
Abstract
A lack of surveillance and diagnostics for zoonotic diseases in rural human clinics limits clinical awareness of these diseases. We assessed the prevalence of nine zoonotic pathogens in a pastoral, low-income, HIV-endemic community bordering wildlife reserves in South Africa. Two groups of participants were included: malaria-negative acute febrile illness (AFI) patients, called febrilers, at three clinics (n = 74) and second, farmers, herders, and veterinary staff found at five government cattle dip-tanks, called dip-tanksters (n = 64). Blood samples were tested using one PCR (Bartonella spp.) and eight antibody-ELISAs, and questionnaires were conducted to assess risk factors. Seventy-seven percent of febrilers and 98% of dip-tanksters had at least one positive test. Bartonella spp. (PCR 9.5%), spotted fever group (SFG) Rickettsia spp. (IgM 24.1%), Coxiella burnetii. (IgM 2.3%), and Leptospira spp. (IgM 6.8%) were present in febrilers and could have been the cause of their fever. Dip-tanksters and febrilers had evidence of past infection to Rickettsia spp. (IgG 92.2% and 63.4%, respectively) and C. burnetii (IgG 60.9% and 37.8%, respectively). No Brucella infection or current Bartonella infection was found in the dip-tanksters, although they had higher levels of recent exposure to Leptospira spp. (IgM 21.9%) compared to the febrilers. Low levels of West Nile and Sindbis, and no Rift Valley fever virus exposure were found in either groups. The only risk factor found to be significant was attending dip-tanks in febrilers for Q fever (p = 0.007). Amoxicillin is the local standard treatment for AFI, but would not be effective for Bartonella spp. infections, SFG rickettsiosis, Q fever infections, or the viral infections. There is a need to revise AFI treatment algorithms, educate medical and veterinary staff about these pathogens, especially SFG rickettsiosis and Q fever, support disease surveillance systems, and inform the population about reducing tick and surface water contact.
Introduction
Z
Studies in sub-Saharan Africa investigating acute febrile illness (AFI) patients have found evidence of present or past zoonotic infections (Table 1). In populations with a high prevalence of HIV infection, this proportion of zoonotic infections may be even higher due to immunosuppression; HIV also increases the clinical severity of many zoonoses and results in a more protracted, chronic illness (Froberg et al. 2004, Biggs et al. 2011).
Microscopic agglutination test.
immunofluorescent assay.
SFG, spotted fever group.
A lack of human surveillance for zoonotic diseases (Rodríguez-Prieto et al. 2015) and laboratory capacity causes a lack of clinical awareness, leading to underdiagnosis and consequently mismanagement of cases (John et al. 2008). In this light, the early detection of new and reemerging human pathogens is also problematic (Zumla et al. 2016). Gaps in data on the burden of zoonotic infections are especially pressing in the study site, a pastoral setting where humans, their domestic animals, and wildlife have frequent direct and indirect contact. The zoonoses selected for this study were based on prior information concerning infection prevalence and laboratory capacity. The study aimed to document the prevalence of nine zoonoses in this setting; investigate the proportion of AFI patients and high-risk cattle farmers, herders, and veterinary staff who have evidence of exposure or infection to these zoonoses; and identify risk factors for these zoonoses. Implications for public health surveillance, and diagnostic and treatment protocols used in this setting are explored.
Materials and Methods
Study site
The study was implemented in three rural government primary healthcare clinics and five government cattle dip-tanks in Bushbuckridge Municipality, Mpumalanga Province, South Africa (Fig. 1). The prevalence of HIV infection in the province is 14.1% (Shisana et al. 2014).
