
Abstract
Introduction:
Scrub typhus is a major reason for febrile illness, caused by a bacterium Orientia tsutsugamushi, a rickettsial pathogen. Few outbreaks of scrub typhus have been reported from Arunachal Pradesh in recent past. However, there is lack of seroprevalence data from the region. In this regard, this study was undertaken using archival serum sample available from seven districts of Arunachal Pradesh.
Methodology:
This serological study was conducted in Regional Medical Research Center for NE Region, Dibrugarh. Reactivity to IgG class of antibodies against scrub typhus was done using Scrub typhus detect IgG ELISA kit as per manufacturer's protocol.
Result:
Seroprevalence of scrub typhus in seven districts of Arunachal Pradesh was found to be 40% (120/300). The age-specific scrub typhus seroprevalence rose steadily from 5.6% in children <10 years of age to 61.8% in persons aged ≥40 years (p = 0.0001). Prevalence is lowest in Papumpare (25.9%) and highest in East Siang (72.5%) (p = 0.0001). The seroprevalence in males and females was very similar, however, the female prevalence increases from age group ≥30 years (p = 0.053). Moreover, among the farmers, the seroprevalence is higher (58.3%) (p = 0.0001).
Conclusions:
As clinical symptoms overlap with other viral/bacterial infections, scrub typhus infection should be considered in differential diagnosis of any acute febrile illness in this part of the country. In view of the high prevalence, empirical therapy of doxycycline/azithromycin may be done in cases of undiagnosed fever. Active surveillance has to be done to understand exact magnitude, epidemiological aspects, and distribution of vector and disease of this reemerging neglected tropical disease.
Introduction
S
During World War II, scrub typhus is known to have broken out in epidemic form among the military troops in northeastern states of India, especially on the India–Burma border (Tattersall 1945). Moreover, outbreaks of scrub typhus have been reported from Arunachal Pradesh and northeast India (Khan et al. 2012, Borkakoty et al. 2016), however, the actual population incidence is not known. Seroprevalence data across the state will help to determine exposure to O. tsutsugamushi and suggest areas of likely high incidence. Furthermore, seasonal outbreak of fever is being reported at a regular interval from different regions of Arunachal Pradesh, at times the disease remains undiagnosed or underdiagnosed. In this regard, this study was undertaken to provide first-hand information on the serological evidence of scrub typhus in Arunachal Pradesh. Population-based serologic surveillance provides important data on prevalence and risk factors of susceptible disease in a particular region and to evaluate health programs to overcome future outbreaks. Sera can be collected from a randomly selected population-based sample. However, this technique requires trained technicians to visit participants to collect serum sample, which is expensive and time-consuming. The use of residual/archival serum banks overcomes many of these problems.
Methodology
Ethics statement
This study was approved by the Institutional Ethics Committee of Regional Medical Research Center (RMRC), for NE Region, Dibrugarh. Consent for future use of the archival samples was taken during the earlier conducted studies, as well as informed consent was obtained from health workers from Dibrugarh district (urban area) of Assam (an adjoining state of Arunachal Pradesh). The health workers included in the study neither had any travel history to O. tsutsugamushi endemic area nor ever diagnosed with scrub typhus.
IgG ELISA and statistical analysis
Serum samples collected from apparently healthy individuals for hepatitis B virus screening from community, conducted in various parts of Arunachal Pradesh during the period 2009–2013, were selected for this study. A total of 2975 serum samples were available from seven districts of Arunachal Pradesh (Fig. 1), belonging to the age group of 2–80 years, of which ∼10% serum samples (300) were selected. Randomization of the sample was performed using random number generation in OpenEpi (online software), after which a systematic sampling (every 10th) was done beginning from the random number as the first sample. Among seven districts, in two districts (East Kameng and West Siang) the numbers of available archived samples were less than 300, as such, the representations from those two districts were less. The serum samples were tested for reactivity to IgG class of antibodies against scrub typhus using the Scrub typhus detect IgG ELISA kit (InBios International, Inc.) as per manufacturer's protocol. Confidence intervals (CIs) at 95% were estimated using the exact binary method (Korn and Graubard 1998). Statistical association was evaluated using Pearson's chi-squared test. The level of statistical significance was kept at p≤0.05. Analysis was performed by using statistical software SPSS 20.0 (trial version) and MedCalc version 9.3.9.0 (trial version).
