
Abstract
Introduction:
Babesiosis is an emerging tick-borne disease (TBD) caused by Babesia microti, an intracellular parasite of red blood cells. Currently, it is the highest ranked pathogen transmitted by blood transfusion. Most healthy individuals infected with B. microti are asymptomatic, but may be at risk for chronic infection. Similar to Lyme disease transmitted by Borrelia burgdorferi, B. microti is spread by Ixodes scapularis ticks. The rate of coinfection with these TBDs in humans is unclear as most studies have focused their prevalence in ticks or rodent reservoirs.
Materials and Methods:
In this study, we aimed to determine the seroprevalence of B. microti infection in individuals who tested positive for Lyme disease. Serum samples obtained from 130 subjects in New York were tested by immunofluorescence assay (IFA) for the presence of IgM and IgG antibodies against B. microti.
Results:
Overall, 26.9% of the serum samples tested were positive for IgM and IgG antibodies against B. microti, suggesting exposure to TBD. Individuals who tested positive for Lyme disease as determined by two-tiered serological testing and the presence of both IgM and IgG antibodies directed against B. burgdorferi, were significantly increased for antibodies directed against B. microti (28.6%; p < 0.05), suggesting the possibility of coinfection with both TBDs. In contrast, the Lyme disease-negative control group had only 6.7% of samples seropositive for B. microti.
Conclusions:
These findings suggest the need for more extensive studies investigating infection rates with multiple TBDs in areas where they are endemic and further support for the need to implement an FDA-approved screening test for blood products to help prevent transfusion-transmitted babesiosis.
Introduction
L
Signs and symptoms of early Lyme disease usually occur 1–2 weeks after being bitten by an infected tick (Gerber 2002). The most distinguishing physical feature associated with Lyme disease is a distinctive expanding skin lesion called erythema migrans (EM), which forms at the site of the tick bite in 70–80% of cases, resembling a bull's-eye lesion (Smith 2002). The skin lesion is frequently accompanied by flu-like symptoms, such as malaise, fatigue, headache, arthralgias, myalgias, and fever (Steere 1983). If left untreated, Lyme disease can cause chronic joint inflammation, known as Lyme arthritis, neurological symptoms such as facial palsy and neuropathy, and/or heart rhythm irregularities (Wormser et al. 2006).
The CDC recommends serology as the preferred initial diagnostic test through the use of a two-tier testing system that includes an enzyme-linked immunosorbent assay (ELISA) initially, followed by a qualitative Western blotting assay to help confirm the diagnosis (Centers for Disease Control and Prevention 1995). It has been found that IgG antibodies are detectable in individuals who have symptoms beyond 4 weeks (Sehgal and Khurana 2015). Detection rates for serum antibodies range from 20% to 50% in early localized disease and increase with duration of infection, with 70–90% of patients testing positive in the early disseminated stage and nearly 100% in late disease (Sehgal and Khurana 2015).
Human babesiosis is an emerging zoonotic TBD caused by Babesia, obligate intracellular parasites of erythrocytes (Vannier and Krause 2012). The white-footed mouse and the white-tailed deer are thought to act as reservoir hosts for vector ticks, providing the blood meal that adult deer ticks require for reproduction (Thompson et al. 2001, Joseph et al. 2011). Humans are the accidental host and can acquire the disease through the bite of an infected tick (Thompson et al. 2001). Although babesiosis is a zoonotic disease, human-to-human transmission has also been documented through blood transfusion (Blood Products Advisory Committee 2015). Babesia has also been reported to have the capability of crossing the placenta of a pregnant mother and infecting the fetus in the womb (Surra and Jesus 2015).
Most cases of babesiosis consist of a mild to moderate illness characterized by the gradual onset of malaise and fatigue, followed by intermittent fever and one or more of the following: chills, sweats, headache, arthralgia, myalgia, anorexia, and cough (Vannier and Krause 2012). Those who are at the greatest risk for severe babesiosis are asplenic individuals, individuals with congenital or acquired immunodeficiencies, and the elderly (Rożej-bielicka 2015).
The diagnosis of babesiosis relies strongly on clinical laboratory examinations due to the lack of easily recognized clinical signs (Vannier and Krause 2012). A definitive diagnosis is made using microscopic identification of Babesia on thin blood smears with Giemsa or Wright staining, where B. microti trophozoites appear as pleomorphic ring forms (Mosqueda et al. 2012). If a smear is negative, other laboratory tests are used in helping to establish the diagnosis (Vannier and Krause 2012). Detection of antibodies against the parasite can be measured using indirect immunofluorescence assay (IFA). IgM antibodies directed against Babesia are usually first detected 2 weeks after the onset of the illness during the acute phase of the illness, and decline within 8–12 months (Ruebush et al. 1981, Krause et al. 1996a). In addition, PCR is a highly sensitive and specific method in detecting Babesia DNA in blood, using primers complementary to the small ribosomal subunit genes (Krause et al. 1996a, 1996b).
