
Abstract
Background:
A Lyme disease (LD) diagnosis can be far from straightforward, particularly if erythema migrans does not develop or is not noticed. Extended courses of antibiotics for LD are not recommended, but their use is increasing. We sought to elucidate the patient patterns toward a diagnosis of LD, hypothesizing that a subset of patients ultimately receiving extended courses antibiotics may be symptomatic for an extended period before the first LD diagnosis.
Methods:
Claims submitted to a nationwide U.S. health insurance plan in 14 high-prevalence states were grouped into standardized diagnostic categories. The patterns of diagnostic categories over time were compared between patients evaluated for LD and given standard antibiotic therapy (PLDSA) and patients evaluated for LD and given extended antibiotic therapy (PLDEA) in 2011–2012.
Results:
The incidence of PLDSA was 40.45 (N = 3207) and that of PLDEA was 7.57 (N = 600) per 100,000 insured over 2011–2012. 50.3% of PLDEA were diagnosed in the nonsummer months. Seven diagnostic categories were associated with PLDEA. From 180 days before the first LD diagnosis, the risks of having claims associated with back problems (odds ratio [OR], 2.1; confidence interval [95% CI], 1.4–2.9; p < 0.001) and connective tissue disease (OR, 1.6; 95% CI, 1.1–2.3; p < 0.01) complaints were higher among PLDEA. From 90 days before the diagnosis, malaise and fatigue (OR, 1.7; 95% CI, 1.1–2.6; p < 0.05), other nervous system disorders (OR, 2.0; 95% CI, 1.3–3.1; p < 0.01), and nontraumatic joint disorder (OR, 1.4; 95% CI, 1.0–2.0; p < 0.05) were more likely found among PLDEA than PLDSA. From 30 days before the diagnosis, the risk for mental health (OR 1.6; 95% CI, 1.1–2.0; p < 0.01) and headache (OR 1.5; 95% CI, 1.1–2.0; p < 0.05) among PLDEA was elevated.
Conclusions:
Among patients evaluated for LD and ultimately receiving an extended course of antibiotics for LD, 15.8% of them were symptomatic and seeking care for several months before their first LD diagnosis.
Introduction
L
Early LD can be treated effectively with 2 weeks of antibiotics, and late LD can be treated with 4 weeks of antibiotics (Wormser et al. 2006, Halperin et al. 2007). If untreated, LD may lead to neurologic and rheumatologic manifestations weeks to months later (Centers for Disease Control and Prevention 2015c). Even after standard treatment, about 10–20% of patients with LD report nonspecific persistent symptoms, such as fatigue, headache, widespread musculoskeletal or joint pain, and cognitive difficulties (Shadick et al. 1994, Seltzer et al. 2000, Cerar et al. 2010, Weitzner et al. 2015). These nonspecific symptoms may result in a diagnosis of post-treatment LD syndrome (Centers for Disease Control and Prevention 2015c), especially when the diagnosis is delayed or the treatment is inadequate (Kalish et al. 2001). We recently documented increasing use of extended treatment for LD (Tseng et al. 2015a), even though studies have concluded that extended antibiotic therapy provides no meaningful benefit (Klempner et al. 2001, Kaplan et al. 2003, Krupp et al. 2003, Wormser et al. 2006, Feder et al. 2007, Fallon et al. 2008, Klempner et al. 2013, Berende et al. 2016) and the approach is not recommended by the Infectious Disease Society of America (IDSA) (Wormser et al. 2006).
For patients given standard or extended courses of antibiotics after diagnosis with LD, we sought to elucidate patient patterns toward a diagnosis of LD, hypothesizing that a subset of patients ultimately receiving extended courses antibiotics have been symptomatic and seeking diagnosis for nonspecific symptoms before receiving a Lyme diagnosis.
Methods
Study population and data
We performed a population-based retrospective cohort study by using insurance claims submitted to a nationwide, private health insurance plan in the United States from July 2010 to December 2012, for patients residing in the 14 states with a high-prevalence of LD—Connecticut, Delaware, Maine, Maryland, Massachusetts, Minnesota, New Hampshire, New Jersey, New York, Pennsylvania, Rhode Island, Vermont, Virginia, and Wisconsin (Centers for Disease Control and Prevention 2015a).
