
Abstract
Dengue fever is a global disease with a spectrum of clinical manifestation ranging from mild febrile disease to a severe disease in the form of dengue hemorrhagic fever and dengue shock syndrome. Dengue virus is one viral hemorrhagic fever that exists in the Kingdom of Saudi Arabia in addition to Alkhurma (Alkhurma) Hemorrhagic Fever, Chikungunya virus, Crimean–Congo Hemorrhagic Fever, and Rift Valley Fever. The disease is limited to the Western and South-western regions of Saudi Arabia, where Aedes aegypti exists. The majority of the cases in Saudi Arabia had mild disease and is related to serotypes 1–3 but not 4. The prospect for Dengue virus control relies on vector control, health education, and possibly vaccine use. Despite extensive collaborative efforts between multiple governmental sectors, including Ministry of Health, Ministry of Municipalities and Rural Affairs, and Ministry of Water, dengue remains a major public health concern in the regions affected.
Introduction
D
Dengue infection occurs in an endemic form in 128 countries worldwide (Khetarpal and Khanna 2016). DF is one of several viral hemorrhagic fevers that exist in the Kingdom of Saudi Arabia (Alhaeli et al. 2016) in addition to Alkhurma (Alkhurma) Hemorrhagic Fever (AHF) (Zaki 1997, Al-Tawfiq and Memish 2017), Chikungunya Hemorrhagic Fever (Hussain et al. 2013), Crimean–Congo Hemorrhagic Fever (CCHF) (El-Azazy and Scrimgeour 1997, Hassanein et al. 1997, Leblebicioglu et al. 2015), and Rift Valley Fever (Balkhy and Memish 2003, Al-Afaleq and Hussein 2011). Of the four serotypes of Dengue virus, serotypes 1–3 but not 4 were reported in Saudi Arabia (Ashshi 2017). The first description of DF in Saudi Arabia dates back to 1994 when Dengue virus serotype 2 (DEN-2) was isolated from a fatal and a nonfatal case in Jeddah, Saudi Arabia (Fakeeh and Zaki 2001).
Search Strategy
The search included MEDLINE and Scopus databases for articles published in English as follows: 1. “Dengue” OR “Dengue Virus” OR “Dengue Hemorrhagic Fever” OR “Dengue Fever” 2. “Saudi Arabia” OR “Kingdom of Saudi Arabia”; 3. #1 AND #2.
In addition, we searched the Saudi Epidemiology Bulletin (available from the Saudi Ministry of Health 2007–2016,
The Virus