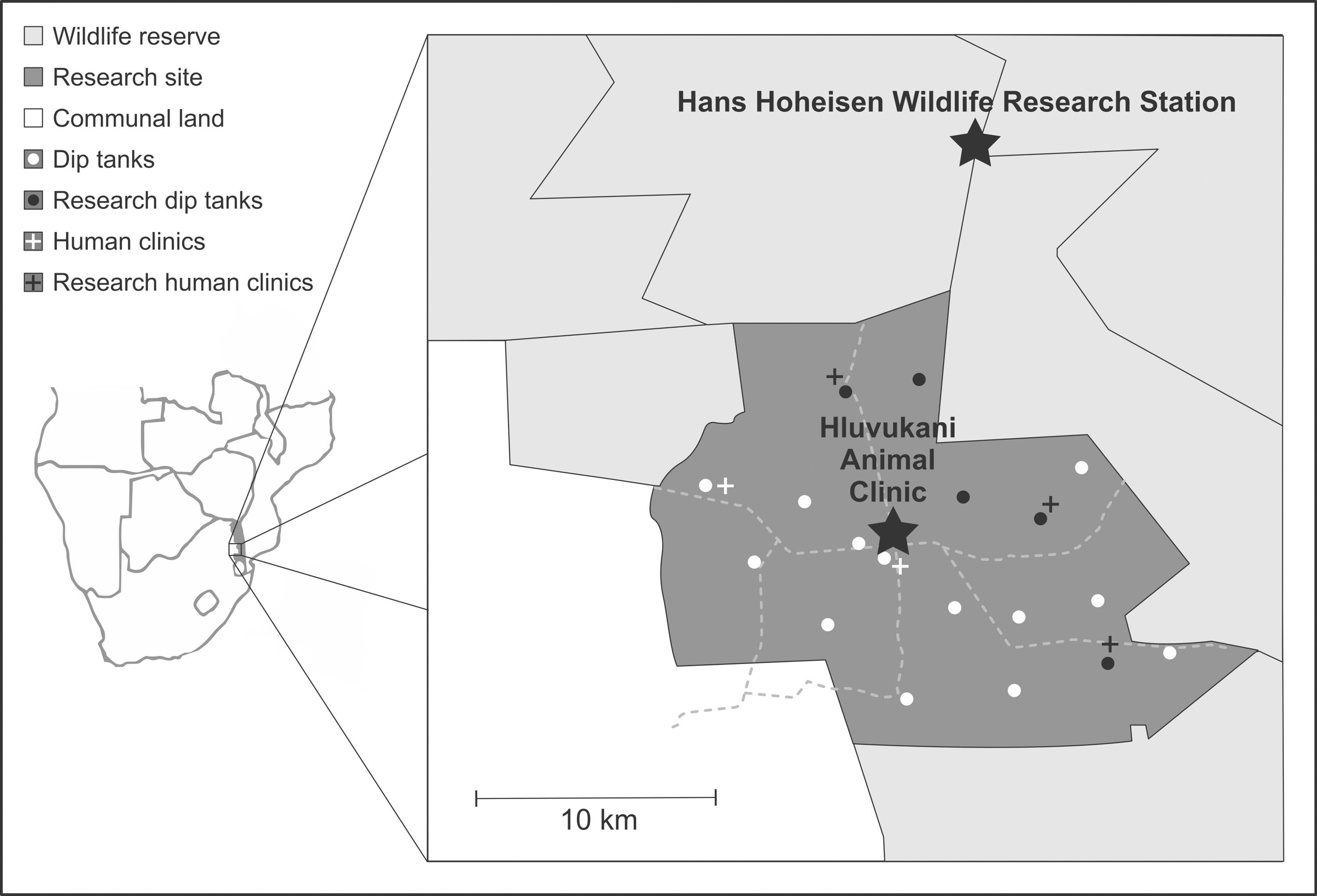
Map of the study site with clinics and dip-tanks used for sampling. Location of the research site, Bushbuckridge Municipality, Mpumalanga Province, South Africa.
The study area was in the Mnisi Community Programme area, containing the Hans Hoheisen Wildlife Research Station and Hluvukani Animal Clinic, and is a joint initiative by the University of Pretoria with the Mpumalanga Veterinary Services and the Mnisi Traditional Authority to promote sustainable livelihoods through research into human and animal health, animal production, and natural resource utilization. Approximately 40,000 people live in 8500 households (Statistics South Africa [SSA] 2012), with 72% of all households owning at least one species of animal and agro-pastoralist farming being the primary subsistence activity (Berrian et al. 2016). Chickens are owned in 55% of households, cattle in 25%, goats in 16%, pigs in 5%, and companion animals in 36% (Berrian et al. 2016). The community shares three-quarters of its boundary with wildlife reserves. In the communal area, there are hares, small antelope, rodents, and small carnivores, and in the wildlife reserves, all wildlife typical of “big five” reserves in this region. In these wildlife areas, brucellosis has been detected in buffalo, other antelope, zebra, lions, hyenas, and other animals, including monkeys (De Vos and Van Niekerk 1969, Gorsich et al. 2015). Malaria is endemic in the area, but the average annual incidence of the infection has decreased over the past 10 years, due to intensive control activities (Maharaj et al. 2013). The contribution of malaria to the syndrome of AFI has thus reduced.
