
Abstract
Background:
A Japanese encephalitis (JE) epidemic occurred in 2013 in China. The aim of this study was to determine the spatial–temporal pattern of JE cases in adults occurring in 2013, as well as identify potential hotspots of incidences in the afflicted regions in China.
Methods/Principal Findings:
To generate a spatial–temporal pattern of JE cases in China, epidemiological and demographic data between 2011 and 2013 were collected. Our results indicate that the total number of JE cases in 2013 was significantly higher compared with those in 2011 and 2012. While the incidence of JE in individuals aged less than 15 years decreased in 2013, the incidence rate increased substantially in those aged 15 years and older. The population aged over 40 years was associated with the greatest increase of JE. Demographic analysis revealed a consistent increase in the proportion of JE cases aged 15 years and older in 2013 (42%) compared with that in 2012 (15%). In addition, JE cases from areas located between 35°N, 114°E and 40°N, 120°E in northern China were found to account for 27.17% of total JE cases nationwide in 2013, compared with 2.21% and 3.13% in 2011 and 2012, respectively. In these northern regions, the group aged 15 years and older represents the predominant population with JE, accounting for 73% of total cases. Further cluster analysis identified a large number of hotspots of JE in adults (>15 years of age) in northern China.
Conclusions/Significance:
Unlike the JE epidemics primarily in children below 15 years old in southern China, a significant outbreak of JE occurred in northern China in 2013, with the older age groups being the primary population affected. The increasing incidence of JE in adults has become an important public health issue and poses a new challenge to the successful prevention and control of JE in China, as well as other countries in East Asia.
Introduction
J
In the past, many regions of China were highly endemic for JE. Fortunately, the incidence of JE has decreased significantly, mostly owing to the JE vaccination campaign initiated in the 1980s (Gao et al. 2010, 2014, Zheng et al. 2012). In 2008, the JE vaccine was included in the national Expanded Program on Immunization (EPI), allowing children less than 15 years of age to receive free vaccination. As a result, JE incidence further decreased and reached the lowest level in history since 1951 (Gao et al. 2014, Li et al. 2016). In the past decade, JE was mostly distributed in provinces in southern China (latitude 15–30°N, longitude 95–140°E), including Sichuan, Chongqing, Yunnan, and Guizhou, where children aged less than 15 years were the predominant JE-infected individuals in the population (Li et al. 2016). However, more recently an increase in JE cases among adults has been reported in parts of northern China (latitude 30–50°N, longitude 70–140°E). In these regions, the proportion of adult cases, especially those aged 40 years and older, has increased significantly, exceeding the proportion of cases in children and has become the primary population for local cases of JE (Wang et al. 2007, Li et al. 2016).
In 2013, a notable increase in JE cases was reported at the country level, most of which occurred within the adult population rather than children as demonstrated in previous years. The number of JE cases in the population aged 40 years and older increased nearly fourfold (394.16%) compared with that in 2012, while the number of cases in children decreased by 17% in the country (Li et al. 2016). Furthermore, the majority of these adult cases occurred in the northern region of China. In fact, 407 cases were reported in Shandong Province alone, 49.1% of which were aged 40 years and older while only 26.78% were less than 15 years of age (Tao et al. 2014). Besides, all the JEVs isolated in Shandong belonged to genotype 1. In some of these northern provinces, the ratio of JE cases aged 40 years and older was even higher than the overall national average in 2013 (Li et al. 2016).
Evidently, the increasing incidence of JE among adults has become a significant public health issue that needs to be addressed. In the present study, we used a population-based approach to analyze data obtained from the 2013 outbreak of JE in adult populations in northern China and to provide further spatial and temporal insights to this change in the epidemiological characteristics of JE.
Materials and Methods
Data collection and management
The epidemiological and demographic data of JE used in the study were collected from the China Information System for Disease Control and Prevention (Wang et al. 2013). This study did not use any patient medical records or direct personal identifiers, and all data were anonymized for collection and analyses. The types of data collected included the number of reported JE cases and the incidence and mortality of JE, as well as demographic information such as age distribution, gender, and occupation from 31 provinces (cities or autonomous regions) of China in 2013.
Analysis of epidemiological characteristics
The epidemic trend and seasonal characteristics, as well as age distribution and occupation distribution of JE in 2013, were analyzed and presented in the form of line charts and histograms. We used a series of thematic maps, based on JE incidence data from all provinces in China in 2013, to analyze the spatial and temporal patterns of JE cases.
Spatial cluster analysis
Local Indicators of Spatial Association (LISA) were used to evaluate the spatial clusters of reported cases of JE at the county level in Shandong and Hebei Provinces, which represented the two epidemic areas of JE adult cases in 2013 in northern China. By calculating the Local Moran's I coefficient, which typically ranges from −1 to 1, the spatial correlations between the data on a local area unit basis, and the average of neighboring values in the surrounding units, are revealed on LISA cluster maps (Anselin 1995, Impoinvil et al. 2011).
The Z-score is used to assess the significance of observed spatial correlations, as indicated by Local Moran's I. When the Z-score is greater than 1.96 or lower than −1.96, the spatial correlation of the local area units is denoted as being significant (α = 0.05). A high positive Z-score indicates that the surrounding features have either similarly high values (High-High) or similarly low values (Low-Low), while a low negative Z-score indicates a significant (p < 0.05) spatial outlier (High-Low or Low-High) (ESRI 2017). The spatial statistical analysis module of ArcGIS software (version 10.4; ESRI, Redlands, CA) was used to perform LISA analysis and identify the spatial clusters of adult cases of JE in JE-epidemic areas.