DF, DHF, and DSS are caused by the dengue viruses (DENV). Dengue virus is a member of the genus Flavivirus, a member of the family Flaviviridae. The genus Flavivirus is classified into two broad categories based on the vector of transmission: tick-borne viruses and mosquito-borne viruses (Fig. 1). The Dengue virus is a mosquito-borne virus. Four antigenically related but distinct dengue virus serotypes exist and are: dengue virus types 1–4 (DENV-1, DENV-2, DENV-3, and DENV-4) (Khetarpal and Khanna 2016).
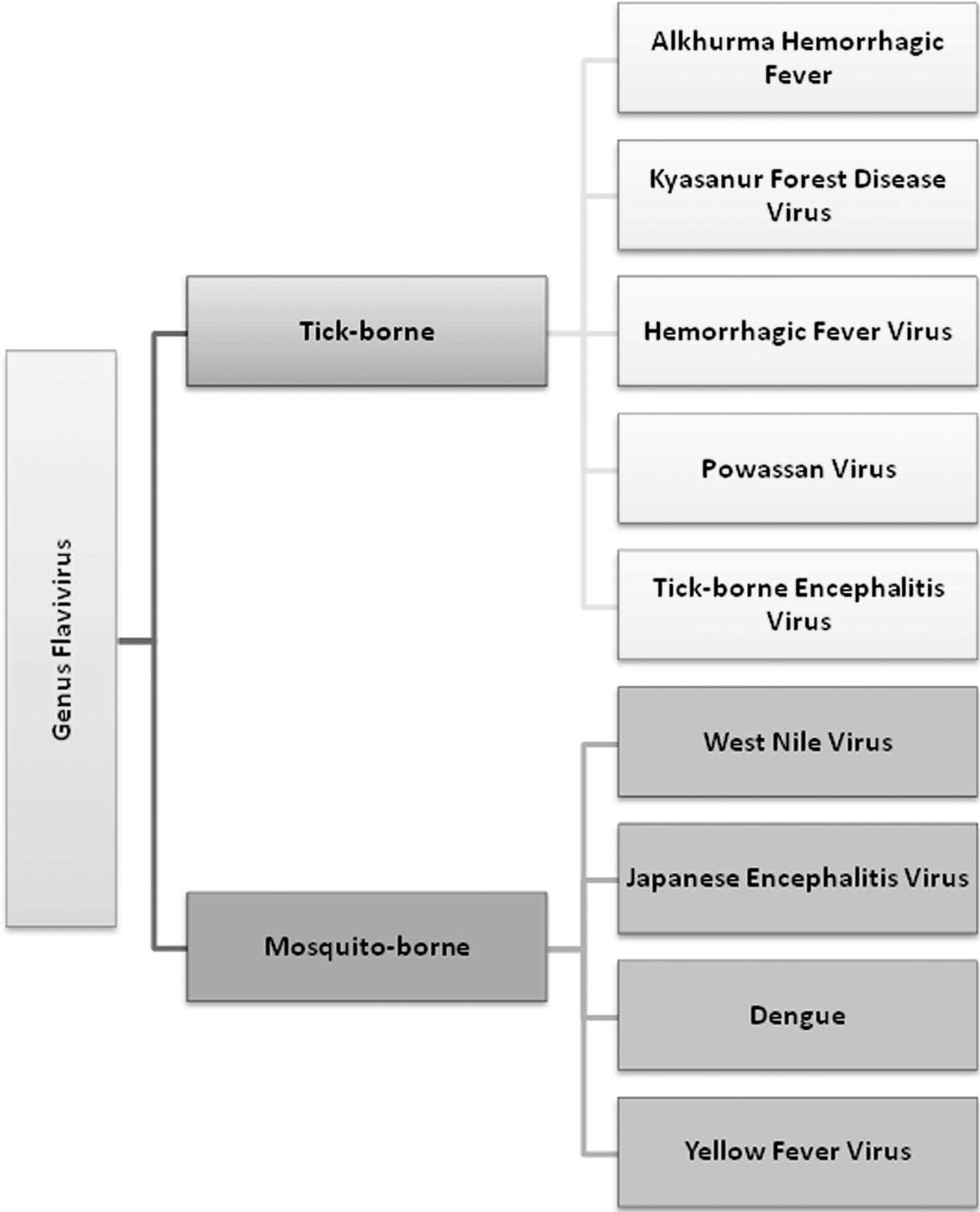
Genus flavivirus and the Dengue virus.
Virus Transmission
The Dengue viruses are transmitted to humans by the females of the mosquito Aedes. The most important vector is Aedes aegypti and other species such as Aedes albopictus, Aedes polynesiensis, and Aedes niveus are secondary vectors (Malavige et al. 2004). The virus is limited to the Western and South-western regions of Saudi Arabia (Fakeeh and Zaki 2001, Ayyub et al. 2006, Khan et al. 2008, Al-Azraqi et al. 2013, Alhaeli et al. 2016, El-Kafrawy et al. 2016). Four different Aedes species were identified in the Western part of Saudi Arabia (Abdullah and Merdan 1995, Jupp et al. 2002, Alahmed et al. 2009, Kheir et al. 2010, Al Ahmad et al. 2011, Aziz et al. 2012, Alikhan et al. 2014) and only A. caspius was identified in the Eastern region of Saudi Arabia (Wills et al. 1985) (Table 1). In a case–control study, the following factors were associated with the risk of Dengue virus infection: presence of stagnant water (OR = 4.9), indoor larvae (OR = 2.2), construction sites (OR = 2.2), and older age (OR = 1.2) (Kholedi et al. 2012). It is known that rainfall in Jeddah is low. The occurrence of A. aegypti with DF in Jeddah is in paradox with the low level of rain; however, water containers play a role as breeding sites for A. aegypti (Ghaznawi et al. 1997, El-Gilany et al. 2010). In addition, the occurrence of huge constructions between 2008 and 2012 in Makkah, Saudi Arabia may have resulted in increased number of cases due to the formation of stagnant water (alwafi et al. 2013). Moreover, Jeddah is the Hajj entry point and is the largest commercial port and airport welcoming many Pilgrims coming from Dengue High Disease Burden countries. Thus, in this context, the role of International Travel as the source of Dengue is a possibility. A recent study highlighted the role of visitors from dengue endemic countries in the importation of the virus into Saudi Arabia (Al-Saeed et al. 2017). The study showed that all dengue viruses in 2010–2015 were from the circulating Indian subcontinent lineage of the Cosmopolitan genotype (Al-Saeed et al. 2017).