Participant recruitment
The sample size calculation was done using an infinite population, where 59 samples are required to detect a disease with 95% chance when the actual prevalence of the disease is 5% (Thrusfield 1995). In addition, 64 samples give unilateral 95% confidence intervals (CIs) of proportions of 12% maximum, which was deemed sufficient for the study.
The study involved two groups of participants. The first comprised patients diagnosed with AFI at the clinics, hereafter called febrilers. An AFI case was defined as a patient with documented axillary temperature ≥37.5°C, or a history of fever within the previous 72 h, whom the clinic staff would routinely test for malaria, in terms of the clinic standard operating procedure. Patients who tested negative for malaria were referred to the study nurse to be enrolled in this study. All patients ≥18 years of age who met this case definition were eligible for enrollment from October 2012 to June 2013. Information was captured onto a standard case information form (CIF). This CIF inquired about a variety of symptoms and questions related to risk factors for zoonotic disease, and diagnosis, treatment, and outcome. The selected risk factors were a variety of contacts (such as handling and consumption) with various domestic animals, presence at dip-tanks, and tick bites. Blood samples (one coagulated for serum and one EDTA anticoagulated) for laboratory tests were drawn at the time of presentation (acute sample) and the patients were asked to return 2 to 3 weeks later to provide follow-up convalescent samples. A study nurse facilitated enrolment of volunteers at all the clinic sites.
The second group comprised cattle farmers, herders, and government veterinary staff (animal health technicians and veterinarians), who attended any of five cattle dip-tanks for weekly stock inspections and tick control in the area in 1 week in June 2013 (Fig. 2). This group was called dip-tanksters. They were recruited for interviewing and provided blood samples as described above for the febrilers, but without follow-up samples. A CIF with the risk factors detailed above was also completed, but excluded the clinical symptoms, diagnosis, or treatment and outcome information. All information was captured onto a Microsoft Excel database.

Sampling of dip-tanksters at a dip-tank.
Laboratory methods
Laboratory testing for all samples was performed at the National Institute for Communicable Diseases. Tests for a panel of nine known endemic bacterial and viral zoonoses in South Africa were used in this study (Table 2).
Sensitivity and specificity are included if available.
AFI, acute febrile illness; ELISA, enzyme-linked immunosorbent assay; HAI, hemagglutination inhibition assay; IFA, indirect immunofluorescence assay; PCR, polymerase chain reaction; RVF, Rift Valley fever.
The DNA for the bartonella test was extracted according to Trataris et al. 2012, from packed red blood cells (obtained after spinning down EDTA tube) using the UltraClean® BloodSpin® DNA Isolation Kit (MoBio Laboratories, Czech Republic). The tests for leptospirosis, Q fever, and brucellosis and hemagglutination inhibition assay (HAI) tests were not done in duplicate. The convalescent samples of the AFI patients were tested and, if found positive, then the corresponding acute samples were tested to detect seroconversion. Positive HAI samples were then tested with IgM ELISA.
Statistical analysis
Data were analyzed in multivariable logistic regression models, separately for the clinic and dip-tank data. Test results of each test were used as binary response variables (in different models). Backward selection of explanatory variables was applied using p = 0.05 as a cutoff. The tested explanatory variables were age (continuous), dip-tank attendance, eating wild animals, history of tick bites, herding of livestock, slaughtering of animals, and eating livestock (binary) for both the clinic and dip-tank data. CIs of proportions >0 and <1 were calculated using logistic predictors, whereas the exact method (assuming a binomial distribution) was used for proportions = 0 or 1.
Ethical clearance
Ethical approval was obtained from the University of the Witwatersrand Human Ethics Committee (certificate number M120667) and signed informed consent obtained from study participants. Further permissions were secured from the Mpumalanga Provincial Government for the study to be done at the three clinics.