Results
Epidemiological features of JE in China, 2013
Incidence and mortality
In total, 2178 cases of JE were reported in 2013, while the average number of JE cases in 2011 and 2012 was 1700 (specifically, 1625 in 2011 and 1788 in 2012). Compared with the previous 2 years, the number of JE cases increased by 28% in 2013 and decreased dramatically in the following years, with 922 cases of JE reported in 2014 and 733 cases in 2015. The sum of JE cases from the latter 2 years was significantly lower (75%) than that reported in 2013 alone, indicating that a JE epidemic occurred in 2013 (Fig. 1). The annual incidence and mortality of JE in 2013 were 0.1611/100,000 and 0.0049/100,000, respectively.
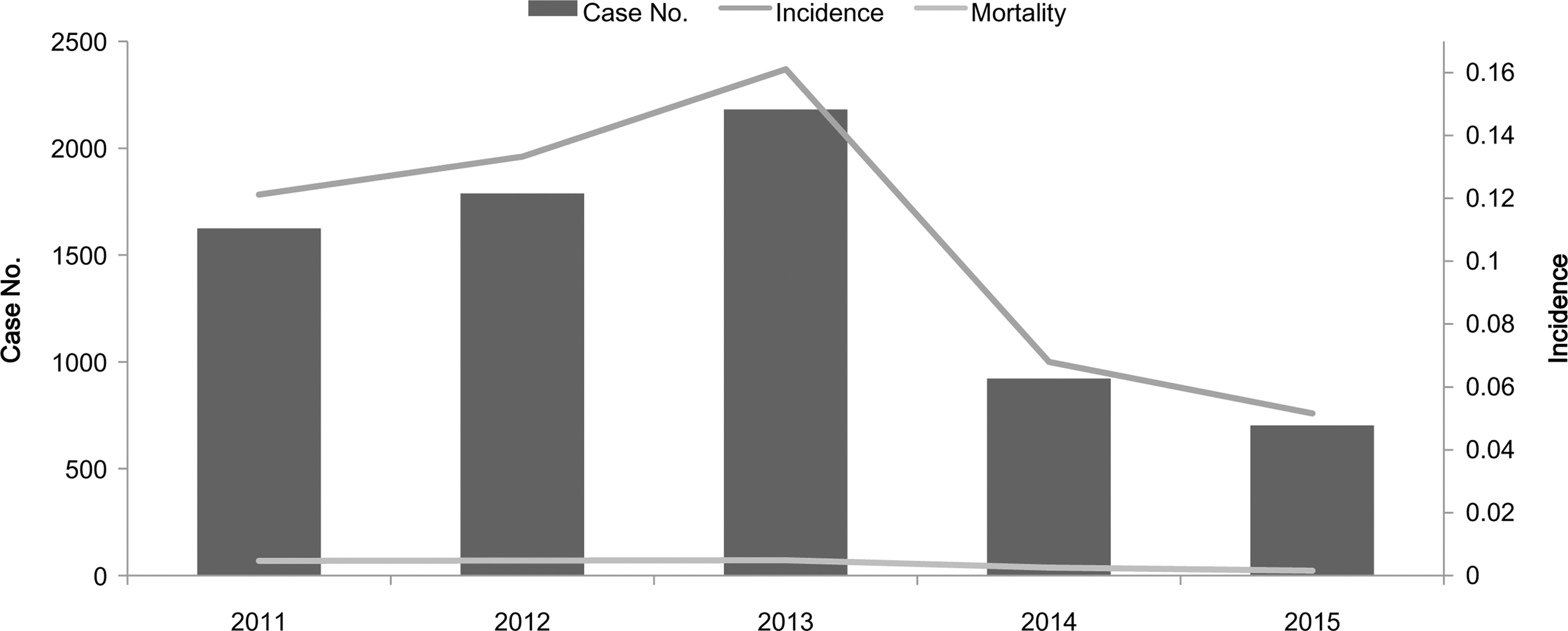
JE in China, 2013. A JE epidemic peak was observed in China in 2013, with the case numbers and incidence of JE being higher than in 2011–2012 and also 2014–2015. JE, Japanese encephalitis.
Gender and occupation
The male to female ratio of JE cases in 2013 was 1.22:1. Analysis of occupation distribution from the reported JE cases indicates that the incidence rate was highest in farmers, accounting for 32.32% of total JE cases, followed by scattered children and students, accounting for 28.93% and 22.54%, respectively. In contrast, the latter two populations ranked top two in 2012, accounting for 43.85% and 28.53% of total JE cases, respectively, while farmers accounted for only 9.81%. Evidently, the proportion of farmers with JE increased significantly in 2013 compared with the previous year.
Age group
The incidence of JE in children (<15 years old) in 2013 remained high. Specifically, the incidence rates were 0.68/100,000 and 0.71/100,000 in the 0- to 5- and 5- to 10-year-old groups, respectively. Both of these were much higher than the national average. Compared with 2011 and 2012, the incidence of JE in children in 2013 had decreased significantly, while that in groups of 15 years and older had increased, especially in adults aged 40 years and older (Fig. 2A). The proportion/ratio of JE cases in the population aged 15 years and older had increased from 11% in 2011 and 15% in 2012 to 42% in 2013. The total number of adult cases also increased notably.
