
Abstract
Introduction:
Kyasanur forest disease (KFD) outbreak was confirmed in Dodamarg Taluka, Sindhudurga district (Maharashtra) in India during the year 2016. The rise in suspected KFD cases was reported in January 2016, peaked during March, and then declined gradually from April 2016. The outbreak was thoroughly investigated considering different socio-clinical parameters.
Methods:
Total, 488 suspected KFD cases were investigated using KFD specific real-time RT-PCR and anti-KFDV IgM enzyme-linked immunosorbent assay (ELISA). Sero-epidemiological survey was carried out in the affected area using anti-KFDV IgG ELISA.
Results:
Among suspected KFD cases, high age-specific attack rate (105.1 per 1000 persons) was observed in adults (aged 40–59 years). Out of 488 suspected KFD cases, 130 were laboratory confirmed. Of these, 54 cases were KFDV real-time RT-PCR positive, 66 cases were anti-KFDV IgM ELISA positive and 10 cases were positive by both the assays. Case fatality ratio among laboratory-confirmed KFD cases were 2.3% (3/130). Majority of laboratory-confirmed KFD cases (93.1%) had visited Western Ghats forest in Dodamarg for activities like working in cashew nut farms (79.8%), cashew nut fruit collection (76.6%), collection of firewood (68.5%) and dry leaves/grass (40.3%), etc., before the start of symptoms. Common clinical features included fever (100%), headache (93.1%), weakness (84.6%), and myalgia (83.1%). Hemorrhagic manifestations were observed in nearly one-third of the laboratory-confirmed KFD cases (28.5%). A seroprevalence of (9.7%, 72/745) was recorded in KFD-affected area and two neighboring villages (9.1%, 15/165). Serosurvey conducted in Ker village showed clinical to subclinical ratio of 6:1 in KFD-affected areas.
Conclusion:
This study confirms the outbreak of KFD Sindhudurg district with 130 cases. Detection of anti-KFDV IgG antibodies among the healthy population in KFD-affected area during the KFD outbreak suggested the past exposure of KFD infection. This outbreak investigation has helped health authorities in adopting KFD vaccination strategy for the population at risk.
Introduction
K
KFD outbreak was confirmed for the first time on January 21, 2016 from Ker village, Dodamarg taluka, Sindhudurg district, Maharashtra state through joint efforts of National Institute of Virology (NIV), Pune and state health authorities (Awate et al. 2016). Further, NIV, Pune had investigated the outbreak in detail in the region along with state health authorities to characterize the outbreak in terms of its timing, place and person distribution, clinical profile of KFD cases, clinical and subclinical ratio. Sero-survey of KFD was also conducted in Ker village to understand whether, KFD was present in this area before the present outbreak.
Materials and Methods
Study area and ecological features
Dodamarg taluk in Sindhudurg district, Maharashtra, is situated in Western Ghats region of India, between latitudes 15° 37′ N to 15° 60′ north and longitudes 73° 19′ E and 73° 40′ east. The Western Ghats, also known as Sahyadri is a mountain range that runs parallel to the western coast of the Indian peninsula. It is a UNESCO World Heritage Site and one of the eight “hot-spots” of biological diversity in the world. Dodamarg shares boundary with Karnataka (toward East) and Goa State (toward South). The population of Dodamarg is around 52,000 (residing in 58 villages). Health services to this population are provided by three primary health centers (PHC)—Morgan, Sateli-Bhedshi, Talkat, and the rural hospital at Dodamarg. Almost 40–50% of the area in this taluk is hilly and covered with tropical evergreen forest with the thick undergrowth of bushes and shrubs with climate being generally moist and humid. The annual average rainfall ranges from 3000 to 6000 mm. Red-faced macaque monkeys (Macaca radiate) habitat is known to cover the whole taluka, but black monkeys (Semnopithecus entellus) are also predominantly observed.
Epidemiological and clinical investigations
In the study area, list of suspected KFD cases was prepared from monthly surveys conducted by health workers, patient's records available in private/government hospitals or health centers during the investigation period (December 2015–July 2016). House-to-house survey was carried out by health workers (state health authorities) by monthly visits to each house (February–June 2016) with inquiries of fever and other symptoms so as to identify suspected KFD cases prospectively. Suspected KFD cases recorded in the month of December 2015 and January 2016 were also line-listed (retrospectively) from the available health records with healthcare workers. Line-list of suspected KFD cases was updated and finalized by removing double entries of suspected KFD cases, considering its reporting from multiple sources.