Babesiosis became a notifiable disease on January 1, 2011 (Babesiosis Surveillance 2012). In 2013, the CDC was notified of 1,762 positive cases of babesiosis, which represented 22 of the 27 states that were required to report positive patients (Lyme Disease Surveillance 2015). The number of babesiosis cases has trailed those of Lyme disease. This is perhaps because it has been reported that B. burgdorferi is more efficiently transmitted to its hosts (Mather et al. 1990). Moreover, patients with babesiosis lack a readily identifiable hallmark such as the erythema migrans rash seen often in Lyme disease and typically present with more generalized symptoms associated with flu-like illness, making it more difficult to distinguish from numerous other conditions (Krause et al. 2004).
Currently, B. microti is the highest ranking pathogen that is transmitted by blood transfusion in the United States, for which there is no FDA-approved donor screen currently implemented (Vannier and Krause 2012). Transfusion-transmitted babesiosis (TTB) has high fatality in transfusion recipients with 28 deaths attributed to complications from TTB reported from 1979 to 2009 and 4 TTB-associated deaths reported to the FDA between 2010 and 2014 (Herwaldt et al. 2011). It is assumed that the actual number of acquired TTB cases may be much higher than currently reported since many recipients of infected blood transfusions may remain asymptomatic.
B. microti and B. burgdorferi, the causative agents of human babesiosis and Lyme disease, respectively, are prevalent within the same geographical range (Dunn et al. 2014). I. scapularis ticks may be infected with either of these pathogens or both simultaneously (Swanson et al. 2006). In a recent study conducted in New York, a total of 11,204 ticks were tested for infection with B. microti and B. burgdorferi. It was found that 14.4% of nymphs and 45.7% of adult ticks were infected with B. burgdorferi compared with only 2.7% and 2.5%, respectively, for B. microti; however, they also reported that both nymph and adult ticks that were collected had a higher than expected coinfection rate (Hersh et al. 2014). This is in agreement with others who have suggested that concurrent infection with B. burgdorferi may have a synergistic effect on B. microti (Dunn et al. 2014).
Reported coinfection rates of B. microti with B. burgdorferi in humans vary greatly and can range from 10% to 32% (Krause et al. 1996c, Johnson et al. 2014). It is believed that B. burgdorferi has contributed to the emergence and expansion of B. microti. Coinfection with multiple TBDs can affect the intensity and duration of symptoms in humans, making its diagnosis and treatment more challenging (Hersh et al. 2014). Additionally, treatment of Lyme disease is generally an oral regimen of doxycycline for early localized disease and intravenous regimens for those who have developed neurologic symptoms, symptomatic cardiac disease, and/or refractory Lyme arthritis (Wright et al. 2012). Doxycycline is the preferred oral treatment because it has activity against other tick-borne illnesses such as human granulocytic anaplasmosis, whereas the treatment for babesiosis is a combination of atovaquone and azithromycin (Wormser et al. 2006, Vannier and Krause 2012, Wright et al. 2012).
The rate of coinfection with TBDs in humans is unclear. Most studies have focused on coinfection in ticks or rodent reservoirs. We believe there will be a high rate of seroprevalence of antibodies directed against B. microti in individuals who are also seropositive for B. burgdorferi, the causative agent of Lyme disease. This study aims to determine the rate of seropositivity for B. microti in these individuals from New York State by testing serum samples determined positive by two-tier serological testing for Lyme disease.
Materials and Methods
Study samples
Serum samples were provided by Northwell Health Core Laboratories located in Lake Success, NY. All samples used in this study were deidentified in accordance with HIPAA regulations and IRB approval was obtained before the study began. Due to its retrospective nature, the only demographical information available for our analyses were age and sex. No additional clinical information was provided. A total of 154 samples were obtained for use in this study during the months when Lyme disease and babesiosis are most prevalent. Of the total samples received, 130 samples were subjected to two-tier testing for Lyme disease and were included in our analyses. In June, 31 samples (23.8%) were collected, 44 (33.9%) in July, 39 (30%) in August, and 16 (12.3%) in September. Samples were collected from 75 (57.7%) males, 52 (40%) females, and 3 (2.3%) were of unknown gender. The age range was 2–93 years. The mean age was 45.2 years with 51 years as the median.