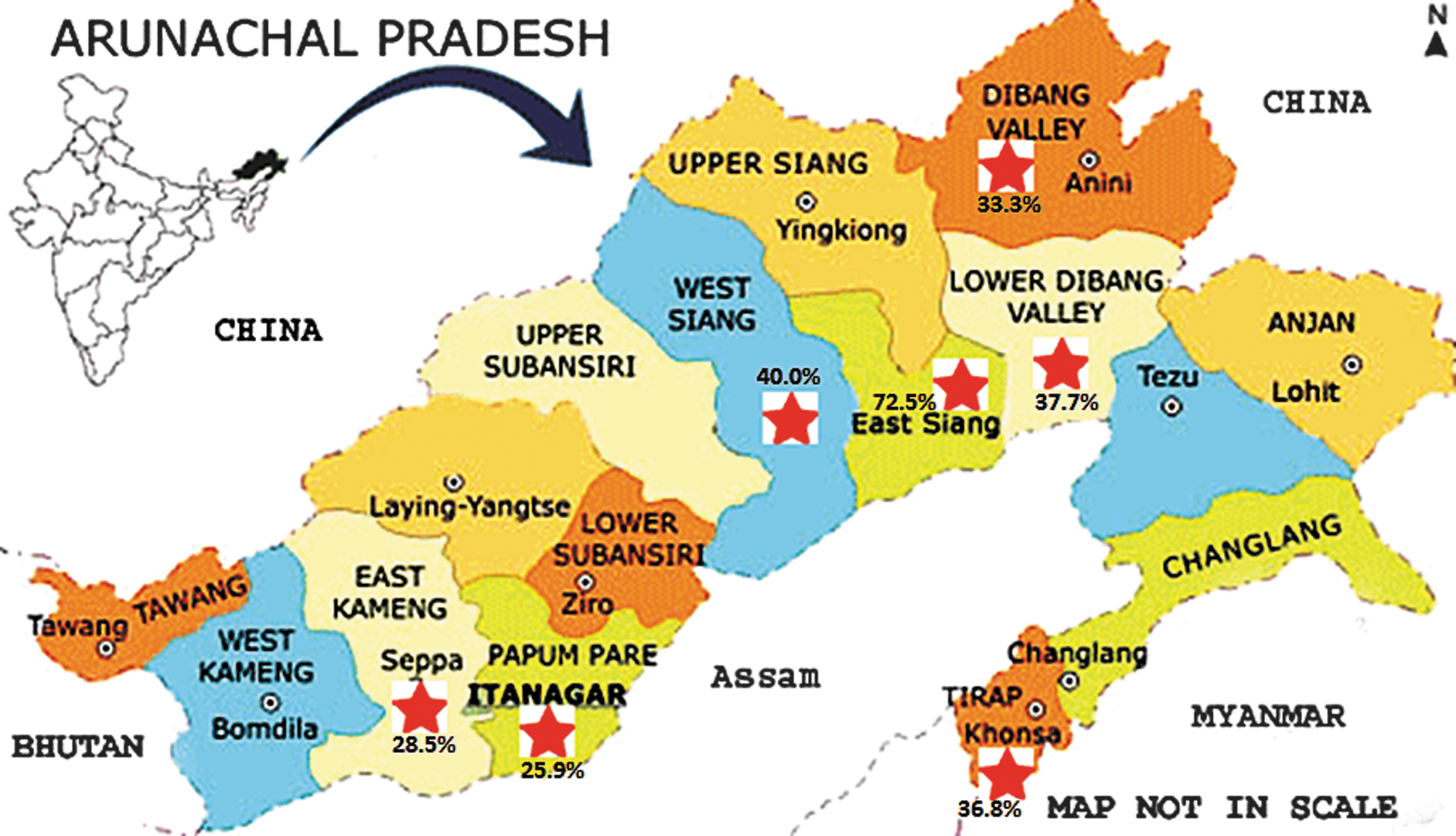
Map of Arunachal Pradesh showing the study districts along with the prevalence (%) in the respective districts. Red star symbol is showing the study districts. Color images available online at
Results
The overall seroprevalence of scrub typhus in seven districts of Arunachal Pradesh was found to be 40.3% (121/300; 95% CI: 34.9–46.1). All the 34 samples collected from health workers in Dibrugarh, Assam, were found nonreactive against scrub typhus IgG. The assay was also repeated with 10% of the randomly selected tested 300 samples (reactive and nonreactive) to check the reproducibility, which showed 100% concordance. The main characteristics of the samples from seven districts of Arunachal Pradesh are described in Table 1. The age-specific scrub typhus seroprevalence estimates are shown in Figure 2. The overall prevalence in this study rose steadily from 5.6% in children <10 years of age to 26.7%, 36.1%, 56.7%, and 61.8% in persons aged 10–19, 20–29, 30–39, and ≥40 years, respectively (p = 0.0001). The prevalence was lowest in Papumpare (25.9%) and highest in East Siang (72.5%) (p = 0.0001). The seroprevalence in males and females was very similar in the age group <30 years, however, the prevalence among female increases from the age group ≥30 years compared to males and approaching significance (p = 0.053).