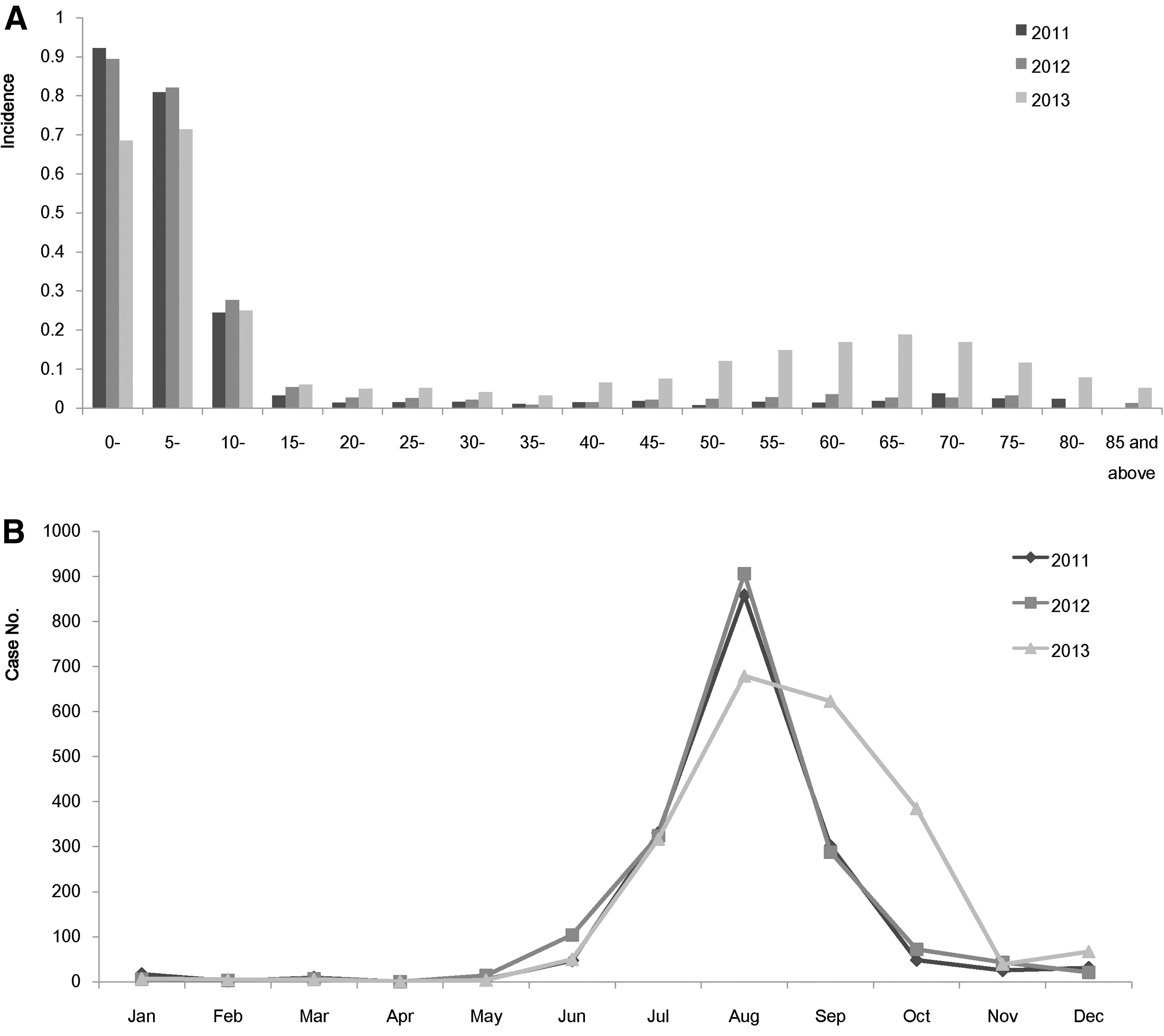
The age and seasonal distribution of JE in China, 2013.
Seasonal distribution
The incidence and distribution of JE exhibited a seasonal pattern. Although reported throughout the year, cases of JE were recorded mainly between the months of June and October, with a peak incidence rate in August (Fig. 2B). In contrast with 2011 and 2012, when JE incidence dropped after August, the number of JE cases reported in September and October of 2013 remained at a high level and was significantly higher than those observed in the same period from the previous 2 years.
Geographical distribution
The JE epidemic areas were mainly distributed in southwestern China, including Sichuan, Chongqing, Guizhou, and Yunnan provinces, as well as in northern China, including Shandong, Hebei, and Shanxi provinces (Fig. 3). The JE incidence in these areas (0.3/100,000) was higher than the national average in 2013.

The geographical distribution of JE in China, 2013. Eight provinces located in the southwest and north of China were denoted as JE high-prevalence areas with the incidence higher than the national average level (0.16/100,000) in 2013. The areas next to the west of Sichuan (west of 100°E) and north of Hebei (north of 35°N) have rare cases of JE. Symbols: HLJ, Heilongjiang; JL, Jilin; LN, Liaoning; NMG, Inner Mongolia; BJ, Beijing; TJ, Tianjin; HB, Hebei: HN, Henan; SD, Shandong; SX, Shanxi; SaX, Shaanxi; NX, Ningxia; GS, Gansu; QH, Qinghai; XJ, Xinjiang; XZ, Tibet; SC, Sichuan; CQ, Chongqing; YN, Yunnan; GZ, Guizhou; GX, Guangxi; GD, Guangdong; GX, Guangxi; HuN, Hunan; HuB, Hubei; JX, Jiangxi; JS, Jiangsu; ZJ, Zhejiang; AH, Anhui; FJ, Fujian; SH, Shanghai; HaN, Hainan; TW, Taiwan.