VIsE chemiluminescent immunoassay
Serum samples were screened for Lyme disease at Northwell Health Core Laboratory for antibodies against Borrelia VIsE (variable major protein-like sequence, expressed) antigens using the Liason® Borrelia burgdorferi indirect chemiluminescence immunoassay (DiaSorin, Stillwater, MN). All assay steps (with the exception of magnetic particle resuspension) were performed on the Liaison XL analyzer by the same manufacturer. Liason-provided B. burgdorferi-negative and -positive serum controls were run daily for each shift the analyzer was in use. Results <0.90 were considered negative and absent of detectable B. burgdorferi antibodies. Results that were equivocal (0.90–1.90) and positive (≥1.10) were tested by Western blotting assay.
Western blotting assay
Positive samples were confirmed by qualitative Western blotting assay for IgM and IgG antibodies directed against Borrelia burgdorferi, using the MarDx B. burgdorferi Marblot Strip Test System (Trinity Biotech, Jamestown, NY), and processed using reagents supplied by the manufacturer in accordance with their recommendations. All assay steps were performed on the TrinBlot Processor and Scanner Version 3.4. Briefly, B. burgdorferi (B-31 strain) antigen was separated by SDS-PAGE and then transferred to nitrocellulose membranes and provided as testing strips by the manufacturer. Serum samples were incubated with strips, washed, and then incubated with alkaline phosphatase-conjugated anti-human IgG. Western blot-negative and weakly reactive IgG controls were used along with the IgG serum band locator as the positive control. Detection and identification of bands were performed using the serum band locator as a reference for position and the weakly reactive control as an indicator of intensity. Bands were either absent (negative reactivity score), less than the intensity of the 41 kDa band on the weakly positive control strip (cutoff for the negative reactivity score), or greater than or equal to the intensity of the 41 kDa band on the weakly positive control (positive reactivity score). Samples were considered positive for IgM antibodies if 2 of 3 bands (23, 39, and 41 kDA) were present and for IgG if 5 of 10 bands (18, 23, 28, 39, 41, 45, 58, 66, or 93 kDA) were present.
Both VIsE screening and Western blotting confirmation testing were performed in laboratories that are fully licensed and accredited by the New York State Department of Health, Joint Commission on Accreditation of Health Care Organizations (JCAHO), and the College of American Pathologists (CAP).
IFA of B. microti
The B. microti indirect fluorescence immunoassay (IFA) IgM and IgG antibody kits were used for the detection antibodies against B. microti in human serum samples in accordance with the manufacturer's recommendations (Gentaur, Inc., San Jose, CA). Briefly, serum samples were incubated in wells on slides containing fixed B. microti-infected hamster erythrocytes. DyLight 488-labeled donkey and anti-human IgM and IgG antibodies were used, respectively, to visualize fluorescence in positive samples. Positive and negative controls provided by the manufacturer were included on each slide, processed in parallel with serum samples for comparison, and used to determine cutoff ranges for positive titers. All serum samples were initially screened at a titer of 1:16 and compared with control wells. Samples that were inconclusive or positive at 1:16 screening dilutions were then used to develop endpoint titers. These samples were retested at titers of 1:16, 1:32, 1:64, 1:128, and 1:256. For IgM antibodies, samples were considered positive at a titer ≥1:32 (normal reference range is a titer <1:20). A titer ≥1:64 was considered positive for IgG antibodies (normal reference range is a titer <1:64). Each sample was tested a minimum of two times. In addition, all IFA slides were subjected to blinded analysis by two independent researchers. For the purposes of our study, only samples that were positive for both IgM and IgG antibodies were considered positive for B. microti. Statistical significance was determined using the chi-squared test for goodness of fit using Microsoft® Office Excel. Other statistical analyses (data not shown) were performed using Microsoft Office, Stata/SE 13.1.
Microscopy
Images were captured using a Zeiss Axio Vert 40 CFL inverted microscope with 3-channel fluorescence (DAPI, GFP, and Texas Red). All images were acquired with a Zeiss A-Plan 40 × objective (NA = 1.25) and processed with Zeiss software (ZEN, blue edition). When necessary, images were further processed using Adobe Photoshop, adjusting contrast and/or brightness for optimal viewing. Each channel was adjusted separately and changes were applied to the whole field.
Results
Although TBDs can occur anytime throughout the year, we collected our samples during the months of peak onset (Fig. 1A). The samples used in this study included 75 males (57.7%), 52 females (40%), and 3 samples of unknown gender (2.3%) (Fig. 1B). There was a wide age range between 2 and 93 years of age, with a mean age of 45.2 and a median of 51 years of age (Fig. 1C).