Incidence
In Saudi Arabia, DF electronic registry was initiated by the MoH in 2008 after dengue was added to the notifiable diseases list. The incidence of DENV infection among tested patients varies based on the location, year of the study, and the method of testing (Table 2) (Fakeeh and Zaki 2001, 2003, Ayyub et al. 2006, Khan et al. 2008, Shahin et al. 2009, El-Gilany et al. 2010, Memish et al. 2011, Al-Azraqi et al. 2013, alwafi et al. 2013, Gamil et al. 2014, Ashshi 2017, Ashshi et al. 2017, Organji et al. 2017). The number of DENV infection was 6512 cases in 2013; 2081 cases in 2014; and 4312 cases in 2015. The number of cases varies between 425 and 4312 per year (Alshamrani et al. 2015; Organji et al. 2017). The annual number of cases of Dengue virus in and n Saudi Arabia shown in Figure 2 and the highest number of cases was in 2013, 2015, and 2016. However, the overall prevalence of DENV is 40–48.7% among clinically suspected patients (Ayyub et al. 2006, Khan et al. 2008) and 31.7% among random sample of patients attending the outpatients' clinics (Al-Azraqi et al. 2013). In a study from 2008 to 2012, the incidence rate doubled to 110 per 100,000 population in 2009, indicating the occurrence of an outbreak (alwafi et al. 2013). The majority of affected patients are adults and infected children constituted 24% (Shahin et al. 2009) in one study and 6% in another study (Ayyub et al. 2006). In a recent study, the age-standardized incidence rates of dengue was 10–99 per 100,000 person-years in 2013 (Stanaway et al. 2016).

Seasonality
In a study of 159 cases in Makkah, 77% of the cases were during the spring and early summer (Shahin et al. 2009). Another study showed increased cases in the summer months and during the months of December and January (Kholedi et al. 2012). In a study of 4187 cases, the peak cases occurred in April–May (alwafi et al. 2013) and a similar finding was in a report of 264 cases from Jazan (Gamil et al. 2014) and a study of cases in 2013–2014 (Aziz et al. 2014a). Thus, the majority of cases occurred in April–May.
Clinical Presentations
DF is characterized by constitutional symptoms of fever, severe headache, backache, joint pains, nausea and vomiting, eye pain, and rash. The disease affects all age groups but tends to cause milder disease in young children. Dengue virus may cause one of four syndromes/diseases: undifferentiated fever, classic DF, DHF, or DSS. The first 207 patients had mild DF and only one patient had DSS and one had DHF (Fakeeh and Zaki 2001). The affected patients in Saudi Arabia were more likely to be males and of young age group (summarized in Table 3). The signs of symptoms of Saudi patients with dengue infections are summarized in Table 4 (Ayyub et al. 2006, Khan et al. 2008, Shahin et al. 2009, Ahmed 2010, El-Gilany et al. 2010, Badreddine et al. 2017). The majority of patients (60–93%) who presented with DF, 5–39.4% had DHF, and about 1% had DSS. The reported mortality was also low. Dengue infection accounts for a total of 0.15–0.29 mortality per million person-years in Saudi Arabia in 2013 (Stanaway et al. 2016). Men are more affected than women in the various studies included. This is mainly related to the fact that men work outdoors and that women in Saudi wear clothing covering head to toes (Alwafi et al. 2013).
DENV, Dengue viruses.
DHF, dengue hemorrhagic fever; DSS, dengue shock syndrome.
Geographic Distribution
Dengue virus was mainly reported from the Western and South-western regions of Saudi Arabia (Fakeeh and Zaki 2001, Ayyub et al. 2006, Khan et al. 2008, Al-Azraqi et al. 2013, Alhaeli et al. 2016, El-Kafrawy et al. 2016). This geographic restriction is directly related to the presence of A. aegypti in the affected regions (Jupp et al. 2002, Alahmed et al. 2009, Kheir et al. 2010, Al Ahmad et al. 2011, Aziz et al. 2012, Alikhan et al. 2014) and not in other parts of the Kingdom of Saudi Arabia (Wills et al. 1985, Abdullah and Merdan 1995). Mathematical modeling showed that central Jeddah districts were the hotspots and the pattern changes greatly with time (Khormi et al. 2011). Using modeling techniques, a total of 111 districts in Jeddah were investigated for the risk of DF (Khormi and Kumar 2012). Of those districts, 15% were high risk, 22% were medium risk, 16% were low risk, and 46% were very low risk (Khormi and Kumar 2012). In analysis of 2288 cases of DF from Jeddah, the disease was found to be concentrated in the south and central-north regions of Jeddah, Saudi Arabia (Alzahrani et al. 2013).
