
Abstract
Background:
Knowledge of the spectrum of presentations and the outcome of congenital brucellosis should expedite diagnosis and improve prognostication.
Methods:
A systematic review of literature of cases of congenital brucellosis was performed on October 10, 2017 (registered as PROSPERO CRD42017072061).
Results:
A case seen by the authors was added to the review, yielding 44 reported cases of which 22 (50%) were from Turkey, Saudi Arabia, or Kuwait. For cases with the gestational age reported, 23 of 37 (62%) were preterm. The species was Brucella melitensis in 35 cases, Brucella abortus in 3 cases and not documented in 6 cases. The diagnosis was based on a positive blood culture from the first day of life in 20 cases (45%). Presentation was usually typical for a bacteremic infant of that GA, but two infants were asymptomatic at diagnosis. There were two recurrences and seven deaths (six in preterm infants), but the role of Brucella infection in the deaths was not clear.
Conclusion:
Brucellosis remains a concern in endemic countries, adversely affecting pregnancy and very rarely causing neonatal infection. Prematurity appeared to be the prime cause of death in neonates with congenital brucellosis.
Introduction
B
Congenital brucellosis results from vertical transmission to the fetus. The spectrum of presenting features and outcomes of congenital brucellosis are not well delineated so a systematic review of the published literature was performed, supplemented by a recent case seen by the authors.
Methods of Systematic Review
Search strategy, selection criteria, and data collection
The electronic databases Ovid Medline (1946–), Ovid Embase (1974–), and Web of Science (Thomson Reuters; 1900–) were searched October 10, 2017 for studies of congenital brucellosis, excluding animal studies (Appendix 1). The World Health Organization website was searched for relevant reports, and a web search conducted using Google. No language or date range restrictions were applied. Reference lists of included studies were searched.
Cases were included if the authors of the case report considered it to be congenital (unless the onset of maternal symptoms was postpartum). Cases were excluded if the authors of the case report concluded that the infant acquired Brucella from consumption of breast milk or nonhuman milk or from blood products. The risk of bias of the studies could not be assessed as the largest case series had three patients.
Data collected on cases that met the inclusion criteria included the timing of onset of maternal symptoms compatible with brucellosis, maternal treatment for brucellosis before delivery, and infant gestational age (GA), birthweight, treatment for brucellosis, and complications.
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (
Case Report
A baby boy was born to a Saudi 25-year-old G1 P0 at 26 weeks' gestation (845 g birth weight). He required resuscitation for apnea followed by mechanical ventilation. The first dose of surfactant was given and the infant was transferred to the neonatal intensive care unit.
Chest radiograph was compatible with mild respiratory distress syndrome. Complete blood count with differential was unremarkable, except for macrocytic anemia (hemoglobin was 99 g/L). A blood culture was obtained and intravenous ampicillin and gentamicin started for possible early onset sepsis.
On day 3 of life, the patient was extubated to nasal continuous positive airway pressure and then to nasal cannula at 7 days of age. Blood culture obtained at admission grew Gram-negative coccobacilli after 3 days of incubation.
The mother did not have a history of abortion. She experienced intermittent hip pain during pregnancy but no fever or other symptoms. She disclosed a history of raw camel milk ingestion in the first trimester and reported that one of her sisters had been recently treated for brucellosis. Therefore, congenital brucellosis was suspected and eventually confirmed by a positive blood culture for Brucella (not further identified). Infant Brucella serology was negative. Breastfeeding was stopped. Ampicillin was discontinued and gentamicin continued for a total of 2 weeks. A 6-week course of oral rifampicin and trimethoprim/sulfamethoxazole (TMP/SMX) was started. The infant had an uneventful clinical course with the exception of Escherichia coli sepsis at 40 days of age, treated with amikacin for 2 weeks. The infant was discharged home at 73 days of age and showed normal development at 19 months of age.
The mother was referred to an adult infectious diseases physician. Brucellosis was confirmed by serology and treatment started. A blood culture was never obtained.
Results of Systematic Review
The search yielded 233 unique titles. Thirty-five studies met the inclusion criteria (Fig. 1). Including our case, there are 44 cases that met the inclusion criteria, dating back to 1941 (Table 1). Nine cases were reported from Turkey, eight from Saudi Arabia, five from Kuwait, five from the United States, four from Peru, three from Greece, two from each of Argentina, Israel, France, and Iran, and one from each of Spain and Jordan. Of the 37 reported cases, where GA was provided, 23 (62%) were preterm (born before 37 weeks GA). The species was Brucella melitensis with the exception of our case and three others, where the species was not reported (Shamo'on and Izzat 1999, Dogan et al. 2010, Elkiran et al. 2010), two cases diagnosed on the basis of infant serology alone (Hagebusch and Frei 1941, Ceylan et al. 2012), and three cases of Brucella abortus (Oran et al. 1983, Giannacopoulos et al. 2002, Alnemri et al. 2017).