JE outbreaks in northern China in 2013
By comparing the number of cases of JE from individual provinces between 2012 and 2013, we found that the provinces with an increasing number of JE cases were distributed mainly in the northern region of China, particularly in Hebei, Shandong, Shanxi, and Shaanxi provinces (Fig. 4). Shandong had the greatest increase of JE cases (356 in total), followed by Hebei, which had a total of 229 cases. However, the number of JE cases in most provinces in southern China decreased by various degrees, with 136 cases reported in Yunnan, 63 cases in Guizhou, and 49 cases in Chongqing. In summary, compared with 2012, the increased number of JE cases in 2013 occurred mostly in northern China (Fig. 4).
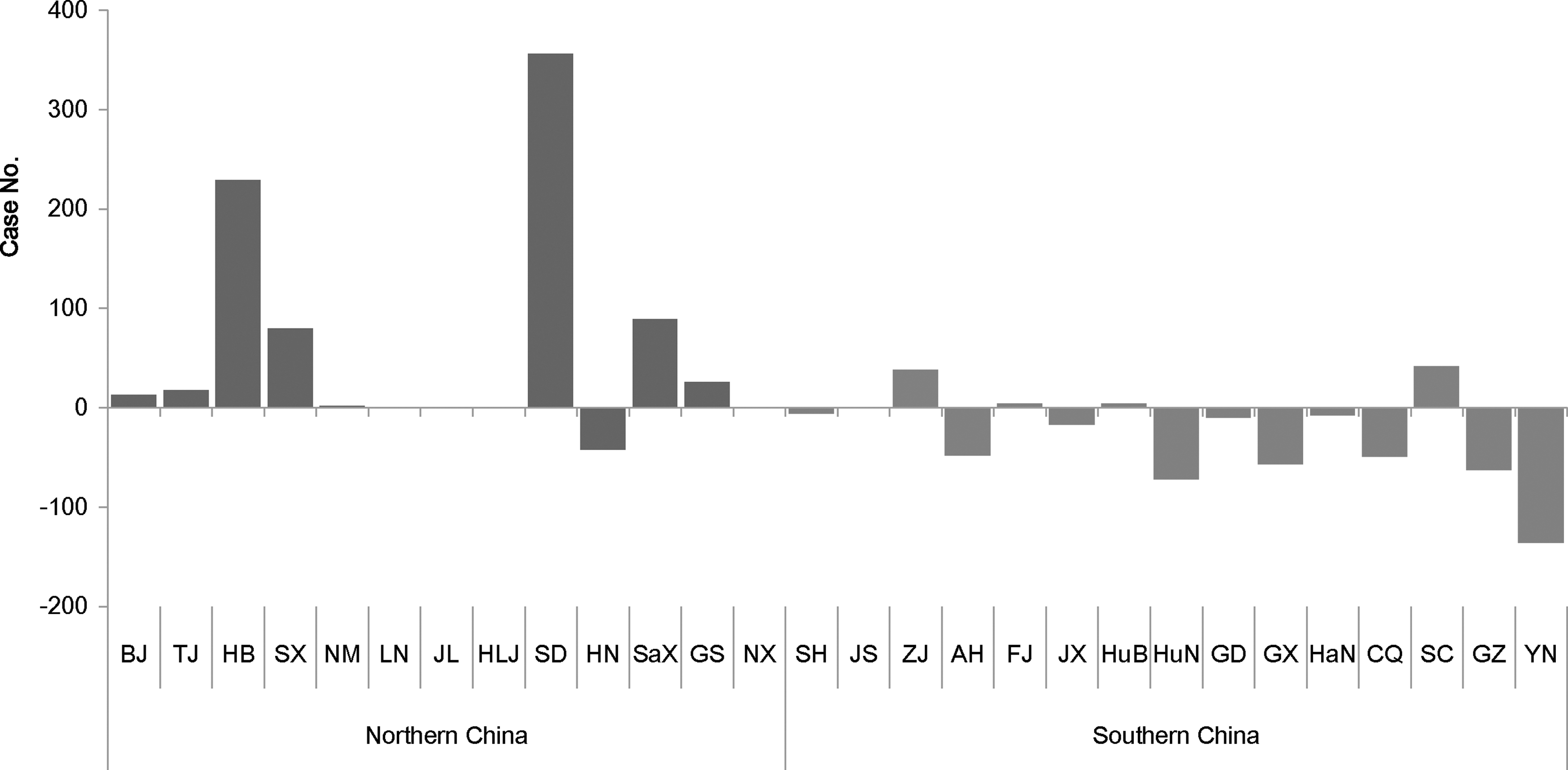
Comparison of case numbers of JE between 2012 and 2013. Compared with 2012, more JE cases in 2013 were mainly distributed in northern China (latitude 30–55°N, longitude 70–140°E; black), including Shandong and Hebei. Most provinces in southern China (latitude 15–30°N, longitude 95–140°E; gray) showed a decrease in JE cases at various degrees.
To gain more spatial insights into the JE epidemic, we analyzed and compared the geographical distribution of cases occurring from September to November in 2012 and 2013. We selected this time period because a dramatic increase in JE incidence was observed in September and October of 2013 compared with previous years (Fig. 2B). As shown in Fig. 5, a larger number of JE cases reported in September and October 2013 were concentrated in the Shandong and Hebei provinces of northern China, and the total case number was significantly higher than that from the same period of the previous year. Specifically, a total of 592 JE cases were reported in Shandong and Hebei in September and October, accounting for 58.73% (592/1008) of total cases nationwide from that time period, while it was only 11.67% (42/360) and 13.16% (20/152) in 2012 and 2014, respectively. In addition, the case number increased by 550 from September to October in 2013. Thus, these data indicated that a JE outbreak had occurred in the Shandong and Hebei provinces of northern China in September and October 2013.