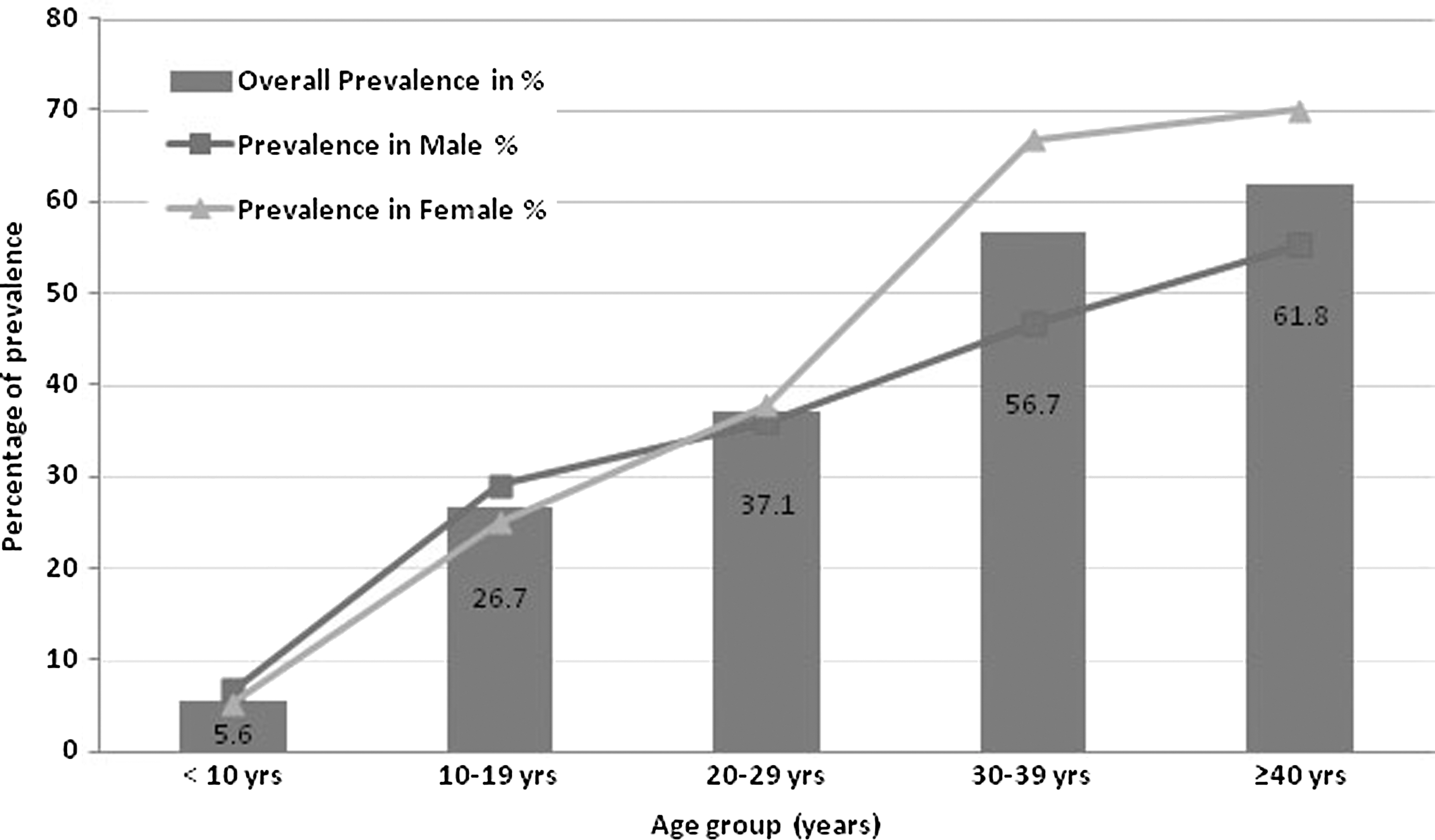
Comparison of age-specific scrub typhus seroprevalence estimates in seven districts of Arunachal Pradesh.
Point seroprevalence estimates are shown with their 95% confidence intervals along with p value calculated against total sample size (300).
EK, East Kameng; ES, East Siang; LDV, Lower Dibang Valley; PPR, Papumpare; TRP, Tirap; UDV, Upper Dibang Valley; WS, West Siang; 95% CI, confidence interval proportion at 95% confidence level.