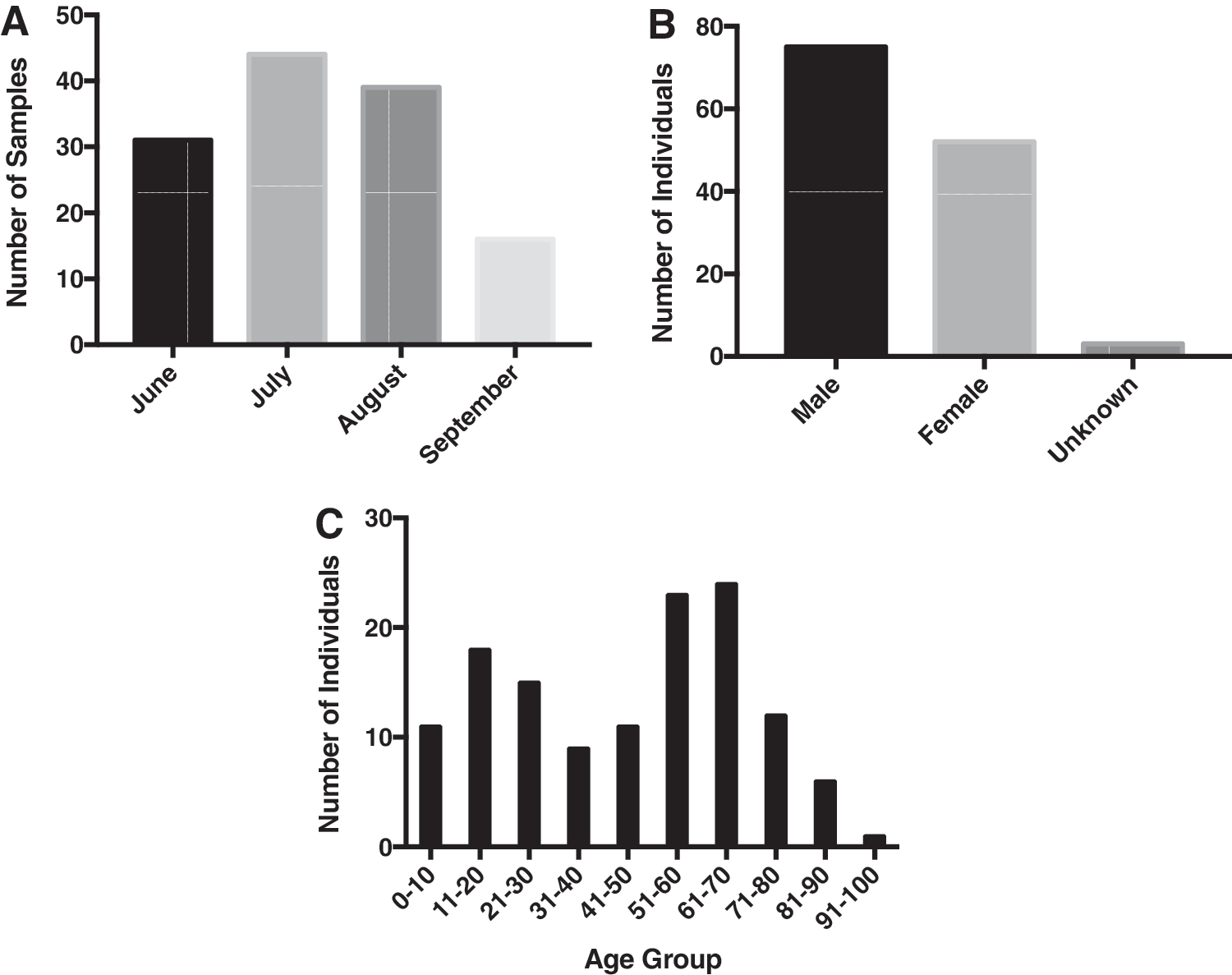
Sample demographics.
First, the two-tiered testing system for Lyme disease recommended by the CDC was used in this study to determine the presence of Lyme disease. Samples were screened by the VIsE chemiluminescence immunoassay (CLIA) to test for Lyme antibodies specific for the immunodominant antigen of VIsE protein, which generates a strong immune response early in the infection and within all stages of Lyme disease. The serum samples were screened for antibodies against B. burgdorferi, as described in the Materials and Methods section. Of the 130 samples, 15 individuals tested negative, 113 tested positive, and 2 samples were equivocal for antibodies against the VIsE antigen (Fig. 2A).

Results of VIsE and Western blotting assays for Lyme disease.