Results
Participant demographics and symptoms
In the febrilers, of 119 eligible participants, 74 (62%) were enrolled (45 were excluded as they declined consent or the study nurse could not access them). There were 23 (16/23 were adult) AFI patients positive to malaria test during the study period, who were not included in the study. The median age of the 74 febrilers was 34 years (interquartile range [IQR] 25–47 years) and 46/74 (62%) were females, of whom two were pregnant. About half were febrile on examination (38/74, 51%). The median duration of illness was 3 days (IQR 2–7 days). About 10% (6/74) were referred to hospital, and 62% (46/74) received an antibiotic. A quarter did not return for follow-up blood sampling (20/74; 27%). Only four febrilers had no systemic symptoms other than fever, 36/74 (49%) presented with one other symptom, 20/74 (27%) with two, and 4/74 (5%) with three other symptoms. The majority presented with muscle pain (85%), while fewer had respiratory symptoms (14%). A total of 64 dip-tanksters were recruited, of whom, 46 (72%) were male and a median of 55 years old (IQR 42–68 years). The median duration of dip-tank attendance was 15 years (IQR 6–30 years).
Clinical and laboratory findings
In summary, 77% (57/74) of febrilers tested positive for at least one of the zoonotic pathogens included in the panel (Table 3). The most prevalent past infection was the spotted fever group (SFG) (Rickettsia spp.), with 63.4% (45/71, 95% CI 51.6–73.7%) testing positive for anti-Rickettsia IgG, while anti-Rickettsia IgM was positive in 24.5% (13/53, 95% CI 14.8–37.8%) of febrilers, indicating a more recent or current infection. Of the 13 anti-Rickettsia IgM-positive patients, 12 were anti-Rickettsia IgG positive. Antibodies (IgG) to Coxiella burnetii, the causative agent of Q fever, were detected in 38.3% (28/73, 95% CI 28.0–49.9%) of patients. Other bacterial pathogens included bartonellosis with 9.5% PCR positive (7/74, 95% CI 4.6–18.5%), which were identified as Bartonella vinsonii subspecies berkoffii (n = 1) (which has a dog reservoir), Bartonella henselae (n = 2) (domestic cat reservoir), Bartonella quintana (n = 1) [human reservoir (Zeaiter et al. 2002)], and Bartonella thailandensis (n = 1) [rodent reservoir (Saisongkorh et al. 2009)] and two Bartonella positives are unnamed, but rodent borne. Leptospirosis with 6.8% (5/74, 95% CI 2.8–15.2%) group-specific IgM antibodies and brucellosis with 1.4% (1/74, 95% CI 0.2–9.0%) group-specific total antibodies were also found. West Nile and Sindbis fever antibodies were detected in 4.1% (3/73, 95% CI 1.2–12.0%) and 1.4% (1/73, 95% CI 0.2–9.1%) of febrilers, respectively. No chikungunya or Rift Valley fever (RVF) antibodies were found.
SFG rickettsiosis IgM (recent) done on the 45 AFI participants who were positive on SFG rickettsiosis IgG (past) and 19 IgG-negative and one IgG-untested participant.
IgM for Q fever done on acute specimens for which there was no convalescent specimen and in participants who were positive for IgG.
CI, confidence interval.
In the dip-tanksters, the proportion with anti-Rickettsia IgG antibodies was also high at 92.2% (59/64, 95% CI 82.6–96.7%), and 60.9% (39/64, 95% CI 48.6–72.1%) had anti-Coxiella IgG antibodies. No evidence for exposure to Brucella spp. was detected, but 21.9% (14/64, 95% CI 13.4–33.6%) tested positive for Leptospira IgM antibodies. For viral etiologies, 3.1% (2/64, 95% CI 0.8–11.7%) of dip-tanksters tested positive for West Nile virus IgM, 4.7% (3/64, 95% CI 1.5–13.6%) for chikungunya, and 3.1% (2/64, 95% CI 0.8–11.7%) for Sindbis virus antibodies. No RVF antibodies were detected.
The AFI participant arbovirus HAI-positive samples were retested with IgM ELISA and had the following results: the three West Nile virus (WNV) positive samples had two negative results and one untested, and the Sindbis positive was also IgM positive. Among dip-tank participants, for chikungunya, one of the three HAI-positive samples was also IgM positive, one was negative, and the last untested; both WNV HAI-positive samples were IgM negative, and both Sindbis HAI-positive samples were also IgM positive.
The only risk factor that was statistically significantly associated with a disease was attending dip-tanks in febrilers for Q fever IgG (p = 0.007). Thirteen of the 74 (18%) febrilers were found to have previously attended dip-tanks and of those tested, 77% (10/13) were IgG positive compared to 31% (19/62). None of the risk factors for the dip-tanksters were associated with the test results.
