance of the investigation of the prevalence in animals for identification of risk areas. This article provides a unique overview about published CCHFV antibody prevalence in animals in comparison to human incidences in different areas of Bulgaria and Turkey. Although it will help to complete the understanding of the CCHFV situation in these countries, it also demonstrates the lack of unpublished and published data even in these highly endemic areas.
Introduction
C
In Bulgaria, 1447 human CCHF cases were reported between 1953 and 2012 (Edinakova et al. 2013), while in Turkey even 9069 human CCHF cases were notified from 2002 to 2014 (Public Health Agency of Turkey 2015). In contrast, information about infections in animals is very limited. For Bulgaria, a study carried out in 1968 revealed high prevalence of CCHFV-specific antibodies in animals in the endemic area, and a study from 2011 found an overall antibody prevalence of 72% in cattle and sheep in the Burgas province (Hoogstraal 1979, Barthel et al. 2014). Summarizing the three published studies targeting animals in Turkey, high prevalence has been reported from all nine investigated provinces (Balikesir, Bilecik, Bursa, Elazig, Samsun, Sinop, Sivas, Tokat, and Yozgat) among the 81 provinces of Turkey (Kirbas et al. 2010, Albayrak et al. 2012, Tuncer et al. 2014).
The aim of our studies was to increase the knowledge about the distribution of CCHFV in Bulgaria and Turkey by summarizing and confirming previously published data and by testing animals of regions with unknown CCHFV status.
Materials and Methods
Serum samples from 497 sheep and cattle from seven provinces of Turkey were collected in 2011, and 619 sera from sheep, goats, and cattle from 11 provinces of Bulgaria were collected in 2011 and 2014. In addition, 49 sera collected from sheep from the Burgas province in Bulgaria in 1974 were included in this study. All sera were collected from animals older than 18 months, which were grazing frequently on common pastures. According to their ear tags, all animals were born in the same location where they were sampled. In Turkey, sampling was carried out randomly at district level. In Eskisehir and Corum, the samples were collected from ruminants from animal markets, but those animals were born in the same province (according to their ear tags). In Bulgaria, samples were collected in general in regions where the disease is established.
Serum samples were screened by species specific in-house enzyme-linked immunosorbent assays (ELISAs) for CCHFV-specific IgG antibodies. The ELISAs are based on the recombinant Nucleocapsid (N-) protein of CCHFV strain Kosovo Hoti. Detailed protocols and validation data for all assays have been published previously (Mertens et al. 2015, Schuster et al. 2016). All samples, which were positive or inconclusive in the in-house ELISA, were tested in a commercial ELISA (Vector-Best). This ELISA bases on inactivated CCHFV (strain from Uzbekistan) and was originally designed for testing sera from humans. The test was adapted and validated for the investigation of serum samples from ruminants (Mertens et al. 2015, Schuster et al. 2016). In case the result of the in-house ELISA was not confirmed by the commercial ELISA, the respective sample was tested in a commercial immunofluorescence assay (IFA) as second confirmation assay (Euroimmun). The IFA detects the reaction of specific antibodies with the Glycoprotein C or the N-protein expressed by transfected eukaryotic cells. This IFA, produced for human serum samples, was adapted for testing sera from cattle, sheep, and goats (Mertens et al. 2015, Schuster et al. 2016). The result of the IFA in combination with the previous results leads to the final result. In general, a sample was defined as positive if the result of two of the assays was positive; a sample was declared as negative if the screening ELISA was negative (Mertens et al. 2009).
In the seroepidemiological studies, the prevalence was calculated with a confidence interval (CI) of 95%. The comparison of prevalence was based on the Fisher Exact Test. A p-value lower than 0.05 (p < 0.05; 95% CI) has been adjusted as statistically relevant.
Results
Results for Bulgaria demonstrate high CCHFV seroprevalence for animals from the southern provinces (Blagoevgrad 38%, Haskovo 34%, Yambol 24%, Sliven 57%, and Burgas 50%), whereas in the central and northern provinces, a low prevalence (Plovdiv 5% and Gabrovo 13%) or no CCHFV-specific antibodies (Montana, Lovetch, Shumen, Dobritch all 0%) were found in animals (Table 1 and Fig. 1). Testing of sheep serum samples from Burgas (Akhtopol municipality) collected in 1974 revealed a prevalence of 86% (95% CI 73–94%).