Detailed epidemiological and clinical information was recorded in case report form for laboratory-confirmed KFD cases (130) identified by NIV, Pune. Case examination and clinical records available through discharge cards recorded clinical details of these cases. Epidemiological data include information regarding housing condition, occupation, exposure details, work conditions, and others. Work habits of the laboratory-confirmed KFD cases were also noted. Geographical information system tools were used for getting geo-coordinates of laboratory-confirmed KFD cases detected by NIV, Pune.
A suspected KFD case was defined as any person with the history of fever with one or more symptoms: headache, body ache, myalgia, vomiting, diarrhea, skin rash, any hemorrhagic manifestation, neurological symptoms, and living in villages in a forest in Dodamarg taluka, Sindhudurg district during December 2015–July 2016. The definition of KFD confirmed case followed was; a case, which was found positive either by KFD real-time RT-PCR or by Anti-KFD immunoglobulin M (IgM) enzyme-linked immunosorbent assay (ELISA) or with both the assays were considered as laboratory-confirmed KFD cases.
Specimen collection and laboratory tests
Among line listed suspected KFD cases (2306), blood samples (2–3 mL) were collected from suspected KFD cases (488). These cases (488) were reported at primary health centers (Talkat, Sateli-Bhedshi, Morgaon) and the rural hospital (Dodamarg) and serosurvey activity (February 23–March 3) during the outbreak investigation period. Blood samples were transported to NIV, Pune. The sera were separated, aliquoted, and tested for KFD on the basis of postonset day (POD) of symptoms. During the diagnosis, 0.140 mL blood/serum was used for RNA extraction using Qiagen RNA extraction kit, followed by KFD real-time RT-PCR, which was set up by targeting the NS-5 gene as described earlier (Mourya et al. 2012). For screening of IgM antibodies from suspected KFD cases, serum samples were tested by an indigenously developed Anti-KFD IgM ELISA using the inactivated KFDV antigen and biotinylated antibodies as per protocol described earlier (Mourya et al. 2012). For screening samples of sero-survey collected from the study site, Anti-KFDV immunoglobulin G (IgG) ELISA was performed. In this indigenously developed ELISA, polystyrene microwells were coated with inactivated KFD antigen (Rows A–D) and control antigen (Rows E–H). One hundred microliter of diluted human serum samples and controls were incubated in respective wells to allow specific antibody present in the samples to react with the antigen. Peroxidase-conjugated anti-human IgG was added and allowed to react with specific IgG. Nonspecific reactants were removed by washing, following which enzyme substrate was added and the color was allowed to develop. After adding the stop solution, the intensity of color/optical density (O.D.) was measured at 450 nm. Cutoff criteria for IgG assay was calculated based on the P/N ratio (O.D. of the sample with positive antigen/O.D. of samples with control antigen). The sample was considered positive if P/N ratio is >3.0 and O.D. with positive antigen >0.2 (Mourya et al. 2012).
The ELISA has been checked for the specificity using the panel of IgG antibodies from positive and negative human serum samples against Japanese encephalitis, West Nile, Dengue virus (DENV), and Leptospira samples. With this, cross-reactivity was also tested with positive and negative rheumatoid factor samples. None of them showed any cross-reactivity; Dengue IgG-positive samples showed 20% cross-reactivity, which is common across the flaviviruses.
Acute phase (≤3 days) sera (151) were screened only for KFDV real-time RT-PCR and sera (241) between POD 4 and 14 were screened for both KFDV real-time RT-PCR and anti-KFDV IgM antibodies. Sera with POD >14 was screened only for anti-KFDV IgM antibodies (96). Randomly collected sera from a subset of suspected KFD cases (139) were screened for anti-KFDV IgG antibodies. Peripheral blood smears collected by health workers from all suspected febrile cases (2306) were tested for malaria parasites at primary health centers. During the early phase of outbreak, (January–February 2016), among 51 reported suspected KFD cases, sera were screened for both anti-DENV IgM antibodies and anti-CHIKV IgM antibodies (33), only anti-DENV IgM antibodies (12) and only anti-CHIKV IgM antibodies (7) by ELISA (Gadkari and Shaikh 1984, Hundekar et al. 2002). Laboratory investigation reports like complete blood count, liver function test, kidney function tests, and so on performed on laboratory-confirmed KFD cases (36) admitted in hospitals and diagnosed by NIV were recorded from available discharge cards.
