
Abstract
Mycoplasma pulmonis is a naturally occurring respiratory pathogen in rodents. To date, this pathogen was not isolated from humans. This study aimed to evaluate the prevalence and seropositivity to M. pulmonis in humans who have had direct contact with rats. Moreover, the prevalence of M. pulmonis in pet and laboratory rats was assessed. Overall, 131 and 235 oropharyngeal swab samples were collected from human individuals and rats, respectively. In humans, M. pulmonis was detected by PCR in 21 of 86 pet rat keepers (24.42%), 10 of 13 technicians (76.32%), and 8 of 32 (25.0%) veterinarians. In rats, M. pulmonis was identified by PCR in 86 of 122 pet rats (70.49%) and 56 of 113 (49.56%) laboratory rats. Seroprevalence in humans was examined by screening sera from 44 individuals for M. pulmonis-specific IgG using ELISA. In total, 26 out of 44 (59.09%) humans were seropositive to M. pulmonis (4 out of 9 technicians, 8 of 12 veterinarians, and 15 of 23 pet rat keepers).The high antibody titer was found in 4 individuals (2 pet rat keepers and 2 veterinarians), whereas the moderate and low antibody titers were found in 8 and 14 individuals, respectively. The high antibody titer found in humans might indicate an active infection. However, it is unknown whether the presence of M. pulmonis in humans might be associated with disease and whether the foreign Mycoplasma can survive for long in its new environment.
Introduction
M
Although Mycoplasmas can infect a wide range of taxonomically diverse species, it is generally thought that majority of them are very host specific. To date, there was only one clinical case of M. pneumoniae transfer between humans and rodents (Mikola et al. 1997), whereas M. pulmonis has never been isolated from human oropharynx using standard, culture-based methods, thereby never diagnosed in humans. However, the interspecies transmission between rodents and humans might occur.
There are at least two factors that can favor the transmission of M. pulmonis to humans. Delgado and Timenetsky (2001) have shown that M. pulmonis can be recovered in high amount, ∼105 CFU/mL from tracheal aspirates of infected rats and in droplets of secretions generated during rat sneezing. Furthermore, M. pulmonis can be detected in rat throat for a long time, up to 248 days postinfection (van Kuppeveld et al. 1992). Thus, the prolonged exposure of humans to M. pulmonis that take place in rodent facilities might result in its transfer between rats and humans. Theoretically, a similar scenario might occur between pet rats and pet rat keepers who are in close, regular contact with these animals.
This study aimed to evaluate the prevalence and seropositivity to M. pulmonis in human individuals (pet rat keepers, technicians, and veterinarians) who have had a direct contact with the rats. Moreover, the prevalence of M. pulmonis in pet and laboratory rats was assessed.
Materials and Methods
Human and animal swab samples
To establish the prevalence of M. pulmonis in human individuals, a total of 131 oropharynx swab samples were collected (n = 86, pet rat keepers; n = 13, technicians; n = 32, veterinarians). Moreover, 235 swabs were also collected from pet and laboratory rats (n = 122, pets rats and n = 113, Winstar laboratory rats). The pet rats were kept in 62 private, small-scale breeding facilities (n = 1–5 rats/breeding), whereas the laboratory rats belonged to four different conventional breeding companies (n = 100–300 rats/facilities). The swab samples were collected using sterile flocked swab (FLOQSwabs™, Copan, Italy). The swab was introduced into the oropharynx, rotated, and held for 5 s to obtain maximum absorbency and then placed into a sterile test tube. The swabs were stored at −20°C until use.
Human sera samples
To further investigate the possibility of cross-species transfer, we performed ELISAs with 44 volunteers' sera collected from 23 pet rat keepers, 9 technicians, and 12 veterinarians who have had direct contact with the rats. The blood samples were taken through a catheter placed in an arm vein by qualified personnel at Jan Mikulicz-Radecki University Hospital in Wrocław (Poland).
Antimycoplasma IgG antibody titers in human sera were measured by human M. pulmonis Antibody IgG ELISA kit (MPAB-IgG) (MyBioSource, Canada) according to the manufacturer's instructions. Optical density (OD) was read at 450 nm using Asys Expert 96 microplate reader (Biochrom Ltd., United Kingdom). The existence of human MPAB-IgG in the samples was determined by comparing the OD of the samples to the cutoff (cutoff was calculated as the average of negative control well +0.15). The samples were negative when the OD was less than the cutoff value, whereas the samples were considered as a positive when the OD was greater than the cutoff value.
DNA isolation and PCR
DNA from oropharyngeal swab samples was extracted using Genomic DNA Prep Plus® kit (A&A Biotechnology, Gdynia, Poland) according to the manufacturer's instructions. The DNA concentration in each sample was measured by spectrophotometry (BioPhotometer, Eppendorf, Leipzig, Germany).