Discussion
Our study looked at both acutely febrile participants in clinics and cattle dip-tank participants at high risk for zoonoses. Undifferentiated AFI is among the most common presenting signs in patients seeking medical care in Africa (Perkins et al. 1997, Crump et al. 2003, Van Hemelrijck et al. 2009). Despite this, the syndrome is frequently misdiagnosed and the etiologies still poorly understood. Febrile illness is often misclassified as malaria, especially in adults living in areas with low to moderate malaria transmission (Reyburn 2004, Chandler et al. 2008, Nankabirwa et al. 2009). Misdiagnosis leads to delays in appropriate treatment and higher case-fatality rates (Chandler et al. 2008).
This study showed that 77% of febrilers and 98% of dip-tanksters had at least one positive test. Bartonellosis (PCR 9.5%), spotted fever (IgM 24.1%), and less likely, leptospirosis (IgM 6.8%) and Q fever (IgM 2.3%) could have been the cause of the AFI in the febrilers, as IgM and PCR suggest recent or current infection. This is a valuable finding, relevant to the management of clinic patients, as amoxicillin is the standard treatment for patients with AFI, but it would not be effective for these diseases. Therefore, the AFI treatment algorithms in this and similar settings need to be reconsidered and health staff educated on these infections.
The febrilers also showed a high past exposure (IgG) to SFG Rickettsia spp. (63.4%) and Q fever (37.8%), not previously described in this population. The high proportion of exposure to Rickettsia spp. is understandable, given that 70% of tick pools and 100% of flea pools taken from dogs in the area were positive for Rickettsia spp. (Kolo et al. 2016). Over 70% (50/71) of febrilers had either an SFG Rickettsia spp.- or Q fever-positive result, while 95% of dip-tanksters had either an SFG Rickettsia spp.- or Q fever-positive result. We expect veterinary staff or livestock herders and farmers presenting at the dip-tanks with their livestock to be at a higher risk for zoonotic diseases (especially for those diseases transmitted by vectors/reservoirs and associated with livestock) in this population. However, the only diseases where dip-tanksters had a CI higher than febrilers was spotted fever (IgG). There are differences between proportions of participants positive in the febrilers and dip-tanksters, but this is not strongly statistically supported in this study.
Dip-tanksters are on average 21 years older than febrilers and therefore have had more time for exposure to pathogens. Although the number of zoonotic illnesses per individual was not correlated with years of dip-tank attendance in the dip-tank group, contact with cattle dip-tanks was positively associated with Q fever exposure in AFI patients. The higher proportion of spotted fever IgG in dip-tank participants could be from cattle owners having higher levels of exposure to ticks, related to their dogs and other domestic animals that they interact with daily. There was little evidence of other risk factors contributing to positive serology. The lack of positive associations may be due to a relatively small sample size and test-positives. Also, the environment is homogenous such that even if people say they do not own or work with animals, some contact is inevitable, due to the free-ranging nature of the animals and their close proximity to humans, for example, almost a fifth of the febrilers had some contact with the dip-tanks.
The higher bartonellosis test-positive proportion in febrilers could be as the test was detecting organisms and not antibodies, which would be more closely associated with patients presenting with fever compared to dip-tanksters. Bartonella infection rate in other studies was also found to be high in HIV-infected individuals (Frean et al. 2002, Trataris et al. 2012), and although our participants were not tested for HIV, HIV prevalence may have been higher in the febrilers who had an average age of 34 years compared to the dip-tankster with an average age of 55 years, which correlates with the provincial age and HIV prevalence demographics (Shisana et al. 2014). The Bartonella species found in the febrilers were associated with humans (n = 1) and domestic dogs and cats (n = 3), and rodents (n = 2). Bartonella infections have been found to be common in cats (23.5%) and dogs (9%) in a southern African study (Trataris et al. 2012), and in fleas (36.3%) elsewhere in Africa (Leulmi et al. 2014).
A review of leptospirosis in sub-Saharan Africa, noted very few human studies, with most data being from animals studies (De Vries et al. 2014). In our study, evidence of leptospirosis was higher in the dip-tanksters, although with CIs overlapping, which again makes sense given that transmission to humans is from the urine of infected animals, commonly rodents, pigs, and other domestic animals. Cattle in a neighboring province had leptospirosis prevalence of almost 20% (Hesterberg et al. 2009) and a South African study found leptospirosis in 4.7% (25/530) of dogs tested (Roach et al. 2010). What is more difficult to understand is the dip-tanksters having a threefold higher IgM (which should indicate current or recent infection) than AFI patients. The dip-tank participants may be more consistently exposed to Leptospira spp., but not present with fever at the clinic. The Leptospira ELISA IgM is known to have a low specificity (55%) and diagnostic accuracy, which may influence the reliability of the results (Desakorn et al. 2012).