Seroepidemiological survey
The seroepidemiological survey was conducted in the KFD affected and unaffected areas during the early phase of the outbreak (February 23–March 3 2016). Blood samples (2–3 mL) were collected from healthcare staff from PHC (30) and forest guards/workers (18), KFD affected villages (Ker [288], Asaniye [169], Zolambe [75], and Kolzar [165]), and control villages (control area) (Tamboli [93] and Nagartas [72]) from neighboring taluka Sawantwadi situated more than 15 km from affected area in Dodamarg. Collected sera were screened for anti-KFDV IgG antibodies as defined above. Epidemiological information was collected and recorded in the questionnaire.
In Ker village, during the early phase of the outbreak, among 288 individuals residing in the village at the time of serosurvey, sera from 276 individuals were tested for both anti-KFDV IgG antibodies and anti-KFDV IgM antibodies for determining the clinical and subclinical ratios. Among susceptible individuals for KFDV infection (i.e., subjects negative for anti-KFDV IgG antibodies and anti-KFDV IgM antibodies) in Ker village, the clinical and subclinical ratios were calculated.
Ethical issues
Informed consent was obtained from patients and healthy individuals in KFD-affected area and in control area before the specimen collection. The institute's Human Ethics Committee at the NIV, Pune reviewed and approved the investigations (NIV/IEC/2017/D-43).
Statistical analysis
The age-specific attack rates for suspected KFD cases and case fatality ratio for laboratory-confirmed KFD cases was calculated. The Chi-square (χ 2) test was used to compare the clinical symptoms between laboratory-confirmed KFD cases and those negative for KFD. Confidence interval (CI) and p-value were calculated.
Results
Epidemiological investigation
Among 2306 suspected KFD cases, health workers considered 1774 through the house-to-house survey and 532 were recorded at private/government clinics/hospitals. The rise in suspected KFD cases was reported in January 2016, peaked during March, and then declined gradually from April (Fig. 1). Majority (83.1%, 1917/2306) of the cases were reported between January and May (Fig. 1). The overall attack rate of suspected KFD cases was 7.6% (2306/30439) (Table 1). The attack rate of suspected KFD cases varied from 2.1% to 36.6% among the villages. Suspected KFD cases were reported from villages; Kendre (36.6%), Ker (22.1%), Asaniye (21.4%), Zolambe (18.3%), Fukeri (14.4%), Kolzar (10.8%), and Talkat (10.8%) (Table 1).
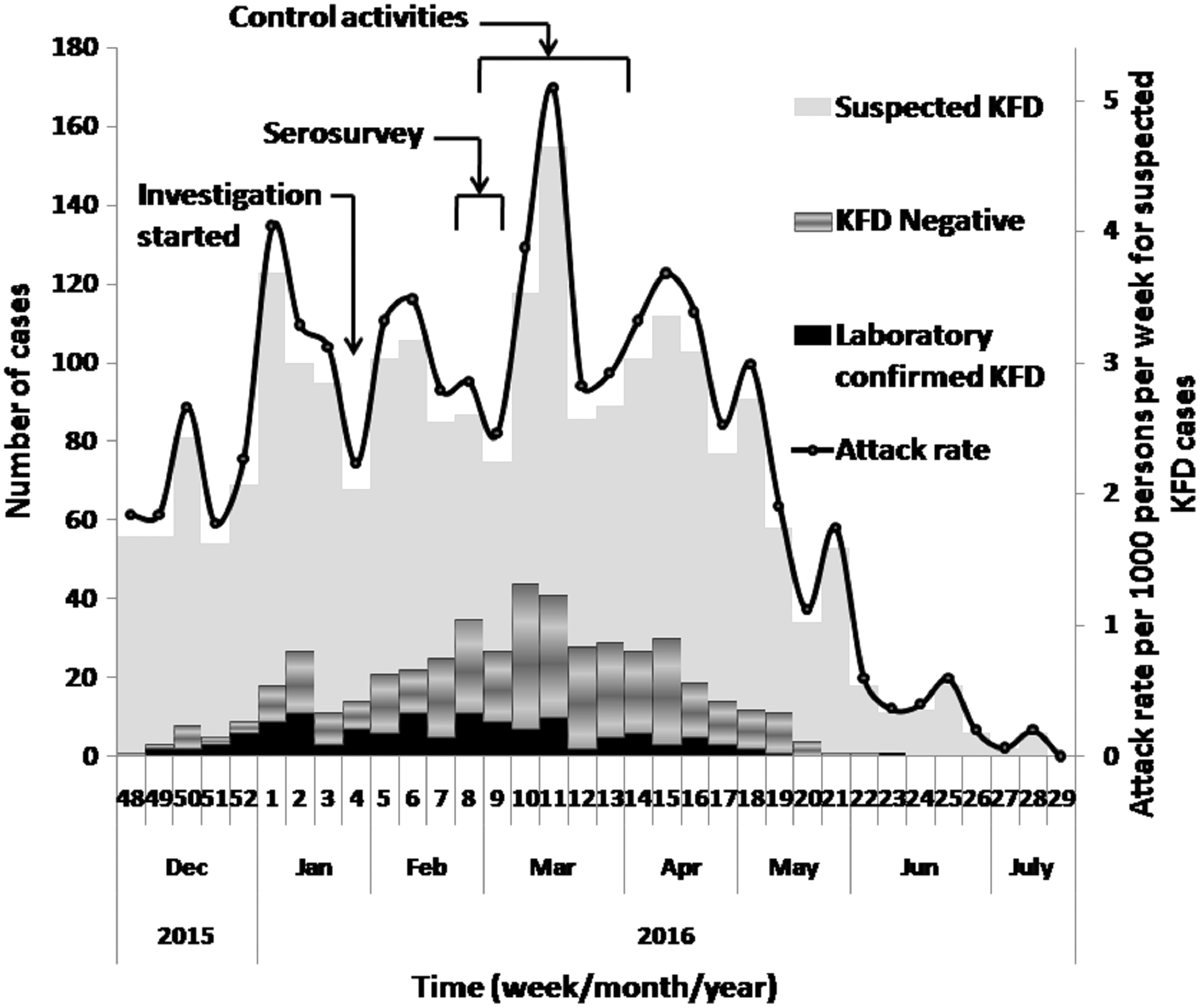
Weekly distribution of suspected Kyasanur forest disease cases showing Kyasanur forest disease viral etiology and attack rate during the investigation period (December 2015–July 2016).
