
Abstract
Objective:
Toxoplasma gondii, the causative agent of toxoplasmosis, is a zoonotic obligate intracellular protozoan parasite responsible for the infection of almost one-third of the world's population. T. gondii is particularly threatening for primo-infected pregnant women and may lead, following vertical transplacental transmission, to spontaneous abortion, miscarriage, or severe manifestations in the newborn. The aim of this study was to provide an updated estimate of the seroprevalence of anti-T. gondii antibodies among a group of Lebanese pregnant women and its seroconversion rate.
Methods:
This is a retrospective cohort study, in which medical records of 11,000 pregnant women were screened. These women visited a private Obstetrics and Gynecology clinic located in Beirut, the capital of Lebanon, during the period of January 1994 till September 2015. Serological results of anti-T. gondii immunoglobulin G (IgG) and immunoglobulin M (IgM) results of 2456 Lebanese pregnant women who fulfilled the inclusion criteria were included in the analysis. Seropositivity and seroconversion rates for women with repeated tests were reported according to age and area of residence.
Results:
The overall anti-T. gondii IgG and IgM seropositivity among 2456 Lebanese pregnant women was 82.6% and 1.8% respectively. The highest IgG seropositivity is among the age group of 35–44 years (87.81%) and at the governorate of “Mount Lebanon” (82.95%). Sixty-four seroconversions were detected and two abortions due to T. gondii infection during pregnancy were recorded.
Conclusions:
The seroprevalence of anti-T. gondii IgG among the screened pregnant women in Lebanon is the highest in the Arab region. These results highlight the importance of running a national sample survey to estimate the real potential burden of this infection and its impact on maternal and fetal health.
Introduction
T
Felines, mostly cats, are the definitive hosts and play a pivotal role in horizontal transmission of this parasite to intermediate hosts ingesting contaminated vegetables with oocysts shed in cats' feces (El-Shahawy et al. 2014). T. gondii horizontal transmission may also occur upon ingestion of uncooked meat harboring tissue cysts (Weiss and Kim 2000, Fox et al. 2011). More importantly, T. gondii is one of the rare parasites capable of crossing the transplacental barrier following vertical transmission from a primo-infected pregnant woman to her fetus.
The spectrum of the disease caused by T. gondii varies between individuals and is mainly dependent on the host immune response. While in immunocompetent individuals toxoplasmosis is generally asymptomatic to mild symptomatic (Aqeely et al. 2014), severe symptoms that may lead to death appear as a result of an acute infection or the reactivation of a chronic infection in immunocompromised individuals (Aqeely et al. 2014).
Congenital toxoplasmosis entitles the spectrum of complications resulting from the vertical placental passage of T. gondii from a mother to her unborn child (Bojar and Szymanska 2010). Severity of associated conditions depends on the time of acquisition of the parasitic infection by the mother in reference to her pregnancy progression. In primo-infected mothers, if infection occurs in the first trimester, the result is spontaneous abortion, stillbirth, or severe disease. Infants may be asymptomatic at birth only to develop disease months to years later (Alford et al. 1974). Most often these children develop retinochoroiditis with or without blindness or other neurologic problems, including retardation, seizures, microcephaly, hydrocephalus, and hearing loss (Murray et al. 2012).
Diagnosis of both acute and latent toxoplasmosis is based on serological testing for the presence of immunoglobulin G (IgG) and immunoglobulin M (IgM) anti-Toxoplasma antibodies (Bouhamdan et al. 2010). Additional screening through the avidity test of T. gondii-specific IgG antibodies and PCR analysis of the amniotic fluid are usually used for more certainty (Liesenfeld et al. 2001). Besides diagnosis, the results of these tests can serve for determining the seroprevalence of toxoplasmosis.
Within the different countries of the Arab region, a variation in the seroprevalence of anti-T. gondii antibodies among pregnant women was recorded. For instance, seroprevalence among pregnant women was reported to be 24.1% in Jazan province in Saudi Arabia (Aqeely et al. 2014), 34.1% in Sudan (Elnahas et al. 2003), 53.1% in Kuwait (Iqbal and Khalid 2007), 50.8% among high-risk pregnancy group in Egypt (Kamal et al. 2015), and 15% and 35.1% among women of childbearing age in Turkey and Qatar, respectively (Tamer et al. 2009, Abu-Madi et al. 2010).