Each insurance claim-defined encounter was coded with up to six ICD-9 (International Classification of Diseases, Ninth Revision) codes. Prescription drugs were reported by date, National Drug Code, and quantity dispensed (in days). Laboratory orders were coded with the Current Procedural Terminology (CPT) codes. Following established practices (Ryan 2010a, b, Tseng et al. 2015a, b), we merged two visits with the same diagnosis codes into a “condition era” (Ryan 2010a) and two prescriptions for the same antibiotic(s) into a single “drug era” (Ryan 2010b). The Boston Children's Hospital Institutional Review Board approved the study, granting a waiver of consent.
Case identification
Using a published LD claims data-based case definition (Tseng et al. 2015a, b), patients were initially included in the cohort of newly diagnosed patients with LD if they had least one LD diagnosis code (ICD-9 code: 088.81) in the principal diagnosis field of a claim. Cases were also required to have at least one serologic test order within 90 days before or after any LD condition era (test results were not available) and a 2-week or longer course of one of the antibiotics recommended for the treatment of LD (Wormser et al. 2006) started within 30 days before or after the LD condition era. Patients evaluated for LD and given standard antibiotic therapy (PLDSA) are defined as those receiving 2–5 weeks of antibiotics. Patients evaluated for LD and given extended antibiotic therapy (PLDEA) are defined as receiving ≥5 weeks of therapy. In summary, the PLDEA case definition requires ≥1 LD ICD-9 code, ≥1 LD serologic testing order, and antibiotic therapy for ≥5 weeks. The PLDSA definition is similar, but the length of antibiotic therapy was 2–5 weeks.
To enrich the cohort for patients beginning their diagnostic pattern, we included beneficiaries enrolled in the plan for at least 180 days before an LD diagnosis and who received the first LD diagnosis from January 2011 to December 2012.
Outcome measures
We assessed the association between PLDEA and diagnoses grouped into clinically meaningful diagnostic categories by using the Agency for Healthcare Research and Quality Clinical Classifications Software (CCS) (Agency for Healthcare Research and Quality 2015). CCS is a diagnosis and procedure categorization scheme, collapsing ICD-9 codes into a smaller number of clinically meaningful categories (Agency for Healthcare Research and Quality 2015). Individual ICD-9 codes were grouped into CCS-level 1 categories. ICD-9 codes related to symptoms and signs were grouped by CCS-level 3 categories (groups 17.1.1–17.1.9). ICD-9 codes related to nervous system, sense organs, musculoskeletal system, and connective tissue were grouped by CCS-level 2 categories (group 6.1–6.9 and 13.1–13.9). Each category is defined as a binary variable, based on the presence or absence of at least one ICD-9 code from the appropriate category occurring during defined 30 day time periods between 1 and 180 before a patient's first LD diagnosis.
Statistical analysis
The presence of a diagnosis within the diagnostic categories among PLDEA was compared with the presence in PLDSA by using logistic regression, adjusted by age and gender, and expressed as odds ratios (ORs). All analyses were performed by using R software (version 3.1.3, R Foundation for Statistical Computing,
Results
Incidence of patients evaluated for LD
A total of 7,928,693 insured individuals resided in the 14 states with a high-prevalence of LD. Of these, 3207 and 600 individuals met the case definitions for PLDSA and PLDEA, respectively. The demographic characteristics and antibiotic therapy of PLDSA and PLDEA cases in the study period are described in Table 1. Compared with PLDSA, PLDEA cases were more likely to be women, older, and diagnosed with LD outside of summer months. The incidence rates of PLDSA and PLDEA cases estimated from our study population from 2011 to 2012 were 40.45 and 7.57 per 100,000 insured, respectively. A small group of providers (5.2%) account for a substantial fraction (30.2%) of patients evaluated for LD receiving extended antibiotic courses.
If patients have more than one antibiotic course, we select the longest course for analysis.
IQR, interquartile range; LD, Lyme disease.