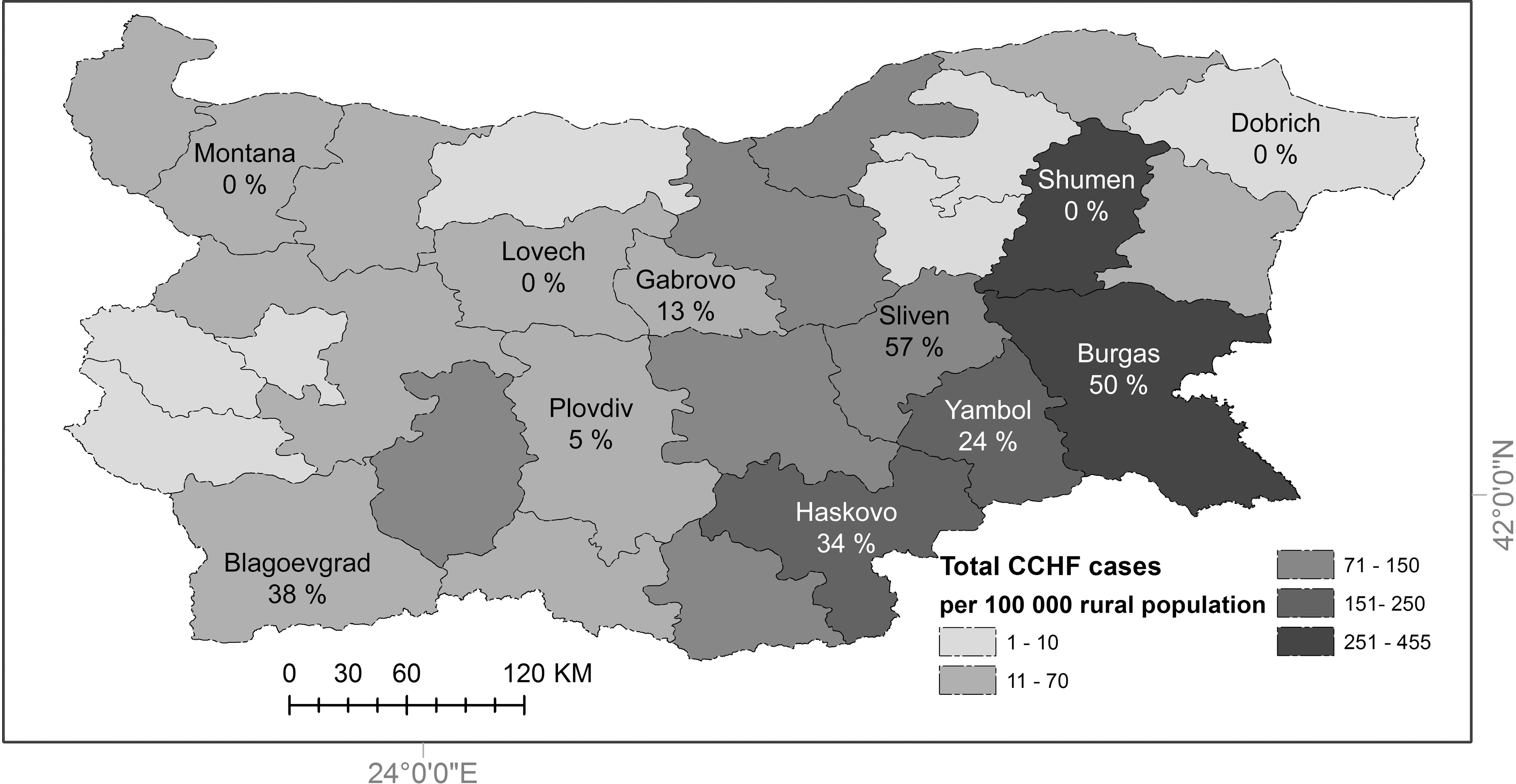
Distribution of CCHFV in provinces of Bulgaria. Province names with prevalence: CCHFV-specific antibodies in sheep, goat, and cattle (%, present study); shaded provinces: human CCHF cases per 100,000 rural inhabitants between 1953 and 2012 (Edinakova et al. 2013). CCHFV, Crimean–Congo hemorrhagic fever virus.