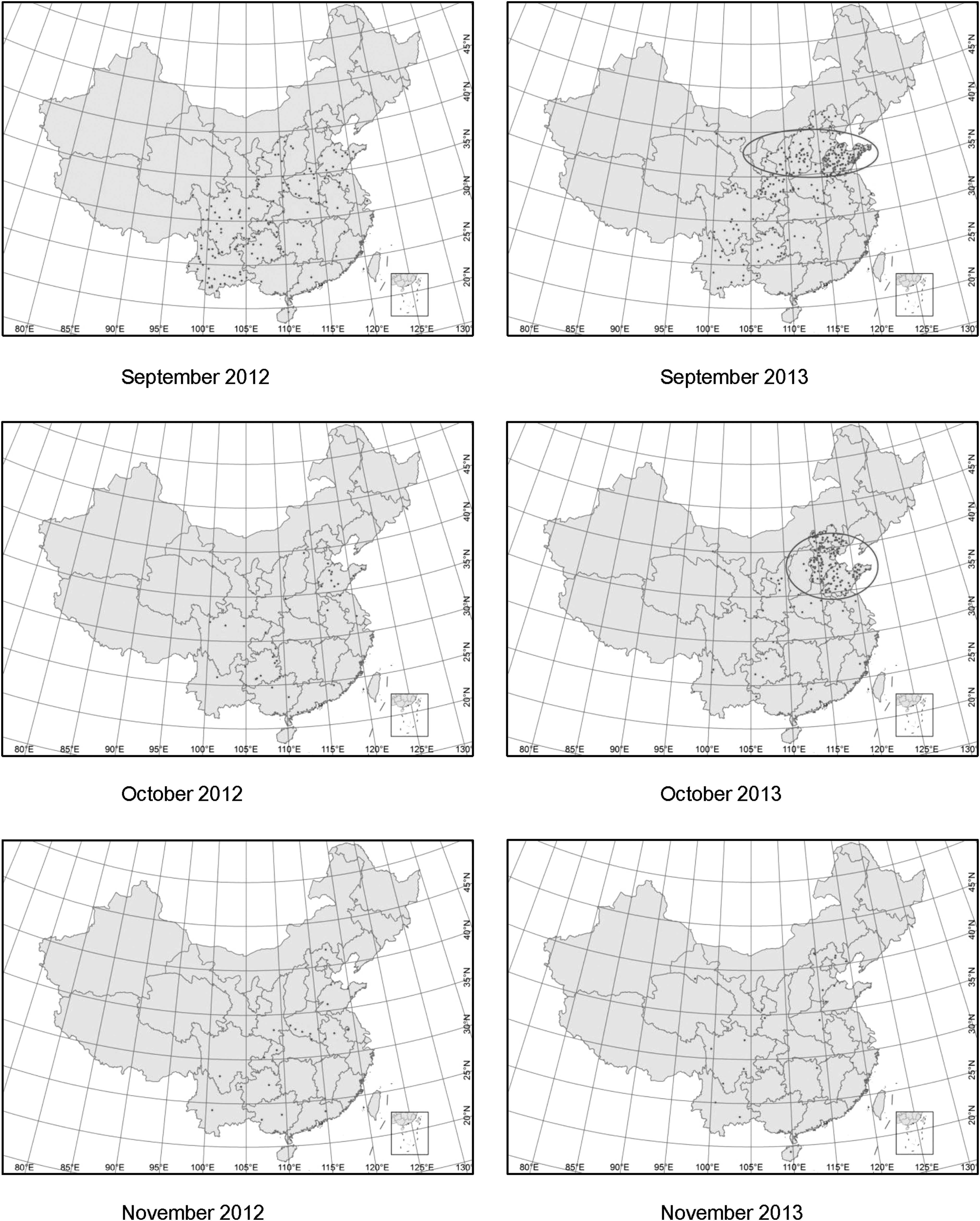
Geographical distribution of JE in September and October of 2012 and 2013. A large amount of JE cases concentrated in Shandong and Hebei of northern China in September and October 2013 (latitude 35–40°N, longitude 114–120°E; black circle).
Cluster analysis of the 2013 JE outbreak in northern China
Spatial clusters
JE cases occurred mostly in Shandong and Hebei (35–40°N, 114–120°E) during the 2013 outbreak in northern China (Figs. 5 and 6A). According to the LISA cluster map, significant spatial clusters of high JE incidence existed in September (Fig. 6B), which involved areas in the northwest regions of Shandong (36–38°N, 115–117°E). Areas of JE clustering gradually moved toward the northwest region in October and were located between latitude 38–40°N and longitude 114–116°E (Fig. 6C). The number of hotspots (High-High) decreased in November (Fig. 6D).