In Lebanon, there are no particular guidelines or recommendations for screening and therapeutic management used in clinical practice of obstetricians, when Toxoplasma infection occurs during pregnancy (Atallah 2010). The most updated information goes to 2010 where a retrospective study conducted by Bouhamdan et al. showed that the overall Toxoplasma seropositivity was 62.2% for IgG and 6.8% for IgM in the city of Beirut. Our retrospective study has focused on a case-series of pregnant women attending one specialized care center in Beirut, regrouping different age groups from the capital, its suburbs as well as its adjacent biggest governorate in Lebanon. The interest in that subgroup corresponds to the relatively high number of screened pregnant women, their age, and geographical representation and provides a recent and focused update on Toxoplasma infection among pregnant women.
Materials and Methods
This study was approved by the Institutional Review Board of the University of Balamand. This is a retrospective cohort study, in which medical records of 11,000 patients who visited a private Obstetrics and Gynecology clinic located in Beirut, the capital of Lebanon, during the period of January 1994 till September 2015 were screened. The clinic drains pregnant patients seeking antenatal care, from the city Beirut, its suburbs, and the immediately adjacent biggest governorate district of “Mount-Lebanon.” All medical records of pregnant women who underwent pregnancy serological examination of toxoplasmosis at any time during the studied timeframe period were included. Of the 11,000 screened medical records, only 2456 records fulfilled the inclusion criteria and were included in the analysis.
Gathered data included the patient's T. gondii serostatus, age, and region of residence of the patients. The results of IgG and IgM anti-Toxoplasma antibodies serological tests noted in the screened medical records of patients were obtained using enzyme-linked immunosorbent assay (ELISA) (Toxo IgM μ-Capture cat. no. 51119 and Toxo IgG cat. no. 51209; Human, Germany), avidity test of T. gondii-specific IgG antibodies or PCR analysis of the amniotic fluid as part of the patient's consultation, and follow-up at the corresponding time of their visit to the obstetrician. The presence of elevated levels of Toxoplasma-specific IgG antibodies indicates that the infection has occurred at some point, but does not distinguish between an infection acquired recently and one acquired in the distant past. In acute infection, IgM antibodies generally rise within 1–2 weeks and remain positive for 7–8 months postinfection. Detection of Toxoplasma-specific IgM antibodies has been used as indicative of seroconversion when the IgG levels were previously negative. A negative IgM with a positive IgG result indicates infection lasting at least since 1 year. Any IgG titer exceeding 5 IU/mL was considered positive according to the ELISA manufacturer.
All medical records of pregnant women were screened retrospectively for anti-T. gondii IgG and IgM antibodies serological results. When screening the medical records, women whose serological tests indicated IgG+ and IgM−, upon presentation, were classified as such in the flow diagram and were categorized in the Toxoplasma seropositive category (Fig. 1). When, upon presentation, the results of IgG and IgM of a patient were detected seronegative, anti-T. gondii IgG and IgM tests were repeated as a follow-up at a frequent basis and at different time points throughout pregnancy to detect any change in serostatus. The results of the follow-up subsequent to anti-T. gondii IgG and IgM tests were considered for classification as follows: (1) if all subsequent results throughout a woman's pregnancy history show seronegative IgG and IgM, the woman was categorized as a T. gondii seronegative pregnant woman; (2) if subsequent results throughout a woman's pregnancy history indicated a seroconversion, at any point in time, detected through seropositive IgG and IgM results (IgG+ and IgM+) or a seropositive IgG and a seronegative IgM (IgG+ and IgM−), the woman was classified accordingly in the Toxoplasma seroconverted category, with seroconversion occurring within the same pregnancy or between pregnancies; respectively. In more details, when upon presentation, the results of IgG and IgM were detected both seronegative (IgG− and IgM−) at first but then seropositive IgG and seronegative IgM (IgG+ and IgM−) appeared in subsequent pregnancies, we assumed that the seroconversion occurred between the pregnancies and thus the positive state of IgM was not captured due to lack of monitoring during this period when the woman is not pregnant. The count of the overall anti-T. gondii IgG seropositivity among Lebanese pregnant women included all women whose serological results of IgG were captured positive at any point in time.
