
Abstract
Background:
Tick paralysis is a frequently overlooked severe disease characterized by bilateral ascending flaccid paralysis caused by a neurotoxin produced by feeding ticks. We aimed to characterize suspected tick paralysis cases documented at the BC Centre for Disease Control (BCCDC) in British Columbia (BC) from 1993 to 2016 and reviewed prevention, diagnosis, and treatment considerations.
Methods:
Demographic, geographic, and clinical data from test requisition forms for ticks submitted to the BCCDC Public Health Laboratory (PHL) from patients across BC between 1993 and 2016 for suspected human and animal tick paralysis were reviewed. Descriptive statistics were generated to characterize tick paralysis cases in BC, including tick species implicated, seasonality of disease, and regional differences.
Results:
From 1993 to 2016, there were 56 cases of suspected tick paralysis with at least one tick specimen submitted for testing at the BCCDC PHL. Humans and animals were involved in 43% and 57% of cases, respectively. The majority of cases involved a Dermacentor andersoni tick (48 cases or 86%) and occurred between the months of April and June (49 cases or 88%). Among known locations of tick acquisition, the Interior region of BC was disproportionately affected, with 25 cases (69%) of tick bites occurring in that area.
Conclusions:
Tick paralysis is a rare condition in BC. The region of highest risk is the Interior, particularly during the spring and summer months. Increasing awareness of tick paralysis among healthcare workers and the general public is paramount to preventing morbidity and mortality from this rare disease.
Introduction
T
Tick paralysis most often appears in the Pacific Northwest during the spring and summer months when tick feeding is most active. The principal tick vector in this area is the Rocky Mountain wood tick, Dermacentor andersoni (Diaz 2015). The primary aim of this study was to characterize demographic, geographic, and clinical parameters for suspected tick paralysis cases documented at the BC Centre for Disease Control (BCCDC) Public Health Laboratory (PHL) in British Columbia (BC) from 1993 to 2016. The secondary aim was to review the pathologic basis of disease, disease prevention, and diagnostic strategies.
Materials and Methods
Live and dead ticks are submitted to the BCCDC PHL from patients across BC, mainly for detecting DNA by PCR if tick species is known to carry Borrelia burgdorferi. Ticks are submitted in small plastic vials containing moist cotton balls. They are identified to the species level by examination of features on the dorsal and ventral sides of the body using a light microscope, as per identification keys by Gregson (1956). For this study, all tick submissions flagged with tick paralysis on the test requisition form from 1993 to 2016 were reviewed. Demographic, geographic, and clinical data were collected from the majority of patients, when available. Descriptive statistics was generated to elucidate tick species and regions of BC implicated in tick paralysis, gender and age distribution, seasonal patterns of disease, and body location predilections.
Results
From 1993 to 2016, there were 56 cases of suspected tick paralysis with at least one tick specimen submitted for testing at the BCCDC PHL. Among these, 24 (43%) involved humans, 31 (55%) involved dogs, and 1 (2%) involved a llama. The majority of cases (48 cases or 86%) involved a Darmacentor andersoni tick, with fewer numbers of Ixodes pacificus (4 cases or 7%), Rhipicephalus sanguineus (3 cases or 5%), and D. albipictus (1 case or 2%) (Fig. 1). The majority of cases (49 cases or 88%) occurred between the months of April and June (Fig. 2). There were 20 cases (human or animal) for which the location of acquisition of the tick was not provided. Among the known locations, the Interior region of BC was disproportionately affected, with 25 cases (69%) of tick bites having been acquired in that area (Fig. 3). Tick bites were also reported from the Kootenays (5 cases or 14%), Vancouver Island (2 cases or 6%), the Lower Mainland (1 case or 3%), the Sunshine Coast (1 case or 3%), and Santa Rosa in California, United States (1 case or 3%). One case listed either the Lower Mainland or the Interior as possible places of tick bite (3%).

Species of tick vectors in tick paralysis cases in British Columbia, 1993–2016.