All positive or equivocal results (115 samples) for the VIsE assay were automatically reflex tested for a Lyme Western blot assay. We found that 88 individuals tested positive for IgM antibodies, 27 tested positive for IgG antibodies, and that 42 of these samples (36.5% of the total tested) were positive for both IgM and IgG antibodies (Fig. 2B). The CDC recommends that a positive IgM Western blot assay is only diagnostic if it is during the first 4 weeks of the course of the disease and that it is more likely to cause false-positive results (Lyme Disease Surveillance 2015). Thus, due to the retrospective nature of this study and lack of clinical information, we only considered individuals who tested positive by CLIA as well as both IgM and IgG antibodies by Western blotting assay as positive for a current infection with Lyme disease.
Next, to determine exposure to B. microti, we tested for seropositivity using an IFA. Individuals who were positive for both IgM and IgG antibodies were considered positive for infection with B. microti (Fig. 3). Overall, 35 individuals (26.9%) tested positive for both antibodies against B. microti (Fig. 4). Only one individual (6.7%) of the Lyme disease-negative control group was positive for antibodies against B. microti. Samples that were positive for either Lyme IgM or IgG antibodies showed that 19 (41.3%) and 3 (11.1%) were positive for B. microti, respectively. Of those we considered positive for a current Lyme disease infection, 28.6% also tested positive for antibodies against B. microti. This was indicative of seroprevalence for both TBDs, which could potentially suggest coinfection. In addition, seropositivity for B. microti in those infected with Lyme disease was significantly increased (chi-squared goodness of fit, p < 0.05) compared with the negative control group.
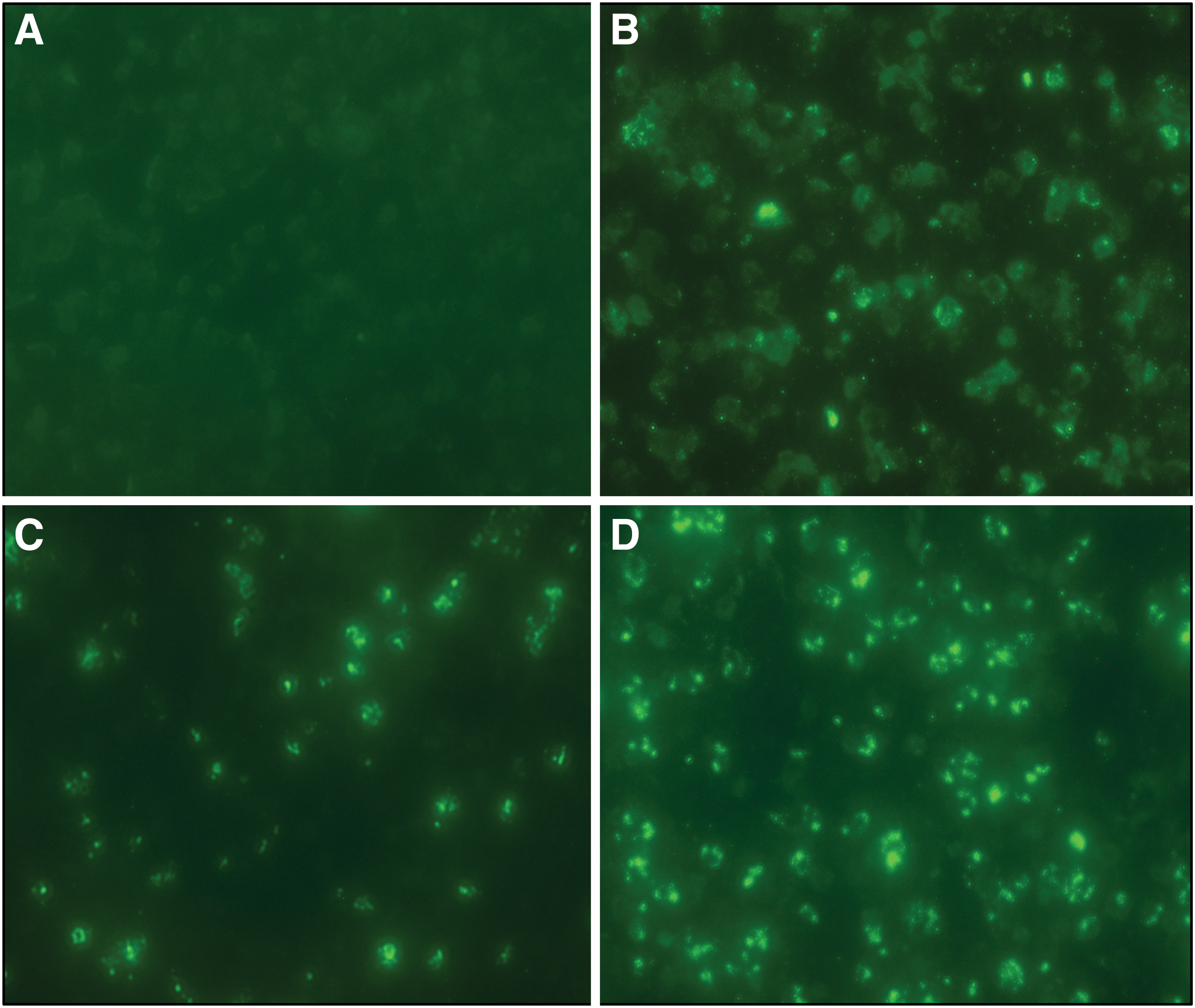
Representative images of B. microti IFA. A titer of 1:32 was used to determine whether an individual was positive for antibodies against IgM, while a titer of 1:64 was used for IgG antibodies.