Discussion
To our knowledge, this is the first report of population-based seroprevalence study of past exposure to O. tsutsugamushi from Arunachal Pradesh. In this region, Jhum cultivation is still practiced, and after clearing the jungles, it becomes ideal for scrub vegetation. This may be the major cause for the predominance of scrub typhus in these regions. Interestingly, the incidence among pediatric age group (<15 years) was also observed, which may be partly explained by an increased exposure opportunity for this age group during playing or while being carried on their mother's back during work in those areas. Again, it was observed that the prevalence of scrub typhus in female starts increasing from the age of 30 years onward compared to males. This might signify increase in exposure of females to scrub vectors during harvesting or cultivation where females usually work in the fields. Moreover, persistence of antibodies over time tends to remain at higher levels in females compared to males, as seen in postvaccination study with hepatitis A (Garuz et al. 1997).
Similarly, in scrub typhus infection also, females may have persistence of detectable IgG titer for a longer duration than males. In the recent past, scrub typhus has been reported from 16 different states (Jammu & Kashmir, Himachal Pradesh, Rajasthan, Haryana, Maharashtra, Karnataka, Andhra Pradesh, Kerala, Tamil Nadu, Pondicherry, West Bengal, Sikkim, Uttaranchal, Assam, Arunachal Pradesh, and Nagaland) in India (Boorugu et al. 2010, Saifudheen et al. 2012). The prevalence of scrub typhus among the blood donors from Malaysia and south India (Vellore) was reported to be 5.4% and 15%, respectively (Tay et al. 2003, Sengupta et al. 2015). In this study, we observed a cumulative ∼40% prevalence of scrub typhus in seven districts of Arunachal Pradesh. It is higher than the study conducted among the healthy adults in Vientiane city (20.3%) (Vallee et al. 2010) and healthy farmers in Tianjin (39.8%) (Zhang et al. 2011). In 2012, a team of scientists from RMRC, Dibrugarh, went to East Siang district of Arunachal Pradesh to conduct a detailed investigation in a suspected outbreak of Dengue, however, only four patients tested positive for dengue virus and 40 were positive for scrub typhus out of 118 samples collected (
In the present study, we recorded an alarmingly high prevalence of past exposure to O. tsutsugamushi among people living in Arunachal Pradesh. This retrospective study, had limitation to elucidate the exact cause for this high prevalence. However, scrub typhus prevalence was found to be higher among the farmers (58.3%, p = 0.0001), which may be associated with the occupational exposure to the scrub vegetation. Scrub typhus infection is reemerging and leads to significant morbidity and mortality of up to 30%, if undiagnosed and proper treatment is not done at the appropriate time (Wang et al. 2007, Rathi and Rathi 2010). In developing countries, it constitutes a very significant, however, often undiagnosed portion of the febrile disease contributing to financial burden on many populations (WHO 1993). As O. tsutsugamushi lacks a proper cell wall (lipopolysaccharide and peptidoglycan) and instead has a slime layer, the cephalosporin groups of antibiotics are virtually ineffective against scrub typhus (Walker 1996, Patrick et al. 2009). The recommended antibacterial therapy is with Doxycycline. Azithromycin is an alternative in children or pregnant women. Rifampicin and azithromycin are alternatives in cases resistant to doxycycline (Cennimo DJ 2015). In these endemic regions, empirical therapy with doxycycline or azithromycin in undiagnosed fever cases may be life saving even if eschars are not observed.
The limitation of this study was that the results were based primarily on a single parameter (ELISA) where the issue of false positivity cannot be ignored. Although testing with some other assays such as Weil Felix tests or indirect immunofluorescence assay could be confirmatory for acute cases, enzyme immunoassay based on IgG detection being fast, reliable, and easy, requiring not much sophistication, is ideal for elucidating the prevalence or past contact with the pathogen. It should be noted that scrub typhus IgG antibodies were not detected in the 34 healthy control samples collected from health workers from Dibrugarh district (a nonendemic area for scrub typhus), which reflects the minimum probability of false positivity of the assay.
Conclusion
In remote regions of northeast India like Arunachal Pradesh, epidemiology and burden of rickettsial disease are largely undiscovered. This study shows that scrub typhus infections may be one of the important causes of undiagnosed fever in Arunachal Pradesh. Therefore, active surveillance has to be done to understand exact magnitude, epidemiological aspects, and distribution of vector and disease burden of this reemerging neglected tropical disease.
Footnotes
Acknowledgment
The authors acknowledge Ms. Monisha Dowerah and Ms. Nazmin Begum for their excellent assistance in the laboratory.
Author Disclosure Statement
No competing financial interests exist.