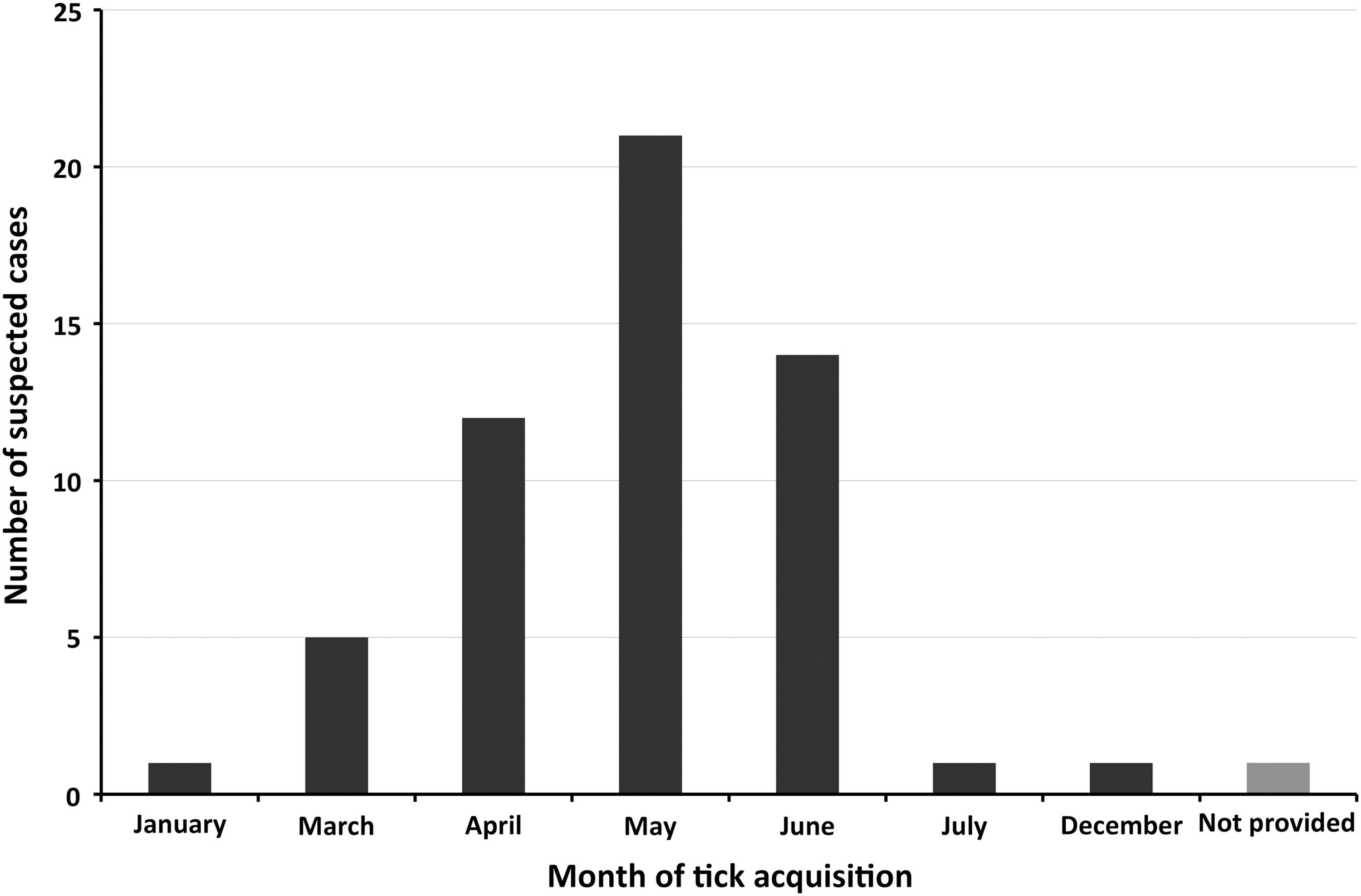
Seasonal distribution of tick paralysis cases in British Columbia, 1993–2016.

Regions of tick acquisition in tick paralysis cases in British Columbia, 1993–2016.
Among the 24 human cases, there was an even distribution of female (13 cases or 54%) and male (11 cases or 46%) subjects. Children under the age of 10 comprised 11 (46%) of the human cases. Twenty-three (96%) human cases had one tick submitted for examination, whereas one (4%) case had two ticks submitted. Only 10 human cases had information about the location on the body where the tick bite occurred: the head and neck were bitten in 8 (80%) cases, while the leg and the arm were each bitten in 1 (10%) case. The symptoms prompting tick submission indicated on laboratory requisitions included ataxia, ataxia with abdominal pain, paresis/paralysis, weakness, diminished reflexes, scalp numbness, bilateral hand paresthesias, and stiff neck or muscles. The most common symptom was paralysis (50% of cases). One case also described fever and a bull's-eye rash at an unspecified location. The tick was identified as Ixodes pacificus and as a result PCR that was done to detect B. burgdorferi, however, was negative. There were no reported deaths in this review.
Discussion
Tick paralysis is a rare condition in BC, with 56 suspected cases over the 24-year period of this review, which translates to an average of two to three potential human and animal cases per year. The distribution of suspected cases is split evenly between humans and animals in BC. In previous reports on humans, most patients were children, particularly girls (Centers for Disease Control and Prevention 2006; Foster et al. 2013). The female to male ratio has been observed as being 4.9:1 in children less than 8 years old (Taraschenko and Powers 2014). This pattern could be due to the tendency of ticks to hide in long hair on females. These patterns were not observed in our study as children under the age of 10 comprised just under half of the human cases, and the number of human cases was split evenly between males and females. As there were only 24 human cases in this study, a review of a longer time period may reveal a tendency toward children and a gender predilection for females. Indeed, our case numbers may not represent the true incidence of tick paralysis due to underreporting. It is probable that not all ticks in suspected cases were submitted to BCCDC PHL for identification and even if submitted, could have lacked mention of tick paralysis on the test requisition, thereby excluding them from this study. BCCDC PHL receives over 1000 ticks yearly, and an average of over 500 ticks is D. andersoni.