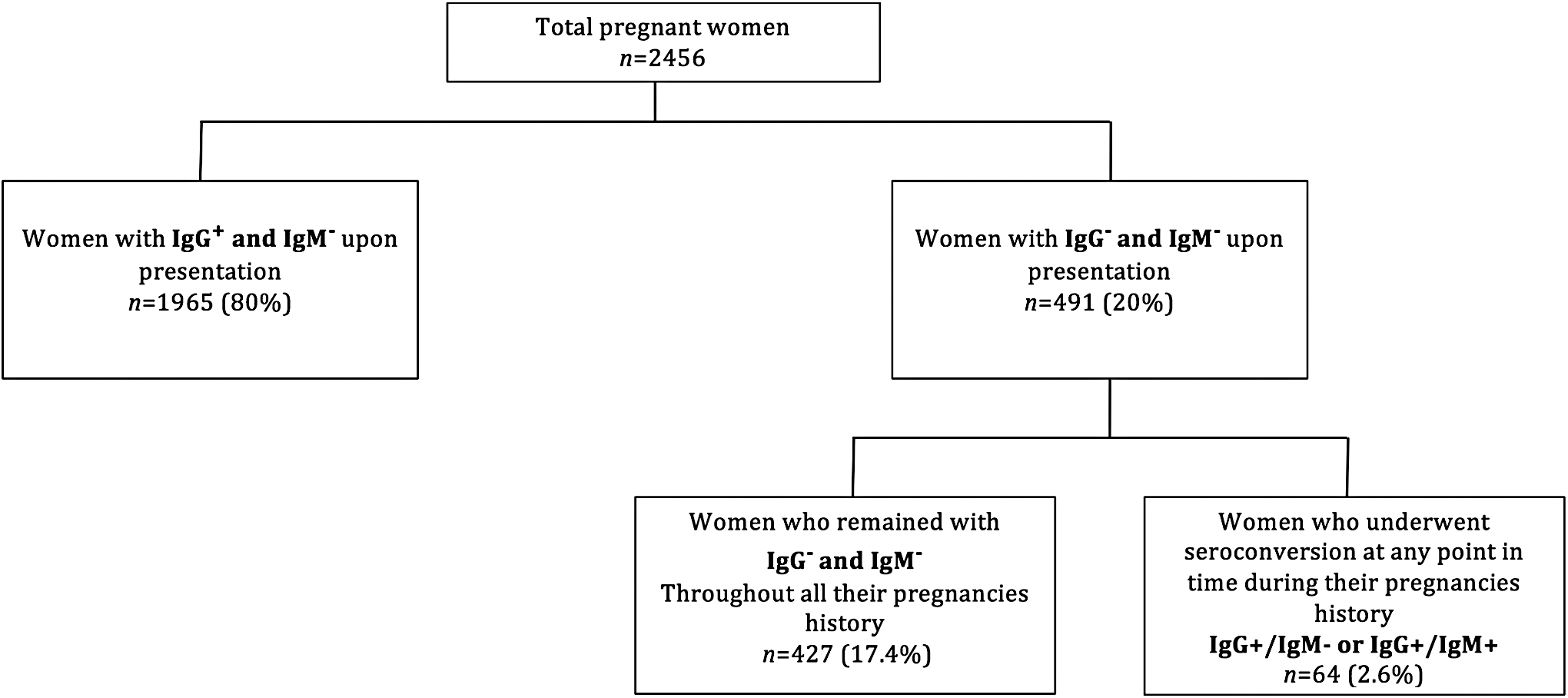
Diagram of the patients tested classified based on their Toxoplasma gondii serological results.
As for the exclusion criteria, medical records of patients who were never pregnant and visited the clinic for gynecology consultation solely, or those among pregnant women who did not undergo serological examination of toxoplasmosis were excluded. Thus, from a total of 11,000 medical records, only 2456 records were included. When studying the distribution of seropositivity over the three governorates of Lebanon (i.e., Beirut, North and Mount Lebanon), the serological results of women residing in regions or cities that do not belong to these governorates were also excluded. As for the study of seroprevalence among different age groups, the serological results of women whose age was not indicated were excluded. All of the 2456 women fulfilled the inclusion criteria for the study of the seropositivity distribution among age groups. Only 2249 women fulfilled the inclusion criteria for the study of the seropositivity distribution on the three governorates. A descriptive analysis was conducted and recorded in absolute numbers and percentages. The odds ratios and its 95% confidence interval were calculated. Inferential analysis was done using STATA software version 10.