The brucellosis results are reflective of what has been found in domestic animals in the area. Although brucellosis is present in the region (Hesterberg et al. 2008), unpublished studies suggest that there is no brucellosis in the cattle, goats, and dogs in the study area (Dr. G. Simpson, Pers. Comm., 15th June 2017). This indicates that the control mechanisms of heifer vaccination and movement control may be keeping the disease at bay, even though there are high seroprevalences in buffalo (8.7–47.6%) across the neighboring reserve fences (Gorsich et al. 2015).
The febrilers had 5.5% (4/73) showing at least one arbovirus-positive result compared to the dip-tanksters with 10.9% (7/64). Little is known about the epidemiology of chikungunya virus in the region, although baboons (Papio ursinus) were previously found to be the primary vertebrate reservoir (Mcintosh et al. 1977). The vectors are the tree canopy-associated Aedes furcifer-taylori group, which are less likely to be found in a peridomestic situation, and which rarely feed on humans. The dip-tank participants may be more at risk as they take their cattle and goats into the surrounding bushveld for grazing. The presence of West Nile and Sindbis virus infections, although at low levels, is of interest as patients are not routinely tested for these diseases. There are also veterinary implications associated with their presence.
Vectors can move pathogens between wildlife and domestic animals species (Bengis et al. 2004). This phenomenon is of growing concern with the expanding human populations, habitat destruction, intensification of wildlife, and potentially greater contact between humans and wildlife (Bengis et al. 2004). The diseases investigated in this study can be transmitted to humans through vectors, food, contact, or contamination of the environment, which has implications for vector, hygiene, and environmental control. Malaria control in the area, for example, has had a negative impact on some mosquito populations, which may affect other mosquito-transmitted diseases. Further vector control, disease control in animals, as well as food and other hygiene improvements, would be beneficial in decreasing the burden of these diseases. There is also a need to educate the population about reducing tick and surface water contact.
A limitation of our study was that sample sizes were small. There was only one nurse covering three clinics for AFI patients, which made it difficult to access all the eligible patients. The dip-tank participants were opportunistically selected in a nonrandom manner. This could influence the extrapolation of the results to all the dip-tank attendees.
Conclusions
Bartonella spp., Rickettsia spp., C. burnetii, and Leptospira spp. are present and could be undetected causes of fever and illness in a community bordering wildlife reserves in the north-east of South Africa. Some AFI patients (9.5%) were infected with Bartonella spp. associated with human, rodent, and domestic dog and cat reservoirs. A high proportion of cattle dip-tank attendees and AFI patients had evidence of past infection or background exposure to Rickettsia spp. and C. burnetii, which is of relevance to public and veterinary health. Current AFI treatment algorithms at the clinics prescribe amoxicillin, which would not be effective for these diseases. The low proportion of brucellosis and viral infections is encouraging, but should continue to be monitored. The vector control strategies for livestock and public health should take into account ticks and fleas as they transmit Bartonella spp. and Rickettsia spp. Animal husbandry should be adapted to include means of infection prevention, such as disinfection, after contact with animal excretions to decrease Q fever, leptospirosis, and potentially brucellosis. This is an opportunity for public and animal health organizations to discuss control programs to tackle common afflictions. Wider zoonotic surveillance should be continued, and veterinary and public health services should be aware of these diseases, their diagnoses, and treatments, and educate their patients and owners in prevention methods and care seeking.
Footnotes
Acknowledgments
This study was funded by Swedish Civil Contingencies Agency (MSB) and Swedish International Development Cooperation Agency (SIDA) and by the Global Disease Detection Program. We thank Sr. Aletta Ennica Ntlemo for her hard work collecting the information and samples from patients and following them up, Mpumalanga Veterinary Services, Hans Hoheisen Wildlife Research Station, Hluvukani Animal Clinic and staff, the staff and patients of Gottenburg, Utha, and Welverdiend Clinics, cattle farmers, herders and veterinary staff of Gottenburg, Utha, Welverdiend A and B, and Thlavekisa diptanks who volunteered for the study.
Author Disclosure Statement
No competing financial interests exist.