Patterns of Non-LD diagnoses among patients evaluated for LD
Among PLDEA, the most common diagnostic categories recorded within 6 months before the LD diagnosis are shown in Figure 1, including endocrine, nutritional, metabolic and immunity disorders, malaise and fatigue, nontraumatic joint disorders, and other connective tissue diseases. From 151 to 180 days before the first LD diagnosis, the most common diagnostic categories were endocrine, nutritional, metabolic, and immunity disorders, recorded in 53 (8.8%) PLDEA. From 1 to 30 days before the first LD diagnosis, the most common diagnostic categories were nontraumatic joint disorders, recorded in 142 (23.7%) PLDEA. The percentage of PLDEA with all the common diagnostic categories were increased closer to the first LD diagnosis date. The most common diagnosis codes in each diagnostic category condition are shown in Table 2.
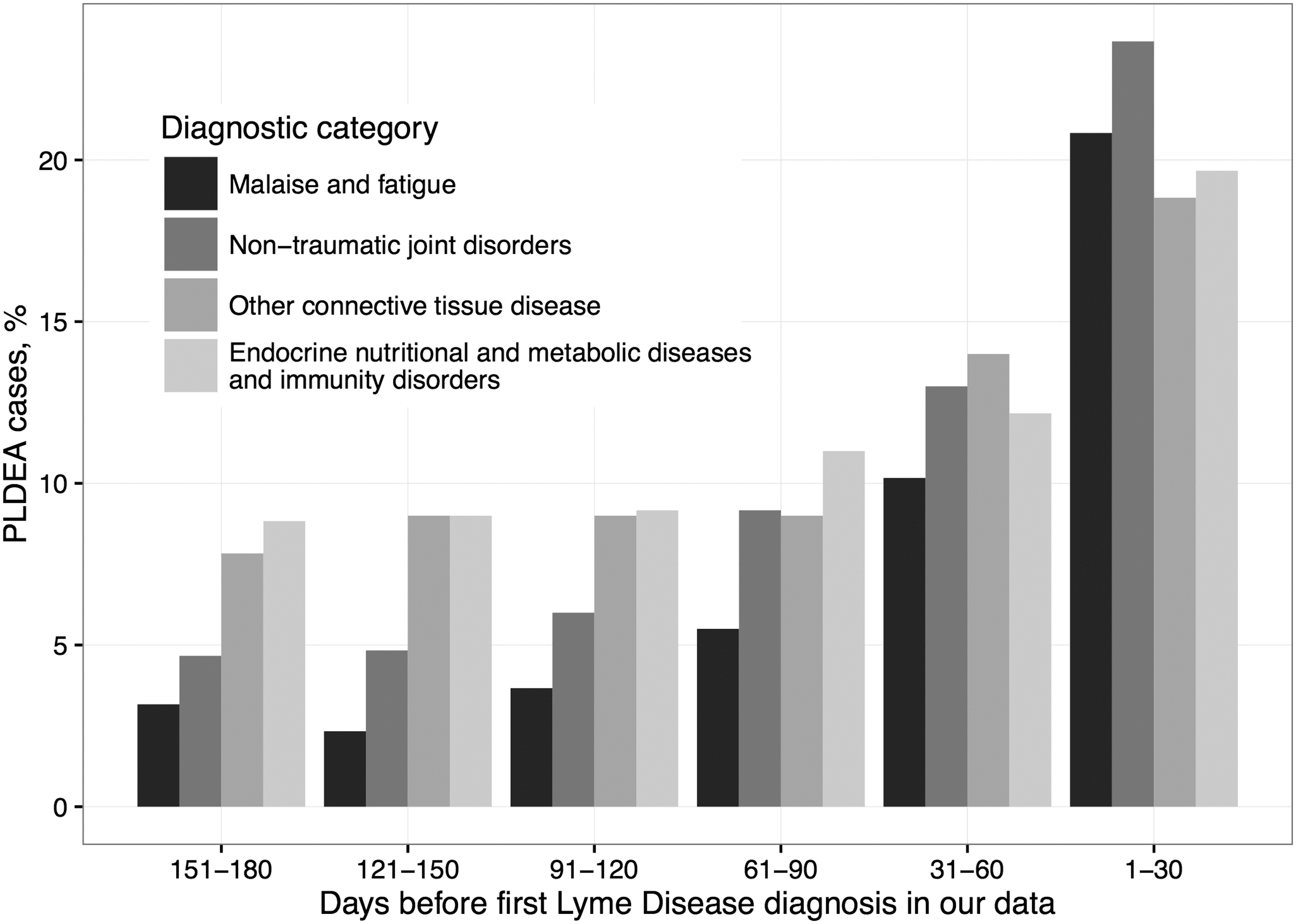
Time trends of diagnostic categories assigned to patients evaluated for LD and given extended antibiotic therapy (PLDEA). Period is within 6 months before the first diagnosis for LD during the study period. LD, Lyme disease.