PCR was performed with M. pulmonis species—specific primers to 16S rRNA gene (MP1 5′- AGC GTT TGC TTC ACT TTG AA-3′ and MP2 5′- GGG CAT TTC CTC CCT AAG CT-3′) as described previously (Van Kuppeveld et al. 1992). The expected product size amplified by the primers was 266 bp. The PCR was set up in 25 μL of reaction mixture containing 50 ng of template DNA, 1 U DreamTaq Green DNA Taq polymerase (Thermo Scientific, Abo, Poland), 10× DreamTaq Green Buffer with 2 mM MgCl2 (Thermo Scientific, Abo, Poland), 200 μM dNTPs (Thermo Scientific, Abo, Poland), and 20 pmol of each primer (Genomed, Warszawa, Poland). PCR cycling was performed as follows: 40 cycles of 94°C for 1 min; 62°C for 1 min; 72°C for 1 min, with a final extension at 72°C for 5 min.
The PCR products were separated by electrophoresis in 1.5% agarose gel with Midori Green DNA Stain (NIPPON Genetics Europe GmbH, Abo, Poland) and observed using the Gel-Doc UV transilluminator system (Bio-Rad, Warszawa, Poland) with Quantity-One software (Bio-Rad, Warszawa, Poland). M. pulmonis (ATCC® 19612™) and M. pneumoniae (ATCC 15531™) were included in this study as controls for PCR.
Sequencing of PCR products
The PCR products obtained with primers MP1 and MP2 were Sanger sequenced by NZOZ Genomed (Warsaw, Poland). DNA sequences obtained after sequencing were assembled and the consensus sequences used to BLAST against the GenBank database (
Results
Prevalence of M. pulmonis in humans and rats
M. pulmonis was detected by PCR in 10 of 13 swab samples taken from technicians (76.32%), 8 of 32 (25.0%) veterinarians, and 21 of 86 pet rat keepers (24.42%). In rats, M. pulmonis was found in 56 out of 113 laboratory (49.56%) and 86 out of 122 pet rats (70.49%) (Table 1). The results demonstrated that consensus sequences of M. pulmonis from human oropharynx represent high similarity to the 16S rRNA of M. pulmonis sequence available in Genebank (AF125582, JN935865.1, NR113692.1, AL445565.1, NR041744.1).
Seroprevalence of M. pulmonis in humans
Overall, 26 out of 44 (59.09%) human's sera were seropositive to M. pulmonis. This includes 4 out of 9 technicians, 8 of 12 veterinarians, and 15 of 23 pet rat keepers. The high antibody titer, with OD >1, was found in 4 individuals (2 pet rat keepers and 2 veterinarians), whereas moderate and low antibody titers were found in 8 and 14 individuals, respectively (Fig. 1).
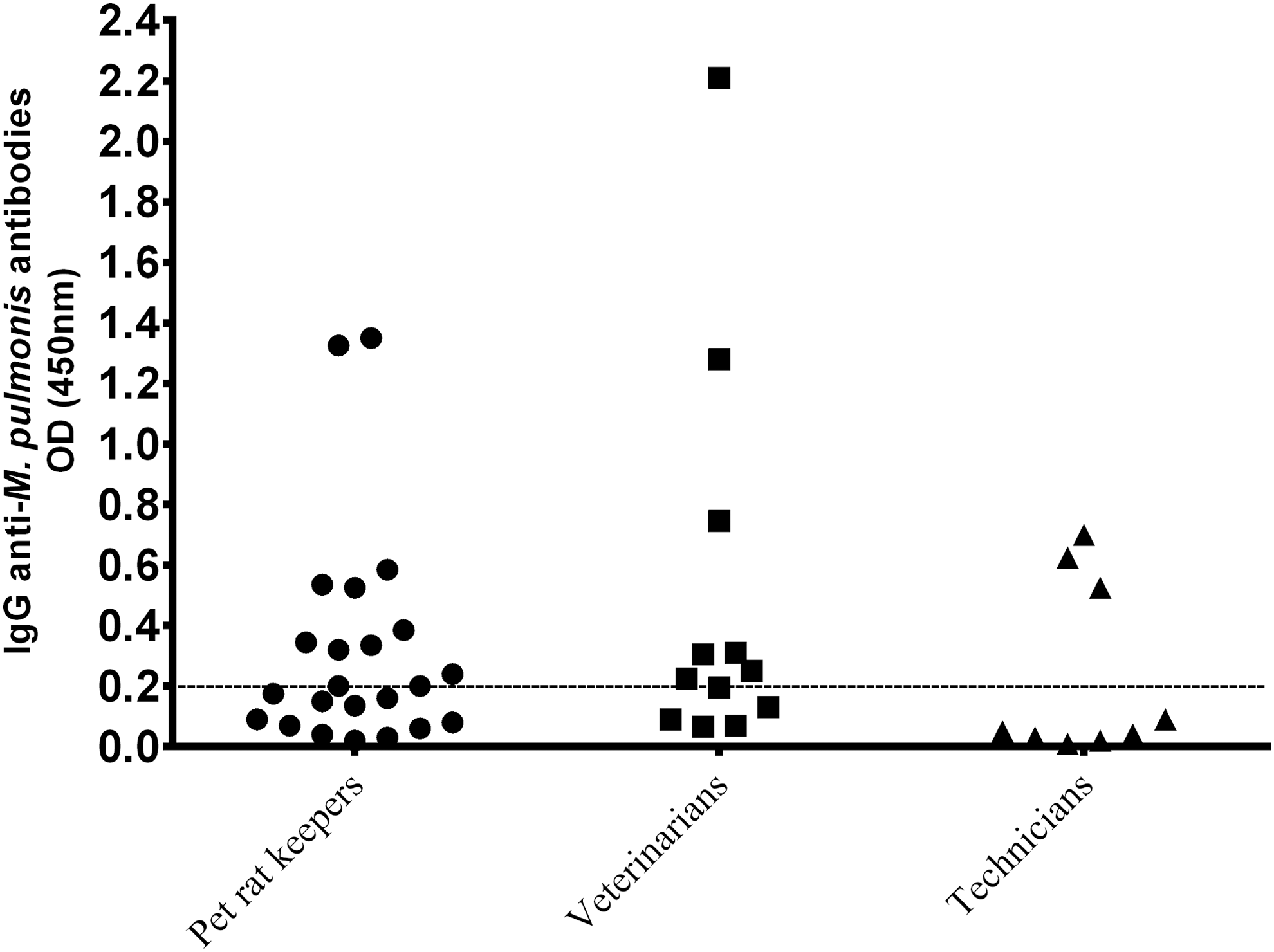
ELISA IgG anti-Mycoplasma pulmonis titer in human sera samples. The dashed vertical line indicates 0.15 cutoff value. Samples with OD greater than cutoff value were considered as positive. OD, optical density.
Discussion