Our finding of the high prevalence of D. andersoni ticks implicated in suspected cases of tick paralysis reflects the ubiquity of this tick species throughout BC. Although D. andersoni and Darmacentor variabilis have previously been reported as causing the most cases of tick paralysis in the United States (Diaz 2010), a variety of soft (argasid) and hard (ixodid) ticks have been implicated in both human and animal cases. These ticks include Amblyomma americanum, Amblyomma maculatum, and I. pacificus (Diaz 2015), the last of which was also found in a small proportion (7%) of cases in our study. To the best of our knowledge, this is the first report of Rhipicephalus species ticks causing tick paralysis in BC (5% of cases in this study). The submission of ticks during the months of April through June in our study coincides with peak tick activity during the spring and summer months. Most North American tick paralysis cases have been reported to occur during these months (Centers for Disease Control and Prevention 2006). Most cases of suspected tick paralysis in BC were reported from the Interior region and the Kootenays (86% and 14% of cases with known location, respectively). These regions have a wider distribution of appropriate tick habitat compared to more urban centers in the Lower Mainland and the Sunshine Coast. The high proportion of tick bites occurring in the head and neck area (80% of cases) of humans in our study correspond with previous studies emphasizing preferred tick attachment sites as the head or scalp, and often behind the ears (Diaz 2015).
A limitation of this study is the lack of standardized requisition forms for each patient, which restricted data collection to the information voluntarily submitted by physicians on their requisition forms. Prospective evaluation of tick paralysis cases, although potentially limited by low case numbers, may reveal a better estimate of incidence and details of the clinical syndrome.
The pathological mechanisms of D. andersoni-induced tick paralyses have previously been thoroughly reviewed (Dworkin et al. 1999). Motor neurons of the efferent pathway are affected, but not the afferent. More specifically, acetylcholine release from the synapse is inhibited through targeting of the neuromuscular junction of peripheral nerves. Pathogenic aspects of Dermacentor-induced tick paralysis have been experimentally demonstrated. Some of these features include a decrease of the maximal motor nerve conduction velocities, decrease in nerve and muscle compound action potentials, and impaired impulse propagation of afferent fibers.
Increasing understanding of tick paralysis among healthcare workers is paramount to preventing the adverse sequelae of this rare disease. Although underreporting may be an issue, deaths due to tick paralysis have decreased in recent years, with no reported deaths in the 2000s in the United States or Australia (Diaz 2015). There were no reported deaths in this review. The higher mortality rate of 10–12% during the early 1900s (Dworkin et al. 1999) may be explained by a general lack of awareness of this disease. Tick paralysis should be differentiated from other diseases causing acute ascending flaccid paralysis with preserved sensorium. These include Guillain-Barré syndrome, cervical spinal cord lesions, and poliomyelitis. While there are some clinical features and laboratory findings that can help differentiate these diseases (Diaz 2015), tick paralysis can be definitively and quickly diagnosed by finding and removing an attached tick. Complete neurological recovery will occur in 1.5 days on average in tick paralysis cases after tick removal (Diaz 2010). During active tick feeding season, physicians in BC, especially those serving the Interior region, should rule out tick paralysis in cases of ascending paralysis by eliciting exposure history (outdoor activities) and performing a complete skin examination for attached ticks. Special care should be taken to check tick-preferred areas, such as the head and neck. Increased knowledge of tick paralysis among medical personnel is essential to reducing morbidity and mortality.
Conclusions
For the general public, preventative measures against tick paralysis involve reducing the risk of tick bites. Evading tick-infested areas or bushy vegetation and wearing protective clothing to cover exposed parts of the body are suggested. Thorough inspection of the body for ticks using frequent buddy checks, showering within 2 h after possible exposure, and checking animals/pets regularly and immediately after hikes or other forays into tick habitat are important. The use of permethrin-containing repellents on clothing or DEET (N,N-diethyl-m-toluamide) insect repellent on the skin is also recommended to protect against tick bites. If found, immediate proper removal of ticks should be undertaken (grasping the tick with tweezers as close to the skin as possible, followed by pulling the tick straight out to ensure removal of the head and mouth). Immediate and regular cleansing of the tick bite site is also recommended. Adequate knowledge of tick paralysis among the general public can mitigate the risk of acquiring this disease.
Footnotes
Acknowledgments
We thank all the primary care physicians and veterinarians who submitted ticks used in this analysis.
All authors contributed equally to this work.
Author Disclosure Statement
No competing financial interests exist.