Virus Serotypes
Dengue virus serotype is associated with the risk of DHF with highest risks with DENV-2, DENV-3, DENV-4, and DENV-1, as well as the pre-existence of antidengue antibodies. In the initial study of 985 suspected cases, DEN-2 accounted for 138 (66.7%) of 207 isolates, DEN-1 for 56 (27%), and DEN-3 for 13 (6.3%) (Fakeeh and Zaki 2001). The contribution of each serotype to Dengue in Saudi Arabia is shown in Table 3. However, DENV-4 was not reported in any of the studies based on serology and molecular testing (Fakeeh and Zaki 2001, 2003, Ayyub et al. 2006, Khan et al. 2008, Organji et al. 2017). Phylogenetic analysis of 19 isolates showed that DENV-1 and DENV-2 caused the 1994 outbreaks and it was an America–Africa genotype (lineage India-2) (Zaki et al. 2008). DENV-3 was isolated in 1997 and the outbreak in 2005–2006 was caused by a strain from genotype Asia (lineage Asia-2) (Zaki et al. 2008). Sequencing of the Dengue virus DENV-1-Jeddah-1-2011 strain showed high similarity with the Asian genotype (D1/H/IMTSSA/98/606 isolate) reported from Djibouti in 1998 (Azhar et al. 2015).
Seroprevalence Among Asymptomatic Individuals
The seroprevalence of Dengue virus antibodies among asymptomatic individuals was found to be 47.8% (927/1939) and among blood donors was 37% (68/184) (Jamjoom et al. 2016). The seroprevalence of antidengue IgG was 31.7% among asymptomatic persons attending outpatient clinics (Al-Azraqi et al. 2013). In one study, male gender, older age, and communal and multistory housing were significant factors for positive ELISA tests (Jamjoom et al. 2016). In a seroprevalence study of 1024 soldiers, only 0.1% tested positive for DENV by ELISA (Memish et al. 2011). Thus, there is variable seroprevalence of dengue among the different populations studied and is higher among patients attending outpatient clinics (31.7%) than the general population (0.1%). The general population may also represent the different regions of the country, which are not affected by DF.
Prospect for Control
Strategies to control Dengue virus requires the control of the vector, A. aegypti, through elimination of breeding sites and the elimination of the vector itself. It is important to intensify the use of insecticides to control mosquito due to the quick and efficient knockdown activity (Aziz, et al. 2014b). In one study in Jazan, Saudi Arabia, A. aegypti mosquitoes were susceptible to Cyfluthrin and had variable resistances to other insecticides, such as lambda-cyhalothrin, Deltamethrin, Permethrin, Fenitrothion, Bendiocarb, and dichlorodiphenyltrichloroethane (DDT) (Alsheikh et al. 2016). Health education and awareness of the disease and its vector play a major role in the control of Dengue in Saudi Arabia (Aziz et al. 2014b). In one study from Saudi Arabia, high-school students' knowledge score was associated with family history of DF, having literate mothers, and age ≥17 years (Ibrahim et al. 2009). Gambusia holbrooki fish was effective in domestic water containers to control A. aegypti (Gamal 2012). In addition, the World Health Organization provides 36 boxes for the control of DF and includes Aedes control methods, Global Strategy for prevention and control of DF/DHF, and lessons learned from sustained efforts in countries combating dengue virus (Parks and Lloyd 2004). One dengue virus vaccine was licensed in Latin America and Southeast Asia. Two large phase III randomized controlled trials of this vaccine showed about 60% efficacy against virologically confirmed dengue in the first 13 months postvaccine (Capeding et al. 2014, Villar et al. 2015). In a meta-analysis of nine studies, the vaccine efficacy was 54% with reduced efficacy of 34% for DENV2 (Malisheni et al. 2017). However, the vaccine was associated with higher relative risk of dengue infection during the third year postvaccination (Hadinegoro et al. 2015). The World Health Organization does not recommend the use of the vaccine for widespread vaccination nor for the use in areas with less than 50% seroprevalence (Anon 2016, World Health Organization 2017).
Conclusion
DF in Saudi Arabia is limited to the Western and South-western regions of the country and is linked to A. aegypti. The majority of the patients had mild disease and was caused by serotypes 1–3. Despite extensive collaborative efforts between multiple governmental sectors, including Ministry of Health, Ministry of Municipalities and Rural Affairs, and Ministry of Water, dengue remains a major public health concern in the regions affected. The prospect for Dengue virus control relies on vector control, health education, and possibly vaccine use.
Footnotes
Author Disclosure Statement
No competing financial interests exist.