KFD, Kyasanur forest disease.
Clustering of laboratory-confirmed KFD cases was observed in Ker village (Fig. 2). In Ker village, 47 cases were reported from 30 houses (4 cases each from 3 houses, 3 cases each from 4 houses, 2 cases each from a house, and 1 case each from 21 houses). Among KFD-affected villages (Table 1), at least one laboratory confirmed KFD case was reported from each affected house.

Distribution of laboratory-confirmed Kyasanur forest disease cases in the study area during the investigation period (December 2015–July 2016).
Age wise distribution of suspected KFD cases with age-specific attack rate is shown in Table 2. The majority (61.8%, 1426/2306) of suspected KFD cases were in the age group 20–59 years. Among suspected KFD cases, high age-specific attack rate (105.1 per 1000 persons) was observed among adults (aged 40–59 years). In suspected KFD cases, high attack rate (89.5 per 1000 persons) was observed in women (Table 2). Majority of KFD cases (93.1%) had visited Western Ghat forest in Dodamag and were involved in occupation like working in cashew nut farm (79.8%), cashew nut fruit collection (76.6%), collection of fire wood (68.5%) and dry leaves/grass (40.3%), and so on. (Table 3).
Seroepidemiological survey
Seroprevalence of anti-KFDV IgG antibodies was high in Ker village (17.4%, 50/288) as compared to other KFD-affected villages that is, Asaniye (9.5%, 16/169), Zolambe (5.5%, 4/75), and Kolzar (1.2%, 2/165) (Fig. 2). In control area, seropositivity was higher in Tamboli (12.9%, 12/93) as compared to Nagartas (4.2%, 3/72). Among the population (including forest guard/workers) living in KFD-affected area, seroprevalence of anti-KFDV IgG antibodies was high (14%, 21/150) among elderly (age ≥60 years), adults aged 40–59 years (13.2%, 34/257), and young adults aged 20–39 years (7.9%, 14/178) as compared to adolescents age group 10–19 years (1.7%, 2/115) and ≤10 years children (2.2%, 1/45). In two neighboring villages (Tamboli and Nagartas) seroprevalence of anti-KFDV IgG antibodies was high (16.2%, 6/37) among elderly (age ≥60 years), adults aged 40–59 years (11.1%, 5/45), and young adults aged 20–39 years (11.8%, 4/34). No anti-KFDV IgG antibodies were detected among adolescent's age group 10–19 years (31) and ≤10 years children (18) in these two villages. Anti KFDV IgG antibodies were also not detected among healthcare staff from PHC (30) and forest guards/workers (18). Overall seropositivity for anti-KFDV IgG antibodies in KFD-affected area (9.7%, 72/745) and two neighboring villages (9.1%, 15/165) was similar.