Results
Upon presentation, out of 2456 pregnant women tested for seroprevalence of T. gondii, 1965 (80%) were seropositive for anti-T. gondii IgG antibodies and seronegative for anti-T. gondii IgM antibodies (IgG+ and IgM−), while 491 (20%) pregnant women were seronegative for both anti-T. gondii IgG and IgM antibodies (IgG− and IgM−) (Fig. 1). Among these 491 women, 427 (17.38%) remained seronegative for both IgG and IgM (IgG− and IgM−) throughout their pregnancies while 64 (2.6%) women underwent seroconversion to a positive anti-T. gondii IgG (Fig. 1). Eighteen women out of the 64 who underwent seroconversion were detected to have positive anti-T. gondii IgG and negative anti-T. gondii IgM results (IgG+ and IgM−) presuming that the infection occurred between pregnancies (Fig. 2). Moreover, 46 women out of the 64 were detected as seropositive for both anti-T. gondii IgG and IgM antibodies (IgG+ and IgM+) showing that the infection occurred within the pregnancy (Fig. 2). Strikingly, and among all of the 64 women who underwent seroconversion, two aborted because of T. gondii infection during their pregnancy as confirmed by PCR on the amniotic fluid (Fig. 2 and not shown).

Diagram of seroconversions during pregnancy.
The distribution of anti-T. gondii IgG seropositivity among three different age groups of 10 years interval showed the highest prevalence (87.81%) among the pregnant women aged between 35 and 44 years, followed by those aged 15–24 years with an IgG seropositivity of 82.86% while 81.68% seropositivity was seen among the pregnant women aged 25–34 years (Table 1). As for the distribution of anti-T. gondii IgM seropositivity among the different age groups, the highest IgM seropositivity of 2.45% was recorded among the pregnant women aged between 15 and 24 years, followed by those aged 25–34 years with an IgM seropositivity of 1.78%, while the age group 35–44 years showed the lowest percentage of 1.43% (Table 1).
Data are given as n (%).
IgG, immunoglobulin G; IgM, immunoglobulin M.
The inclusion criteria for the study were set on the distribution of anti-T. gondii IgG and IgM seropositivity among the three Lebanese Governorates, Beirut, North, and Mount Lebanon. Among the 2249 pregnant women who fulfilled these criteria, the IgG seropositivity was 276 (81.18%), 41 (73.21%), and 1537 (82.95%) in the three Governorates, respectively (Table 2). As for the IgM seropositivity, anti-T. gondii IgM seropositivity in Beirut and Mount Lebanon were 5 (1.47%) and 39 (2.1%), respectively, while no cases of pregnant women seropositive for IgM was seen in North (Table 2).
Data are given as n (%).
N/A, not applicable.
Discussion
Congenital toxoplasmosis occurs in fetuses upon a primo-infection of a pregnant woman with T. gondii. According to the trimester of infection, it does not only cause miscarriage or stillbirth but also serious and progressive visual, hearing, motor, and cognitive complications in a born child. A crucial step in antenatal care is the detection of T. gondii infection in the pregnant mother and her fetus. Cases showing seronegative results for both anti-T. gondii IgG and IgM antibodies in pregnant women care get intensive attention, where serological tests are repeated frequently throughout pregnancy to detect any development of primary acute infection that may result in miscarriage or vertical transmission of the parasite to the fetus (Tamer et al. 2009).
Our study is the first to investigate and update not only the status of Toxoplasma infection in pregnant women but also the rate of seroconversion and miscarriage due to this infection, in the Lebanese community. The importance of our study is entailed in its relatively large sample size of tested pregnant women in lights of absence of studies conducted in Lebanon on pregnant women to investigate the seropositivity of anti-T. gondii antibodies.