The number and percentage of patients having at least one ICD-9 code from among the most common diagnostic categories recorded within 6 months before the first diagnosis of LD. The numbers in each field indicate the number of PLDEA with the ICD-9 codes/total number of PLDEA with the diagnostic category.
Diagnostic patterns among PLDEA
Table 3 shows the risk for claims associated diagnostic categories in PLDEA compared with PLDSA from 1 to 180 days before the first LD diagnosis. Figure 2 maps out the temporal, risks for PLDEA compared with PLDSA in the 6 months leading up to the first diagnosis of LD. From 151 to 180 days before the first LD diagnosis, the risks for claims associated with back problems (OR, 2.1; confidence interval [95% CI], 1.4–2.9; p < 0.001) and other connective tissue disease (OR, 1.6; 95% CI, 1.1–2.3; p < 0.01) were elevated among PLDEA. From 61 to 90 days before, claims associated with malaise and fatigue (OR, 1.7; 95% CI, 1.1–2.6; p < 0.05), other nervous system disorders (OR, 2.0; 95% CI, 1.3–3.1; p < 0.01), and nontraumatic joint disorders (OR, 1.4; 95% CI, 1.0–2.0; p < 0.05) are more likely among PLDEA. From 1 to 30 days before, the risks of mental illness (OR, 1.6; 95% CI, 1.1–2.0; p < 0.01) and headache (OR, 1.5; 95% CI, 1.1–2.0; p < 0.05) associated claims are higher. In contrast, the only low risk claims associated diagnostic category in PLDEA is skin and subcutaneous disorders (OR, 0.6; 95% CI, 0.5–0.9; p < 0.01) occurring up to 30 days before the first LD diagnosis in the study period.
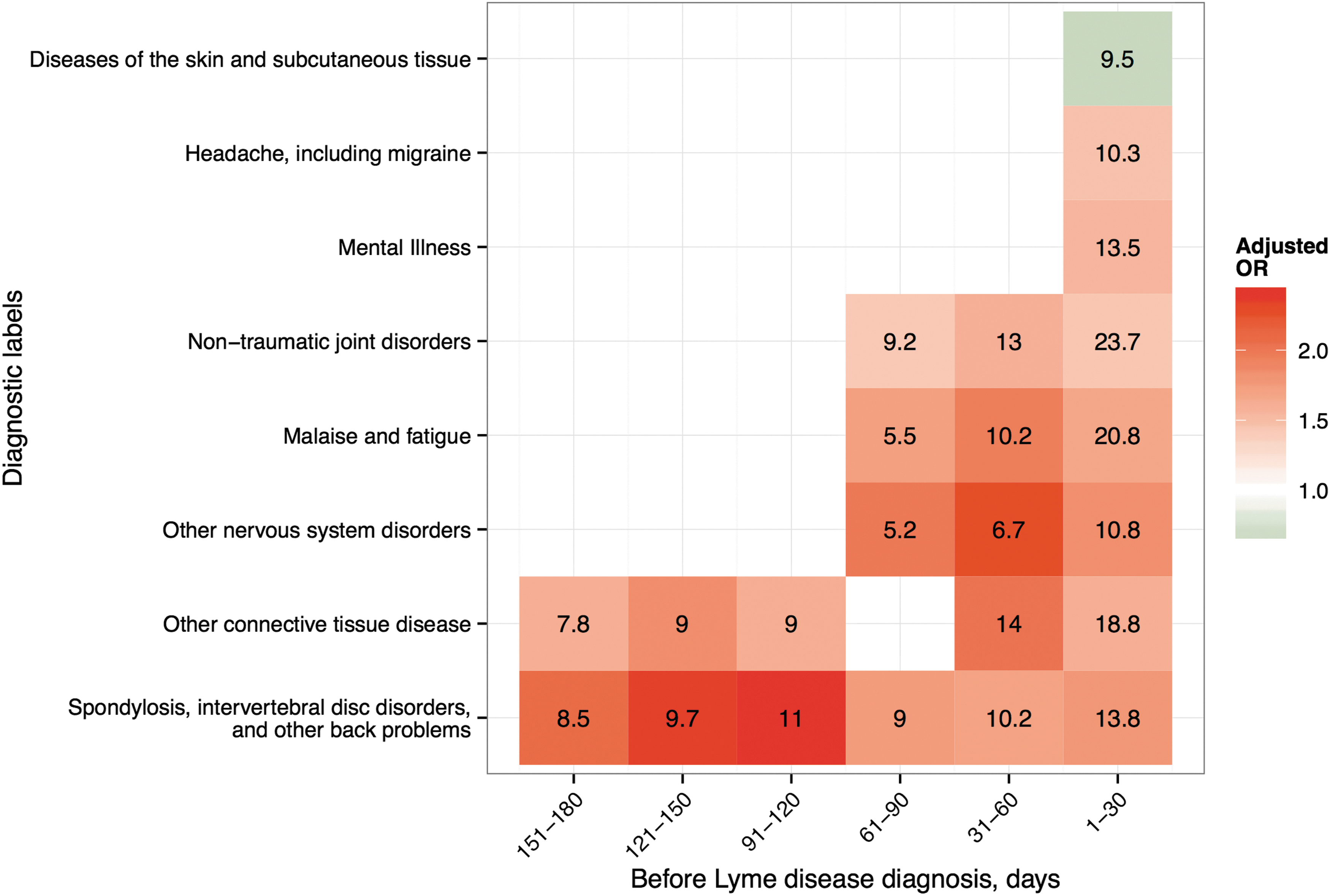