95% confidence intervals shown in brackets.
Results for Turkey demonstrate high CCHFV seroprevalence for animals from the central northern provinces (Corum 43%, Karabük 68%, Kastamonu 17%, Tokat 87%, and Yozgat 85%), whereas in the western (Eskisehir) and eastern (Erzurum) province, no CCHFV-specific antibodies were found in the animals (Table 2 and Fig. 2).
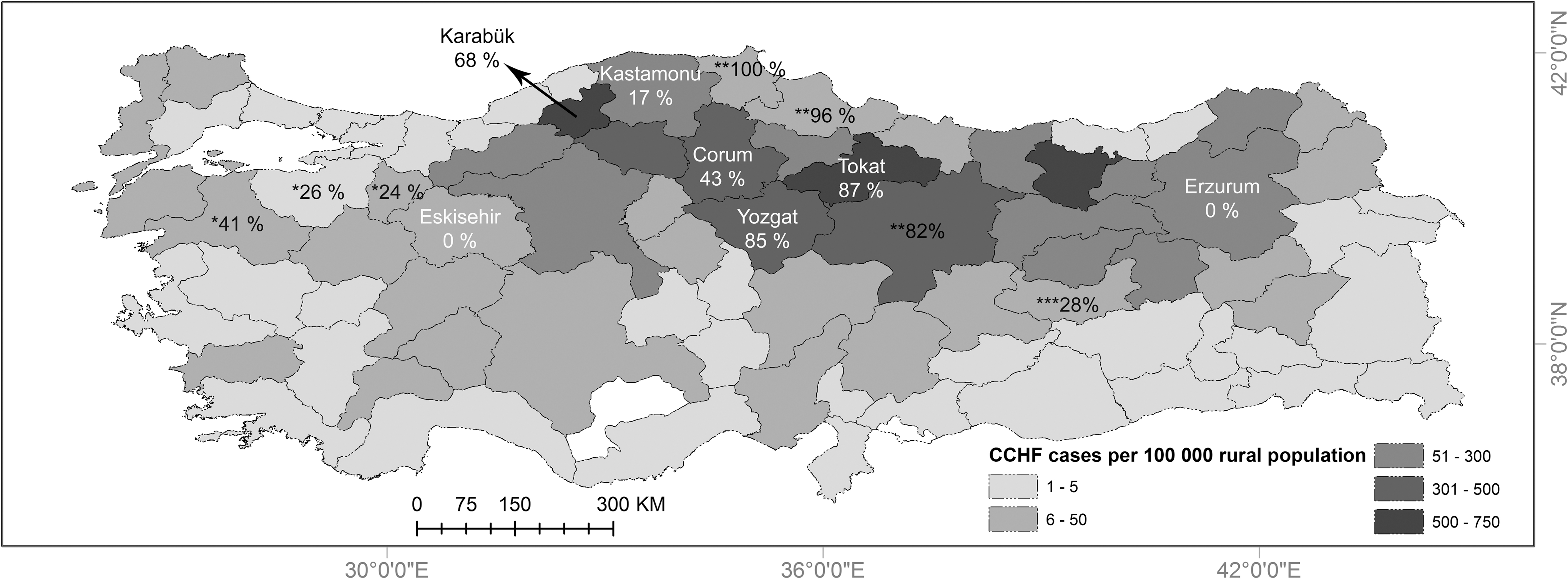
Distribution of CCHFV in provinces of Turkey. Province names with prevalence: CCHFV-specific antibodies in sheep and cattle (%, present study); *prevalence in sheep, goat, and cattle (Tuncer et al. 2014); **prevalence in sheep and goat (Albayrak et al. 2012); ***prevalence in sheep and cattle (Kirbas et al. 2010); shaded provinces: human CCHF cases per 100,000 rural inhabitants between 2002 and 2014 (Public Health Agency of Turkey 2015).
95% confidence intervals shown in brackets.
CT, cattle; GO, goat; n, no. of samples; SH, sheep.