The overall anti-T. gondii IgG seropositivity among Lebanese pregnant women reaching 82.6% is extremely high. This may be due to the exposure to cats and cat's feces, drinking untreated contaminated water, and following some Lebanese dietary habits that favor the infection, as eating raw meat or improperly washed vegetables. The overall anti-T. gondii IgM seropositivity was determined as 1.8%. Furthermore, our study reports for the first time in Lebanon, two cases of abortion because of T. gondii following seroconversion of pregnant women during pregnancy. The stratification of the results on three different age group strata showed that the three age groups presented more or less similar prevalence of anti-T. gondii IgG seropositivity ranging between 81.68% and 87.81%, while anti-T. gondii IgM ranged between 1.43% and 2.45%. The anti-T. gondii IgG seropositivity was the highest among the eldest group, whereas the anti-T. gondii IgM seropositivity was the highest percentage in the youngest group, which suggests that the young population of pregnant women can be recognized as the population at risk of getting acute toxoplasmosis contrary to the eldest one who is mostly immune against T. gondii.
Compared to other countries of the Arab Region, the 82.6% seroprevalence of anti-T. gondii IgG among pregnant women in Lebanon is the highest in the region followed by 53.1% in Kuwait (Iqbal and Khalid 2007), 50.8% in Egypt (Kamal et al. 2015), and 34.1% in Sudan (Elnahas et al. 2003). The IgG seropositivity (82.6%) among pregnant women is even higher than that found in 2010 by Bouhamdan et al. who reported 62.2% IgG seropositivity in the total Lebanese population. However, the IgM seropositivity (1.8%) obtained in the results of this study is found to be lower than that reported by Bouhamdan et al. (2010) of 6.8%.
Potential reasons for the aforementioned difference in the results may be associated with the fact that the T. gondii seroprevalence in the study of Bouhamdan et al. (2010) was calculated based on data shared from six hospitals and five laboratories located all over Lebanon compared with data of this study that were based on information collected from only one private Obstetrics and Gynecology clinic. The geographical location of this clinic in Beirut interferes with the generalizability of this study. Besides, Bouhamdan et al. (2010) did not mention the criteria of positivity that was used in the study and the mean value above which the serological results were considered positive remained unspecified. A difference in the mean value used as a cutoff point above which results were counted as seropositive in Bouhamdan et al.'s (2010) study compared with this study, may thus be also considered as a potential source of discrepancies of the obtained results.
In fact, a main limitation of this study is that it does not target a representative sample where a selection bias is worth noting due to the nature of the catchment area in this particular clinic included in our study. Nevertheless, the result of our study may still be epidemiologically reflective of the population of pregnant women in Lebanon, highlighting, therefore, the need for a national sample survey estimating the real burden of this infection in pregnant women.
On the international level, several European countries as well as the United States of America are currently tilted toward a lower seroprevalence trend (Pappas et al. 2009). Among these countries, Lebanon still possess the highest seroprevalence compared with 21% in Spain (Bartolomé Álvarez et al. 2008), 19.8 in Italy (Masini et al. 2008), 9.1% in United Kingdom (Nash et al. 2005), and 11% in the United States (Jones et al. 2007). The relatively high seroprevalence rate in the Arab region generally and in Lebanon specifically, compared with the European countries and the United States, may be attributed, as previously discussed, is due to the dietary habits of the Arab countries as including raw meat, improperly washed vegetables, and untreated drinking water in addition to the high abundance of cats in Lebanon.
Conclusions
In conclusion, this descriptive study provides key and updated baseline data about the seroprevalence of anti-T. gondii antibodies among Lebanese pregnant women. Nonetheless, further epidemiological studies need to be conducted to investigate the association between toxoplasmosis and its risk factors, including age, region of residence, dietary habits, and other behavioral risk factors. The alarming rate of seroconversion suggests that prevention from T. gondii should be regularly addressed in the immediate environment of seronegative women. The reflective figures of this study emphasize the need for a national sample survey to estimate the real potential burden of this infection on maternal and its impact on fetal health. This is crucial to identify the population at high risk and target it with effective control and preventive measures.
Footnotes
Author's Contribution
H.N. has conceptualized the study and significantly contributed to data collection, analysis, and write up. N.E.A. has conceptualized the study and significantly contributed to data collection, analysis, and write up. E.C. has supported the implementation of this study and provided feedback during the write up. E.A. has supported the implementation of this study and provided feedback during the write up. H.E.H. have conceptualized the study and led data collection, analysis, and write up efforts.
Author Disclosure Statement
No competing financial interests exist.