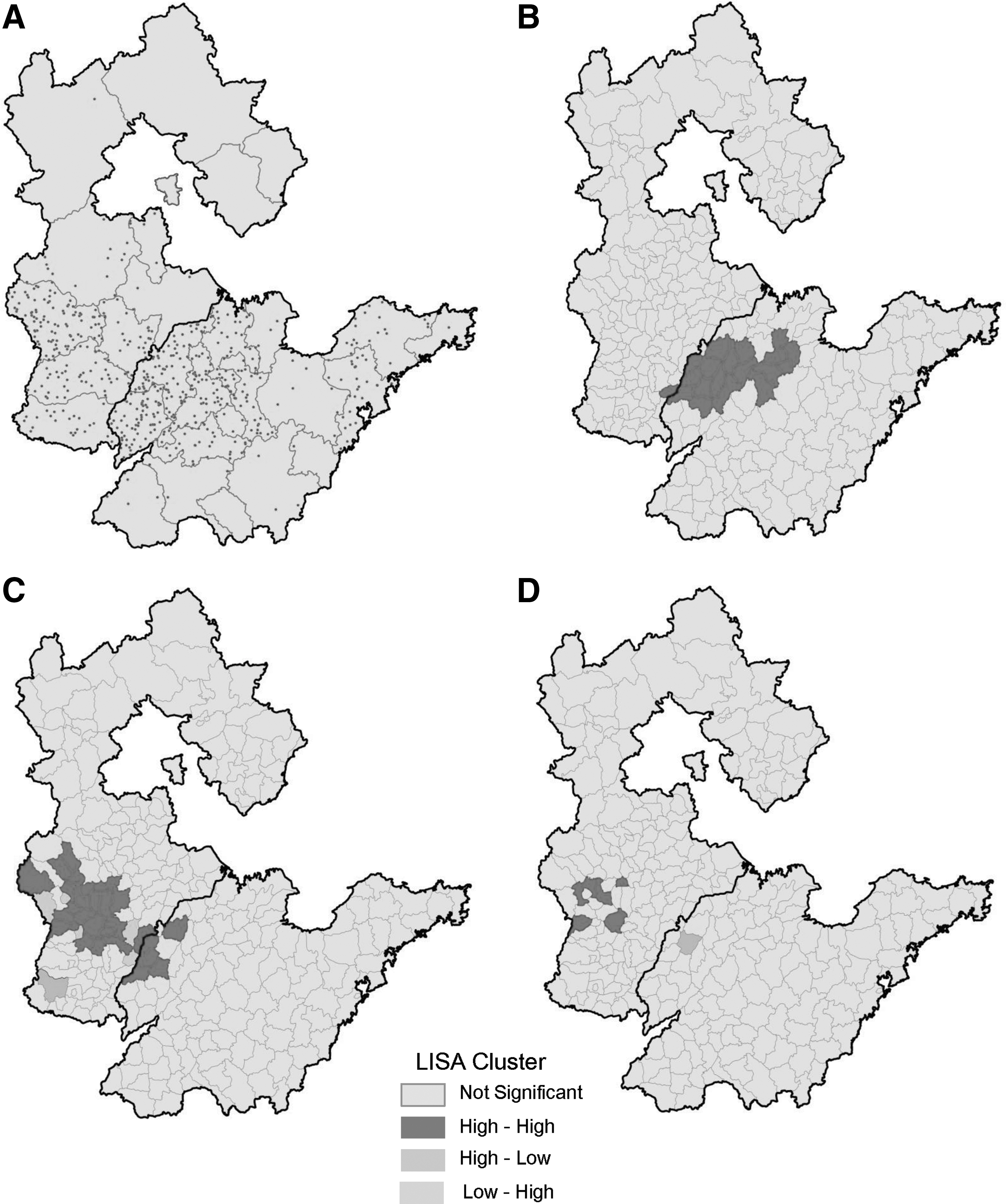
Clusters of JE during the outbreak in northern China from September to November 2013.
Incidence and mortality
In 2013, Shandong and Hebei provinces reported 407 and 234 JE cases, respectively, which were 8 times (407/51) and 47 times (234/5) higher compared with those reported in 2012, respectively. In addition, the 2013 incidence rate was 0.4202/100,000 and 0.3211/100,000 in the two provinces, respectively, and this was significantly higher than the national average (0.1611/100,000). The mortality rate was 0.0114/100,000 and 0.0027/100,000 in Shandong and Hebei, respectively.
Gender and occupation composition
The male to female ratios of JE cases in Shandong and Hebei were 1.02:1 and 1.15:1, respectively. Among all occupation groups, farmers represented the largest JE population in both provinces, accounting for 56.02% and 59.82% of all cases, respectively. The second and third largest JE populations were students (15.72% and 14.52% in Shandong and Hebei, respectively) and scattered children (9.34% and 13.25% in Shandong and Hebei, respectively). Compared with 2012, the number of JE cases in farmers increased by 14-fold (228/15) in Shandong and 70-fold (140/2) in Hebei.
Age group
At the country level, children less than 15 years of age represented the largest population of JE in 2013. In the provinces of Shandong and Hebei, however, the age distribution of JE was significantly different. In Shandong, the JE incidence rate in the 70- to 75-year-old group (0.96/100,000) was comparable to that in the 5- to 10-year-old group (1.00/100,000), which represented the two largest populations among all age groups (Fig. 7). The incidence of JE decreased as age increased from 10 to 35 years, with the lowest incidence rate occurring in those aged between 30 and 35 years (Fig. 7). From the age groups of 35 to 75 years old, the incidence of JE increased gradually, with the 70- to 75-year-old group showing the highest incidence rate (Fig. 7). The incidence of JE in Hebei Province exhibited a similar age distribution, with three age groups (5- to 10-, 50- to 55-, and 55- to 60-year-old) showing the highest incidence rate (>0.5/100,000). In both Shandong and Hebei, adults accounted for most of the cases occurring in the entire population. Specifically, individuals aged more than 15 years accounted for 73.2% and 73.93% of total JE cases in Shandong and Hebei, respectively, compared with the national average of 42.4%. Individuals aged 40 years and older accounted for 59.7% and 47.86% of total JE cases in these provinces, respectively.