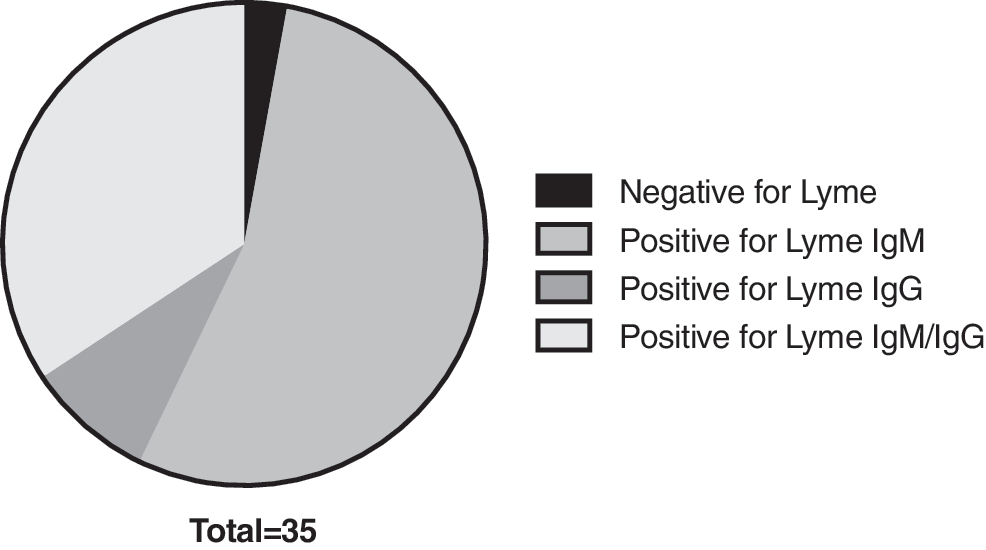
Results of IFA testing for antibodies against B. microti. Of the 130 samples tested, 35 were also seropositive for B. microti. Out of individuals who tested negative for Lyme disease, 46 of those were positive for Lyme IgM antibodies only, and 27 of those who were positive for Lyme IgG only were also positive for antibodies against B. microti. Those who were considered positive for Lyme disease (positive for both IgM and IgG antibodies) had 12 of 42 individuals positive for B. microti and were significantly increased compared with the negative control group and those who had been previously infected with Lyme disease (chi-squared test for goodness of fit, p > 0.05).
We then further categorized our results in terms of gender and age (Fig. 5A,B). Our findings were in agreement with those that have been reported by the CDC with regard to gender and age (Babesiosis Surveillance 2012, Lyme Disease Surveillance 2015). For those with known gender, we found that 64% of those positive for Lyme disease were male and 31% were female (Fig. 5A). In addition, the greatest number of individuals testing positive were in the 0–10 age group (Fig. 5B). The CDC reports that Lyme disease is most common in males aged 5–9 years and that males exceed the number of females in every age bracket until the age of 70 (Lyme Disease Surveillance 2015). Similarly, 60% of those seropositive for B. microti in our study were male and 33% were female. In 2013, the CDC reported that 65% of the reported babesiosis cases were male, 32% were female, and the sex was unknown for 3% (Babesiosis Surveillance 2012). In contrast to Lyme disease, the CDC reported that the highest number of babesiosis cases were found with increased age (50–79 age group), similar to our study. Although we noticed a similar trend to what has previously been reported, we found no statistical significance when testing the relationship between gender, age, and infection rates using various statistical analyses (Pearson's chi-squared test, t-tests on proportions, etc.) or when tested by logistical regression (data not shown).