In Ker village, among 276 individuals, 50 were positive for anti-KFDV IgG antibodies and negative for anti-KFDV IgM antibodies, suggesting past history of KFD infection. Thus, 226 individuals were susceptible to KFD infection. Among these 226 individuals, 42 were positive for anti-KFDV IgM antibodies suggesting recent KFD infection. Among 42 cases, 36 were clinically suspected KFD cases showing clinical manifestations and 6 were asymptomatic, that is, subclinical infection. The ratio between confirmed KFD and subclinical KFD cases was found to be 6:1.
Clinical and laboratory investigations
Among total suspected KFD cases (21.2%, 488/2306) investigated, 237 were male and 251 were female. Out of screened 488 suspected KFD cases, KFDV etiology could be identified in 130 cases. Out of 139 samples screened, IgG antibody positivity was observed in 61 cases (Table 4). Percentage positivity of laboratory-confirmed KFD was 26.6 (130/488). Case fatality ratio for laboratory-confirmed KFD was 2.3% (3/130).
KFDV, Kyasanur forest disease virus; IgG, immunoglobulin G; IgM, immunoglobulin M.
Anti-CHIKV IgM antibodies were detected in five cases in the age group 18–65 years from Kolzar (2), Talkat (1), Ker (1), and Zolambe (1). Anti-DENV IgM antibodies were also detected from two cases in the age group 32–65 years from Ker (1) and Kolzar (1). Sera from 32 years male from Zolambe village showed specific reactivity to DEN and CHIKV antigen. The sera, which were positive for anti-DENV IgM antibodies or anti-CHIKV IgM antibodies, were negative for anti-KFDV IgM antibodies.
Among laboratory confirmed KFD cases (130), majority cases had headache (93.1%) followed by weakness (84.6%), myalgia (83.1%), and hemorrhagic manifestations (28.5%) (Table 2). Among laboratory confirmed KFD-positive (130) and KFD-negative (358) cases, no statistically significant differences were observed for the clinical symptoms like headache (121/130, 93.08% [CI 88.71–97.44] vs. 314/358, 87.71% [CI 84.31–91.11], p = 0.09), weakness (110/130, 84.62% [CI 78.41–90.82] vs. 319/358, 89.11% [CI 85.88–92.33], p = 0.17), myalgia (108/130, 83.08% [CI 76.63–89.52] vs. 312/358, 87.15% [CI 83.68–90.62], p = 0.17), bodayache (105/130, 80.77% [CI 73.99–87.54] vs. 286/358, 79.89% [CI 75.74–84.04], p = 0.82), vomiting (79/130, 60.77% [CI 52.38–69.16] vs. 201/358, 56.15% [CI 51.01–61.29], p = 0.36), and giddiness (69/130, 53.08% [CI 44.50–61.66] vs. 178/358, 49.72% [CI 44.54–54.90], p = 0.51).
The laboratory-confirmed KFD cases were treated initially at primary health centers. Among 100 hospitalized laboratory-confirmed KFD cases (76.9%, [100/130]), 52 were treated at primary health centers and 48 required referral (to tertiary healthcare centers). The average hospital stay of laboratory-confirmed KFD cases was 6 days (range 1–40 days). None of the patients had been vaccinated against KFD.
Laboratory investigation findings were available only from 36 KFD cases. (Supplementary Table S1; Supplementary Data are available online at
Among laboratory confirmed KFD cases, neutrophilic leukocytosis (38.9%, 14/36), thrombocytopenia (41.7%, 15/36), and normal serum electrolyte levels (serum sodium, serum potassium, and serum chlorides) were observed. However, liver function tests revealed that liver enzymes (serum glutamic oxaloacetic transaminase, serum glutamate pyruvic transaminase, and serum alkaline phosphatase) were raised among 22 (81.5%, 22/27) cases (Supplementary Table S1). The peripheral blood smears collected from suspected KFD cases (2306) were negative for the malaria parasite.