Claims associated diagnostic classification. The temporal risk for claims associated diagnostic categories in PLDEA compared with PLDSA in the 6 months leading up to the first diagnosis of LD. The colors in blocks indicate the odds of diagnostic categories in PLDEA compared with PLDSA, for statistically significant (p < 0.05) relationships. The numbers on the color blocks indicate the percentage of PLDEA patients assigned the diagnostic category.
CI, confidence interval; OR, odds ratio.
Seasonality
More PLDEA (50.3%) than PLDSA (40.0%) are diagnosed in the nonsummer months (p < 0.001). Of those PLDEA, 85.8% had a diagnosis in at least one of the PLDEA-associated diagnostic categories before the LD diagnosis, compared with 70.5% of PLDEA diagnosed in the summer months (p < 0.001).
Discussion
People who received extended courses of antibiotics for the treatment of LD were at higher risk for claims associated nonspecific signs and symptoms that were consistent with LD (Shadick et al. 1999, Seltzer et al. 2000, Kowalski et al. 2010, Wormser et al. 2014, Centers for Disease Control and Prevention 2015d, Weitzner et al. 2015), including fatigue, headache, joint pain, and connective tissue diseases before their first LD diagnosis during the study period.
The incidence of claims associated with back problems and connective tissue diseases was elevated in every backtracked period before PLDEA were diagnosed with LD (Wormser et al. 2006, Centers for Disease Control and Prevention 2015d). The nonspecific nature of a complaint like back pain may either elucidate a common symptom experienced by LD sufferers or highlight the nonspecific nature of the presentation of patients eventually diagnosed with LD, whether or not the diagnosis is accurate. Skin and subcutaneous tissue diagnoses are the only category more likely to be found among PLDSA. Given the distinct character of the EM rash and the effectiveness of prompt treatment (Massarotti et al. 1992, Wormser et al. 2003), this is not surprising.