Age distribution of JE in Shandong and Hebei in 2013. The age distribution of JE cases in Shandong and Hebei showed a “V” shaped curve. The incidence of adult JE cases aged 40 years and older was significantly higher than the national average (Fig. 2A).
Temporal distribution
According to the temporal distribution of cases from 2011 to 2013 nationwide, the number of JE cases peaked in the month of August (Fig. 2B). In Shandong and Hebei (in northern China), however, the highest number occurred later in 2013 (Fig. 8). The number of JE cases in Shandong increased gradually from the 34th week (late August) and peaked at the 37th week (September 9–15), at which time a total of 102 JE cases were reported. This was followed by two small peaks observed in the 39th and 41st week (early October) of the year. Case numbers began to decline from the 42nd week (mid-October), and only sporadic cases were reported in December (Fig. 8).
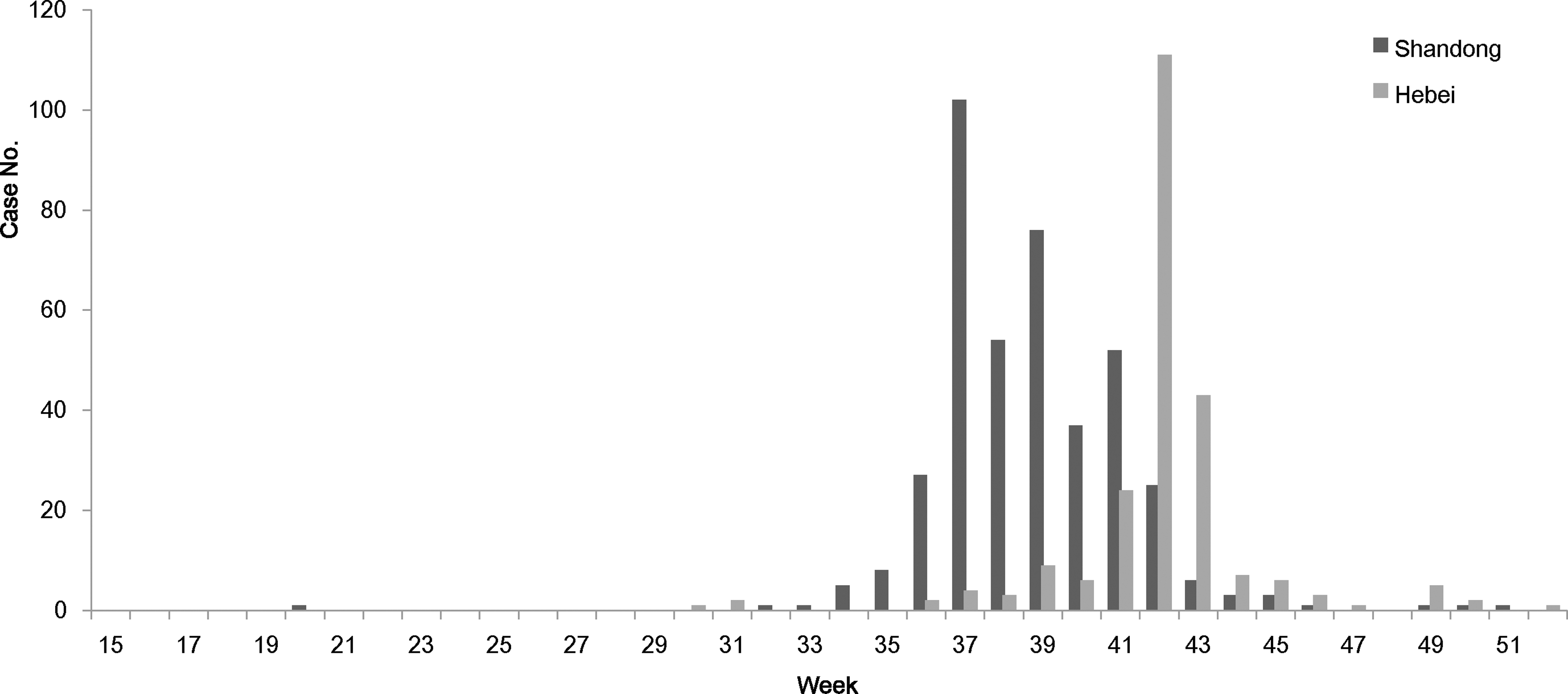
Temporal distribution of JE in Shandong and Hebei in 2013. The peak of JE incidence in Shandong and Hebei lagged behind compared with the previous year; reported cases peaked in mid-September (the 37th week) and mid-October (42nd week) in the two provinces, respectively.
In contrast with the temporal pattern in Shandong, the number of JE cases in Hebei began to increase from the 37th week (mid-September) and peaked at the 42nd week (mid-October). Approximately 111 JE cases were reported in just 1 week within this time period. The case number decreased abruptly to 43 in the 43rd week of 2013 and continued to decline toward the end of the year (Fig. 8).