Control measures
As soon as the outbreak was confirmed by NIV, Pune, Maharashtra State health authorities notified the outbreak to whole community including local villages, central health authorities, and initiated vector control measures for ticks (5 km radius from monkey death hotspot) in coordination with forest and veterinary department in Dodamarg Taluka. Fever surveillance was strengthened in all the villages in forest area and neighboring PHCs were alerted. Health education was imparted to villagers by presentations and lectures regarding prevention of KFD from February 2016. The government of Maharashtra has procured dimethyl phthalate (DMP) oil (99.5%), a tick repellent and started distributing it to villagers from March 2016 with specific health education message regarding use of DMP oil and how to avoid tick bites.
Discussion
Dodamarg taluka in Sindhudurg district of Maharashtra state shares boundary with Goa State, where KFD cases were reported in the year 2015 from Pali and Satari (Department of Information and Technology, Government of Goa 2015). Laboratory confirmation of KFDV among cases in the present outbreak has raised alarm regarding the earlier presence of KFDV in the Western Ghats in Maharashtra. In addition, the detection of anti-KFDV IgG antibodies, in a substantial number of the population in the area, has suggested ongoing KFD infection for quite a long time in the area. Detection of anti-KFDV IgG antibodies among the healthy population in KFD-affected area during the KFD outbreak suggested the past exposure of KFD infection. In this study, the high seroprevalence of KFD in the KFD-affected area suggests that the population had been exposed to KFD infection before the present KFD outbreak. It is likely that the KFDV exists in other areas in cryptic enzootic cycles or is associated with the unrecognized or undiagnosed disease.
If we compare the magnitude of the KFD outbreak in Maharashtra with the KFD outbreaks in neighboring state Karnataka, during 2003–2012 in Karnataka, there were 3263 suspected KFD with 823 laboratory-confirmed KFD and 28 deaths and case fatality ratio was 3.4 (Holbrook, 2012) with KFD attack rate (4.4 per 1000 person) also observed in year 2014 (Kiran et al. 2015). Even, KFD attack rate per 1000 person in the age group 15–59 and ≥60 was much higher in a KFD outbreak in Shimoga (Kiran et al. 2015) as compared to present KFD outbreak in Maharashtra (Table 2). Though seroprevalence for anti KFDV IgG antibodies among KFD-affected villages varies, overall seroprevalence among KFD-affected area and neighboring area where no KFD cases were reported were similar. Seroprevalence of anti KFDV IgG antibodies among elderly was high (14–16.2%) as compared to other age groups. It suggests KFD activity was going on from last few years in the area and elderly are at risk of getting KFD infection.
Majority of laboratory-confirmed KFD cases in Dodamarg that had mild clinical symptoms were treated at PHC by medical officers. Though no hemorrhagic manifestation was observed in the first 28 laboratory-confirmed KFD cases from Ker village (Awate et al. 2016), hemorrhagic manifestations were recorded in subsequently reported laboratory-confirmed KFD cases. A cluster of KFD cases detected in Nagamala hills in the Nedumkayam Reserve Forest, Malappuram, Kerala also showed similar presentation (Tandale et al. 2015). However, in an outbreak of KFD in the year 2014 in Thirthahalli, Karnataka, India, no hemorrhagic manifestations and deaths were reported (Yadav et al. 2014).
In earlier KFD reported cases, the biphasic fever has been noted with neurologic symptoms like a severe headache, stiff neck, mental disturbance, coarse tremors, abnormal reflexes, and cerebro-spinal fluid (CSF) pleocytosis (Pavri 1989). Second episode of fever and neurologic manifestation in form of headache, altered sensorium, and convulsions were recorded among the laboratory-confirmed KFD cases in Dodamarg. The second episode of fever could possibly be due to a different infection, other than KFD. However, we could not confirm it through laboratory testing. During the early phase of the KFD outbreak, the serosurvey was done in the most affected village, Ker, recorded clinical to subclinical ratio 6:1. Among KFD cases, neutrophilic leucocytosis, thrombocytopenia, and raised level of liver enzymes were the prominent laboratory findings. Earlier also, liver involvement in KFD with raised liver enzymes has been reported (Banerjee 1978). In the present KFD outbreak, most of the cases had mild symptoms. Whenever acute febrile cases with comparable symptoms come to clinicians from forest region, physicians should consider KFD as a differential diagnosis so as to have further laboratory confirmation.