Discussion
The results of the study in Bulgaria correlate well with the notification of human CCHF cases in the respective regions (Avsic-Zupanc 2007, Vescio et al. 2012, Christova et al. 2013, Edinakova et al. 2013). Burgas and Sliven have reported high CCHF case numbers, whereas only sporadic human cases were reported from the provinces where no specific antibodies in the animal population were detected (Fig. 1). In Blagoevgrad, the number of human CCHF cases increased from time period 1998–2005 to 2008–2011 (Avsic-Zupanc 2007, Christova et al. 2013), which is reflected by the high seroprevalence in ruminants (38%). This might be an indication that a new high risk area is established and it should be an alert sign for authorities. In contrast, no animal was positive for CCHFV-specific antibodies in Shumen, which is in line with the information that nearly all cases of this region were reported around 60 years ago during the outbreak in 1954/1955 (Edinakova et al. 2013). The prevalence in the sheep population from Burgas was significantly higher (p < 0.05) in 1974 (86%) compared to 2014 (60%). This might be an artifact of sampling (two localities only sampled in 1974), but it highlights the CCHF risk for humans in this long lasting endemic area. Summarizing the results of the present study and those from literature, the high risk area for CCHFV infections seems to be the south, especially the southeastern part of Bulgaria.
The results of the present study for Turkey confirm previous studies and underline the high risk of CCHFV infections in the provinces of central Anatolia. CCHFV-specific antibodies were found in the tested animal population of five out of seven investigated provinces. The prevalence reached from 17% (Kastamonu) to 87% (Tokat) (p < 0.05). No animal was tested positive for CCHFV-specific antibodies in the western province Eskisehir and the eastern province Erzurum. In Eskisehir, it might be a sampling artifact resulting from the low number of samples (Table 2). Anyhow, especially for Erzurum, it seems to be surprising since Erzurum is one of the provinces with the highest number of human CCHF cases in the last years (Yagci-Caglayik et al. 2014). The answer can be found in the location of sampling. Erzurum consists of 20 districts. CCHF is reported only from eight districts in the north of the province and only three of those districts (Oltu, Senkaya, and Olur) are known to have high CCHF prevalence among humans. Other districts do not have suitable habitats for permanent H. marginatum populations. The sera of the present study were collected from central districts where no human CCHF cases were reported and also not expected. Therefore, the result reported in this study is not surprising. A similar observation was made in a seroprevalence study in the human population of Erzurum, which resulted in a very low prevalence (1.3%). The authors explained as well that the samples were collected in the center of the province, whereas the human cases were reported in the north of Erzurum (Yagci-Caglayik et al. 2014). Anyhow, this underlines the impact of the location of a prevalence study on its result and the influence of geographical factors on the infection rate, which might also be the reason for the differences in the prevalence found by previous publications for Tokat and Yozgat in Turkey and Burgas in Bulgaria compared to the present studies (Table 2; Barthel et al. 2014).
In all provinces where CCHFV-specific antibodies were detected in the animal population, higher numbers of human CCHF cases were notified (Public Health Agency of Turkey 2015). These data are in line with previously published data (Table 2 and Fig. 2) and demonstrate that complete north and central Turkey can be classified as a risk area for CCHFV infections. Turkish health authorities were very successful in informing and sensitizing the local population and healthcare workers about CCHFV associated risks. However, the CCHF case number has not decreased to the expected level yet, while lethality rates remain stable at around 5%. Although it seems that we can hardly protect people like farmers from CCHFV infections due to infection routes by tick bite or animal contact, we can increase the general awareness and, thereby, the chance to survive the infection by fast and precise treatment and care.
Conclusion
The comparison of the numbers of human CCHF cases and the prevalence of CCHFV-specific antibodies in domestic ruminants of the respective provinces highlight the importance of seroepidemiological investigations of animals for the identification of CCHFV risk areas. High prevalence in animals should alert the authorities to inform the medical staff and the general population on the risk and the key facts of CCHFV. Anyhow, focusing on Bulgaria and Turkey at large, the summary of the CCHFV situation in humans, as well as in animals, demonstrates a lack of knowledge. There are still regions with unknown status. Public Health authorities, medical doctors, and hospital staff should be aware of CCHF risks, and further investigations should be carried out especially in the northern provinces of Bulgaria and the southern provinces of Turkey. The endemic areas of Bulgaria and Turkey are best characterized worldwide, but the whole infection cycle especially if leading to an endemic situation is still not understood.
Footnotes
Acknowledgments
This study was funded by EU grant FP7-261504 EDENext (
Author Disclosure Statement
No competing financial interests exist.