M. pulmonis is a naturally occurring respiratory pathogen in rats and mice. These animals act as carriers of the organism, spreading the bacteria during close contact or as aerosols through the air. The expression of M. pulmonis infections in rats varies greatly. Most frequently, the murine respiratory mycoplasmosis is a chronic disease and occurs without clinical signs, which means it might escape clinical attention and possess a risk of M. pulmonis transmission. The prevalence of M. pulmonis in laboratory rats varies significantly, from around 3% (Schoondermark-van de Ven et al. 2006, Mähler and Köhl 2009) to almost 100% (Barreto et al. 2002). In this study, a high prevalence of M. pulmonis was found in rats in Poland ranging from 49% in laboratory rats to 70.5% in pet rats.
The high prevalence of M. pulmonis in rats corresponded with a high prevalence of M. pulmonis in technicians working with infected animals. Previously, M. pulmonis was detected only once in 12 human individuals (technicians of a laboratory animal household) who were in contact with infected rats (Ferreira et al. 2008). In this study, M. pulmunis was also found in almost 25% of pet rat keepers and veterinarians. The presence of M. pulmonis in humans might indicate that M. pulmonis has the ability to colonize the human oropharynx. However, it is unknown whether the presence of M. pulmonis in humans is associated with the disease. Interestingly, in this study, almost 60% of healthy individuals who have had direct contact with infected rats were seropositive to M. pulmonis. Although no human individuals reported any clinical signs of respiratory disease, the high IgG anti-M. pulmonis titer found in humans may indicate an active infection.
For many years, it was believed that M. pulmonis is highly host specific and to date this pathogen has never been isolated from human oropharynx using culture-based methods. However, the host may simply be the species in which M. pulmonis is the most frequently detected. A human oropharynx usually harbors human-origin mycoplasmas, thereby it is difficult to isolate murine-origin mycoplasmas in the human oropharynx; therefore, it can be overlooked during medical examination. Furthermore, the immunomodulatory effect of the commensal bacteria in human airways (Henriksson et al. 2004) might be engaged in local immune defense and elimination of M. pulmonis from human oropharynx until the agent can be identified. The relevant questions are whether M. pulmonis can survive for long in its new environment and whether the presence of M. pulmonis in humans might be associated with disease. This needs to be further evaluated.
Conclusion
In this study, a high prevalence of M. pulmonis in humans and rats was shown by PCR screening. Furthermore, more than 50% of humans with regular contact with infected rats were seropositive to M. pulmonis. Although none of the human individuals reported any syndromes of disease, the high IgG antibody titer found in four individuals might suggest an active infection.
Footnotes
Author Disclosure Statement
No competing financial interests exist.