Discussion
China is a vast country spanning 35° of latitude from south to north. Heilongjiang, the most northerly province in the country, is situated at 55°N, while Hainan province, the most southerly province, is situated at 20°N. Consequently, the northern and southern regions of China differ vastly in terms of geographic and climatic characteristics. In southern China (15–30°N latitude), the average temperature remains relatively high throughout the year with abundant rainfall and well-developed river systems. With such an abundance of water supply, rice is one of the most common agricultural products in the region. Along with other factors, these southern areas provide an optimal breeding ground for mosquitoes, including Culex tritaeniorhynchus, which is the principle vector for JEV (Zheng et al. 2012, Li et al. 2016). In contrast, northern China (30–35°N latitude) is situated in the Northern Temperate Zone, with low average temperature and less rainfall. The dominant crops here are drought-resistant wheat and corn, which do not require a large amount of irrigation. These factors among others make these regions less suitable for mosquito breeding/survival, contributing to relatively lower densities and diversities of mosquito species in northern China (Zheng et al. 2012). These marked differences in geographical and environmental factors led to distinct epidemiological patterns of JE in southern and northern regions of China. Southern China is a highly epidemic area for JE, while the incidence of JE in northern China is significantly lower (Gao et al. 2014, Li et al. 2014, 2016).
JE is an infectious disease of the nervous system that poses a substantial disease burden. Humans are susceptible to JEV infection, and children are the primary population that develop JE. According to statistics reported by the WHO, about 75% of all JE cases occurred in children aged 0–14 years (Campbell et al. 2011). The WHO recommended that children less than 15 years of age living in JE epidemic areas should be vaccinated to prevent infection of JEV and to reduce JE incidence and disease burden.
In 2008, the Chinese government introduced the JE vaccine as part of the EPI, which provides children aged 0–15 years nationwide with free vaccination against JE. A national immunization coverage survey in China revealed that the coverage of first dose of JE vaccine could achieve above 90% and that of second dose was 89.49% (Cao et al. 2012). The EPI program has been ongoing for years, and the implementation of this strategy dramatically improved the rate of vaccination in children and contributed to a remarkable decrease in JE incidence in this population. The JE incidence in the country and that in the 0- to 15-year-old age group differs significantly before and after 2008. The incidence rates dropped from 0.3896/100,000 (nationwide) and 1.7132/100,000 (in those aged under 15 years) for the period of 2004–2008 to 0.1801/100,000 and 0.737/100,000, respectively, for the period of 2009–2014. This suggests that the decrease observed in JE among children, following vaccination, has become the main contributor to the decrease of cases seen at the country level (Li et al. 2016).
The JE-inactivated (P3 strain) and JE-attenuated live (SA14-14-2 strain) vaccines were successfully developed in 1968 and 1988, respectively (Yu 2010). However, due to difficult economic situations, low production capacity, as well as a large population, the demand for JE vaccination in China could not be satisfied at that time. Only a small proportion of adults (born between 1970 and 1980) were immunized with the vaccine as children, leaving the rest of the adult population vulnerable to JEV infection. This may have contributed to the increase of JE in adults during that time period (Gao et al. 2014).
In recent years, several epidemics of adult JE have occurred in northern China. Previous studies have shown that these cases were concentrated in six provinces, including Shanxi, Shaanxi, Henan, Hebei, Shandong, and Gansu (35–40°N latitude). Among these provinces, a large number of adult JE cases were clustered in Shanxi, Shaanxi, and Henan (35–36°N) in 2006 and 2009 (Wang et al. 2007, Li et al. 2016). As demonstrated in this study, the epidemic areas shifted to Shandong and Hebei (36–40°N) in 2013 (Fig. 5), suggesting that the epidemic range of adult JE in the northern region altered over time. Whether other factor(s) apart from immunization exist that may influence the emergence of JE among adults require further investigation. Nonetheless, our data indicate that the prevalence of adult JE cases in northern China is not an accidental event and will likely occur every few years.
Recently, an increasing number of adult cases of JE have also been reported in other parts of East Asia. Due to a mass immunization campaign in the 1960–1970s, very few cases of JE in children were reported in Japan and South Korea (Konishia et al. 2010, Lee et al. 2012). However, sporadic incidence of JE in adults continues to occur in Japan annually (Konishia et al. 2010). In South Korea, a total of 129 JE cases were reported during the period of 2010–2015, of which more than 61% were adults aged 40 years and older. The median age of these cases was found to be 53 years (Sunwoo et al. 2016), and the majority occurred near the capital city, Seoul (latitude 37°N). The pattern of adult JE outbreak in South Korea resembles what was observed in northern China in 2013 (latitude 35–40°N). As such, the reemergence of JE in adults has become a regional public health issue that is no longer limited to China. In 2013, it was a particularly warm year in northern China, especially in Shandong and Hebei, and the warmer period lasted longer than that in 2011 and 2012. Then whether or not geographical and climatic factor(s) have influenced the upsurge of adult JE in these regions (35–40°N) warrants further studies.
JE is a clinically significant mosquito-borne disease caused by JEV. Spread of the virus and therefore JE can be affected by multiple natural and environmental factors (Impoinvil et al. 2011, Miller et al. 2012). The occurrence of JE outbreaks in the adult population is likely influenced by other factors besides the absence of immune barrier/vaccination. Due to the high fatality rate and the disease burden associated with JE, it is important that we continue to advance our understanding of the epidemic characteristics of adult incidence in countries with high prevalence of JE. This may in turn provide further insights into the development of effective prevention and treatment options to improve patient outcomes.
Footnotes
Acknowledgments
This work was supported by the National Key R&D Program of China (2016YFC1201904), the National Natural Science Foundation of China (81501757), the National Key Plan for Scientific Research and Development of China (2016YFD0500300), and the Development Grants of State Key Laboratory of Infectious Disease Prevention and Control (2014SKLID103, 2015SKLID505). The founders had no role in the study design, data collection and analysis, decision to publish, or preparation of the article.
Author Disclosure Statement
No competing financial interests exist.