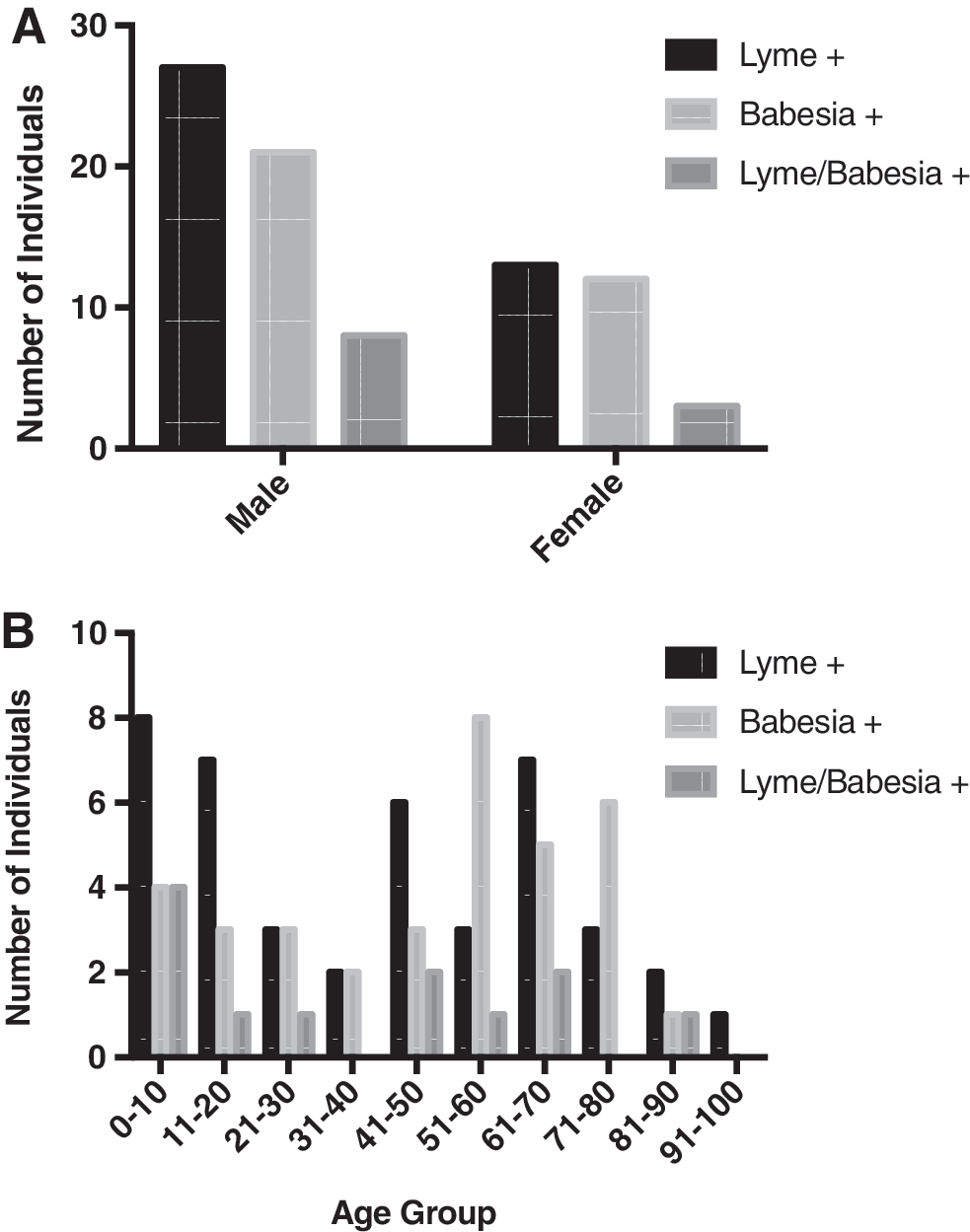
Results of Lyme disease and Babesia testing by gender and age. Number of individuals positive for Lyme, Babesia or both by gender
Discussion
The aim of this study was to determine the prevalence of seropositivity for B. microti in individuals who tested positive for Lyme disease. Overall, we found that 30.4% of the samples tested positive for antibodies against B. microti. In addition, we found that 6.7% of Lyme-negative individuals were positive for antibodies against B. microti and that those we considered positive for current Lyme disease had 26.9% of individuals who also tested positive for antibodies toward B. microti. The seropositivity against both TBDs in these individuals could possibly indicate a coinfection with both TBDs; however, this could not be confirmed due to the lack of clinical information in this study.