Most of the laboratory confirmed KFD cases were farmers and cattle grazers who use to visit forest many times and got tick bites. Chances of getting KFD by tick bites depend upon the number of factors related to infectivity of KFDV in ticks and ticks nymphal activity and population. The seasonality of KFD is related to the tick nymphal activity (Rajagopalan et al. 1968). The villagers in KFD-affected area are exposed to the bite of nymphs of the ticks during field activities. Without taking any precautions, villagers usually work in the forest, particularly during cleaning of ground under cashew nut trees (Anacardium occidentale) a tropical evergreen tree that produces the cashew seed and the cashew apple. Significant exposure to KFD infection seen in this outbreak was due to recent visit to the forest, domestic cleaning around own house, working in cashew nut farms, recent history of tick bite, and history of contact with domestic animals and cattle. Cattle constitute one of the decisive man-made factors that favor vector density at places most frequented by man, thus carrying all stages of different Haemaphysalis species, which might have been found infected with KFD virus (Boshell 1969). KFD is transmitted mainly by Haemaphysalis spinigera, however, other Haemaphysalis species such as H. turturis, H. uanakinneari, H. minuta, H. cuspidata, H. bispinosa, H. kyasanurensis, H. wellingtoni, and H. aculeate are also known for transmission of KFD (Banerjee 1988, Mourya and Yadav 2016).
District health authorities have initiated health education in all villages in the area from February 2016 regarding personal protection measures for avoiding tick bites. However, the actual distribution of tick repellent to villagers was little late in March 2016. Use of tick repellent was a new concept for the villagers and they also had difficulties in using these repellents. Other reasons would be the unavoidable visits of people to the forest, infrequent use of tick repellents for vector control, and incorrect use of personal protection measures. All these factors have reflected in the epidemic curve, which does not show any decline in the number of suspected KFD cases. However, we could not quantitatively measure these factors. Further, for effective control measures, health authorities should give sustainable health education to the people living in the forest so that they strictly use tick repellents along with personal protection measures (long clothes by covering neck, chest, back, and legs) before going to the forest. The population at risk from the area needs to be KFD vaccinated. Quick reporting of monkey deaths so as to initiate ticks control measures near hot spots along with effective coordination between health, veterinary, and forest department personnel.
Detection of anti-KFDV IgG antibodies among two villages in neighboring Taluka, Sawantwadi suggested that KFD might have been prevalent for quite a long time. However, KFD cases may not have been detected from these areas in earlier years, might be due to nonreferral of clinical specimens from fever cases to NIV, Pune (only laboratory facility in the region for detection of KFDV) for differential diagnosis of viral infections. The present KFD outbreak could have been detected earlier if clinical samples would have been referred to NIV, Pune in time. However, initiating tick control measures by health authorities in KFD-affected villages and near monkey death hot spots in the forest has helped to restrict the spread of KFD. Due to strengthened fever surveillance in the KFD-affected area, suspected KFD cases got prompt treatment in the early course of illness so as to curtail the morbidity and mortality due to KFDV.
The evidence generated during the investigation of KFD outbreak was used by public health authorities for preparing future strategies including administration of KFD vaccination to the population in the high-risk area for prevention of KFD in the Western Ghats.
Footnotes
Acknowledgments
We gratefully acknowledge the support rendered by Dr. Kanchan Jagtap, joint director and Dr. R.B. Mugade, Deputy Director (Kolhapur Circle) from Health Services, Govt. of Maharashtra. Authors would also like to thank Dr. Vidyanand Desai, livestock developmental officer, Taluka Mini Veterinary Polyclinic, Sawantwadi for support and help in sending the monkey autopsy specimens. The author acknowledges the contribution of the technical staff of Diagnostic Virology Group (Mr. B.N. Tilekar), Entomology (Mr. Sachin Dhaigude, Mr. V.S. Ghodke, and Mr. Praphulla Sonawane), Epidemiology group (Mr. A.K. Pande) for field and laboratory assistance. Authors are also thankful to all health staff from PHCs (Talkat, Sateli-Bhedshi and Morgaon) for the excellent teamwork. Financial support was provided from the Indian Council of Medical Research, New Delhi.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.