Compared with PLDSA, PLDEA cases exhibited a strong female predominance. We adjusted the risks for diagnostic categories in PLDEA compared with PLDSA by age and gender to focus on their particular diagnostic pattern. The life cycle of the tick predisposes occurrence of LD cases to the summer season when the nymphs, considered to account for up to 90% of LD transmission, are the most active (Centers for Disease Control and Prevention 2015a). However, only about half of PLDEA were diagnosed in summer months. One explanation is that the patients diagnosed outside of the summer season had delayed diagnosis (Steere 2001, Wormser et al. 2006); another explanation is that LD was missed or that other conditions were attributed to LD. Diagnostic errors are clinically and financially costly, need attention as much as other medical errors, and should be defined and measured (Khullar et al. 2015, McGlynn et al. 2015).
We found that a distinct and small group of providers diagnosed a substantial fraction of the PLDEA in the study population, consistent with our previous analysis of a separate dataset (Tseng et al. 2015a). The discussion among patient communities, and in traditional and social media (Cooper and Feder 2004, Macauda et al. 2011, McClellan 2012) might drive patients on a diagnostic pattern to a variety of specialists. Some specialists might use nonevidence-based methods for the diagnosis of and treatment for LD (Feder et al. 2007, Auwaerter et al. 2011, Patrick et al. 2015). Patients not diagnosed by standard two-tiered antibody testing, but instead by alternative tests, have a potentially high false-positive rate and share characteristics with patients with chronic fatigue syndrome (CFS) (Prins et al. 2006, Patrick et al. 2015). Some patients in our cohort with PLDEA were diagnosed with CFS (ICD-9 = 780.71) within 180 days before their LD diagnosis, but there were only 16 (2.7%).
Claims data have proved to be a useful source of case identification (Sickbert-Bennett et al. 2010), and may be an important source of surveillance data on the increasing incidence of LD and antibiotic use in LD. Nonetheless, there are several limitations of this study. Although we implemented a 180-day lead-in period, the first LD diagnosis during the study period may not be the first LD diagnosis. Because we relied on claims data, test results were not available, and diagnosis codes may vary in accuracy (Sickbert-Bennett et al. 2010). Hence, PLDEA and PLDSA incidence may be overestimated by including patients who received antibiotics despite negative test results, or they may be underestimated by ignoring patients who were not tested but had EM, had a non-FDA-approved test performed, or were treated with antibiotics paid out-of-pocket and not captured in claims. Of course, the nature of claims data does not permit detailed insight into the diagnostic workup nor for the motivations for treatments. We are unable to know whether the cases for which LD claims were submitted were diagnosed based on published criteria (Wormser et al. 2006, Centers for Disease Control and Prevention 2015b). The incidence rates of PLDEA and PLDSA are somewhat lower than the rates we reported in a previous study using claims data from a different payor and a different study period (Tseng et al. 2015a, b) and population.
Conclusions
A subset of patients (15.8%) who were evaluated for, and diagnosed with, LD and, ultimately, received an extended course of antibiotics for LD were symptomatic and seeking care for several months before their first LD diagnosis. Defining diagnostic patterns in claims data may help elucidate the diagnostic classifications made by clinicians before arriving at an LD diagnosis. Ultimately, these findings could be used to prospectively identify and target patients who are likely to receive an LD diagnosis several months hence.
Footnotes
Acknowledgments
This work was supported by a contract from the Massachusetts Department of Public Health [Contract ID INTF5104HH4300522092]. Tseng was funded by grants from the Ministry of Science and Technology, Taiwan, MOST105-2218-E-182-003 and from Chang Gung Memorial Hospital, CMRPD3F0051. The Ministry of Science and Technology and Chang Gung Memorial Hospital were not involved in designing or conducting the study, data collection, management, analysis, or interpretation, nor the preparation, review, and approval of the article.
Author Disclosure Statement
No competing financial interests exist.