These findings were in alignment with our expectations based on previous reports that have cited infection rates with Babesia to be between 10% and 32% (Krause et al. 1996c, Johnson et al. 2014). However, there were several limitations to our study. For the purposes of this study, we are only reporting samples that were positive for both IgM and IgG because IgM antibodies are known to cause nonspecific fluorescence and false-positive results. Moreover, due to the retrospective nature of our study, it is unknown if these individuals were tested for other TBDs such as B. microti. We presumed that these individuals were symptomatic because they were being tested for Lyme disease; however, we have no clinical information regarding previous tick exposure or diagnoses.
A greater number of samples and more equally matched control groups would have allowed for a more thorough statistical analysis of our findings. Our sample size was limited and we had a small number of negative controls that were made available to us for our study. Nevertheless, 6.7% of control samples still tested positive for B. microti. Although a smaller portion of our Lyme disease-negative population tested positive for Babesia, these numbers were consistent with findings of other studies, which have varied greatly (Prusinski et al. 2014). Of the 130 samples analyzed in our study, 35 individuals were positive for antibodies for B. microti and may not have known they were ever infected by Babesia.
In addition, there are several possibilities for the high prevalence of seropositivity for B. microti in our study. One possibility is bias in our sample population. Our results suggest that our sample population may be biased, in that they are being tested for Lyme disease because these individuals may have either (1) had a recent tick bite or (2) are presenting with symptoms that are suggestive of TBD. For these reasons, we would expect there to be an increased incidence compared with a random sampling. As stated previously, we did not have any access to the results of any other clinical tests that may have been performed or have any indication as to why the clinician ordered Lyme disease testing. Suspected infection with a TBD would make it more likely that the samples in our study would test positive. It should be noted that the diagnosis of either Lyme disease or babesiosis must also include careful clinical evaluation and should not be based solely on the detection of antibodies against these TBDs. One possibility for the high seroprevalence in our study is that the areas in which these individuals live are endemic for ticks coinfected with both organisms. This would certainly impact the proportion of ticks infected with the disease and subsequently individuals who may test positive. At the time of this investigation, there was no information available specific to ticks tested in Long Island, New York, where we presumed the majority of these individuals live.
An additional limitation in our study was the use of IFA to determine infection rates. The B. microti IFA IgM antibody kit also provided constraint within our findings. The negative and positive controls in the kits were not ideal. Analyses of the samples were subjective and sometimes very difficult to determine. Many samples that had equivocal results were retested several times to ensure proper determination of seroprevalence. One possibility to overcome the subjectivity of this type of analysis would be to confirm using an alternate method of diagnosis. Ideally, this would be done by using PCR to detect B. microti DNA in individual blood samples. B. microti infects red blood cells, so it would have been more advantageous to also test whole blood samples; however, since our study was retrospective, only serum samples were available for testing. In addition, peripheral smears could have also been conducted on whole blood samples to look for the presence of B. microti in erythrocytes. Last, the kit we used in the study cited no evidence of cross-reactivity, except with other species of Babesia. It is possible that some of these samples were actually infected with another Babesia species; however, this is less likely since B. microti is the most common cause of babesiosis in humans (Parija et al. 2015).
Conclusions
Overall, the findings of our study suggest that additional testing for the prevalence of Babesia needs to be performed, particularly in areas where it is endemic. Moving forward, it would be useful to do a more extensive study with a larger sample size and well-matched controls. The results presented in this study coincide with our hypothesis suggesting that there is a high rate of simultaneous seroprevalence for B. microti and Lyme disease, which could possibly indicate coinfection with both TBDs.
The significance of a higher prevalence of B. microti is important, especially in regard to infected blood products. Currently in the United States, almost 5 million recipients undergo blood transfusions annually (Lobo et al. 2013). A recent study performed by the Red Cross North Central region in Minnesota has been testing blood donor samples. A total of 2,150 donations were tested between October 2010 and November 2011 and 42 donors (2.0%) were positive by IFA (Tonnetti et al. 2012). The state of Minnesota represents 6.5% of reported cases of babesiosis to the CDC (Lyme Disease Surveillance 2015). It could be expected that the number of tested blood donors in New York state would be higher as it represents 37.2% of the total number of CDC-reported babesiosis cases. Thus, the implementation of an FDA-approved screening has the potential to save many lives.
Footnotes
Acknowledgments
The authors would like to thank LIU Post Department of Biomedical Sciences and the LIU Post Research Committee for their generous funding of this project. The authors would also like to thank Dr. Veronika Dolar for her help with the statistical analyses and Dr. Ernestine Vellozzi for her advice and expertise.
Author Disclosure Statement
No competing financial interests exist.