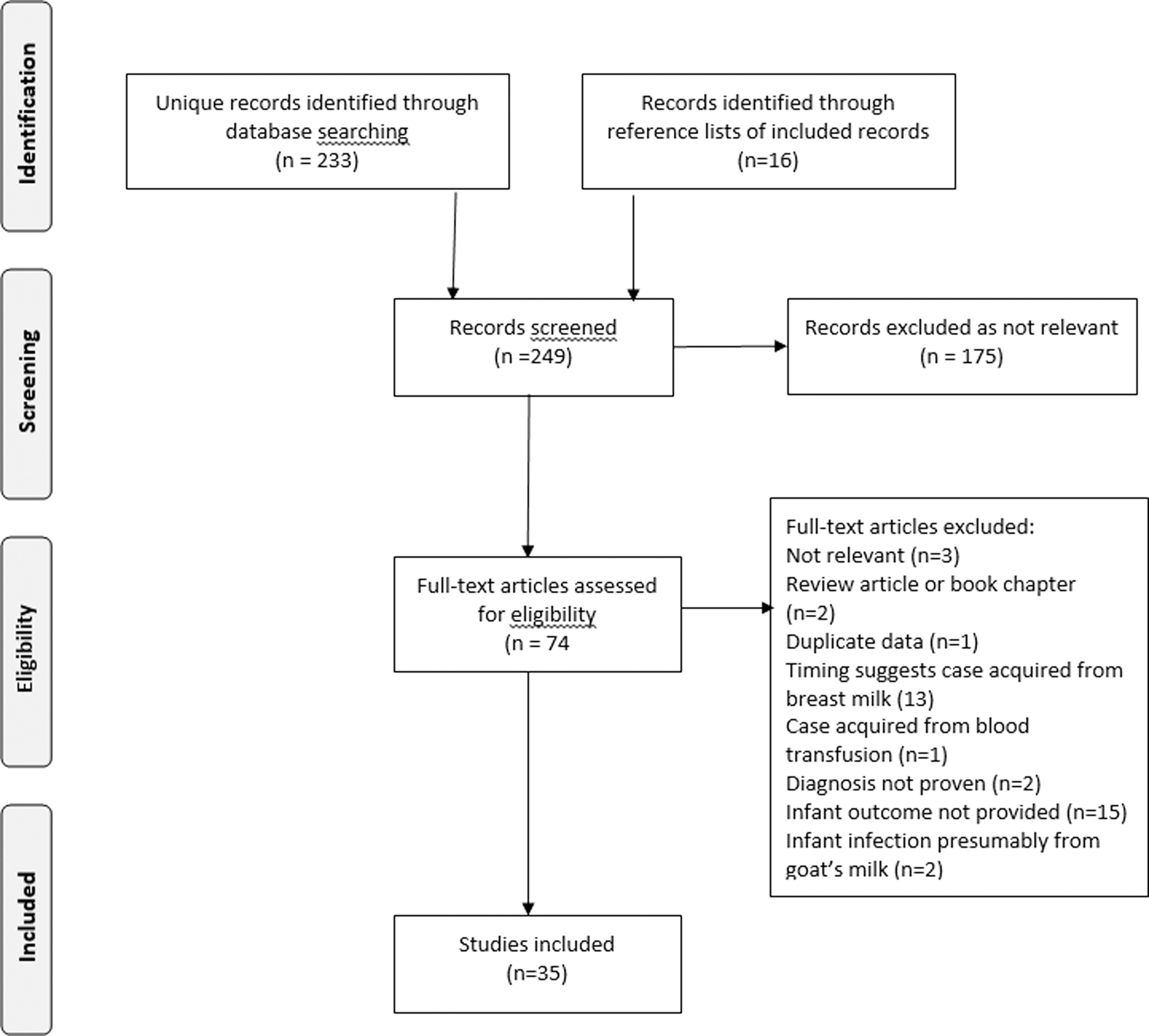
Flow chart for systematic review.
One of 24 infants born to women with brucellosis during pregnancy had congenital brucellosis, but the timing of maternal infection or treatment is not provided.
CSF, cerebrospinal fluid; GA, gestational age; NR, not reported; TMP/SMX, trimethoprim/sulfamethoxazole.
The clinical presentation was usually typical for a bacteremic infant but three term infants were reported to be asymptomatic on days 13 (Singer et al. 1991), 28 (Akin et al. 2015), and 30 (Carbajo-Ferreira et al. 1995) when blood cultures that grew Brucella were sent due to maternal brucellosis. Another infant received 11 days antibiotics for suspected Haemophilus influenzae bacteremia at birth and remained well despite again being bacteremic with B. melitensis at 52 days of age when the original organism was identified as B. melitensis (Cacace et al. 2013).
Unusual presentations included myocarditis at 3 months of age (Elkiran et al. 2010) and hydrocephalus detected at 1 month of age with B. melitensis first detected in cerebrospinal fluid (CSF) at 8 months of age in the face of a maternal history of goat cheese consumption and symptoms compatible with brucellosis during pregnancy (Drutz 1989).
Details on how the diagnosis of congenital brucellosis was made were not provided for four cases (Vilchez et al. 2015). In the remaining 40 patients, the diagnosis was based on positive blood cultures (N = 36; of which the culture was from umbilical cord blood in a single case) (Olivares 1954), serology alone (N = 3) (Hagebusch and Frei 1941, Al-Amoudi 1995, Ceylan et al. 2012), or a positive CSF culture (N = 1) (Drutz 1989) (only one other infant had a documented positive CSF culture) (Oran et al. 1983). For the 35 cases with bacteremia (excluding the case with cord blood bacteremia as this was clearly congenital), 22 were presumed to be congenital as the positive blood culture was from day 1 of life in 20 cases and day 5 in 2 cases (Koklu et al. 2006, Poulou et al. 2006) Table 2. Later diagnosis based on a positive blood culture on days 21 (Miller 1993) and 85 (Labrune et al. 1990) in two preterm infants and at 27 days of age (Giannacopoulos et al. 2002), 30 days (Carbajo-Ferreira et al. 1995), and 3.5 months (Pinto and Al-Suweih 1996) in three term infants were presumed to be congenital as the infants did not receive maternal breast milk. Later diagnosis based on a positive blood culture on day 13 (Singer et al. 1991), day 20 (Lubani et al. 1988), day 26 (Lubani et al. 1988), day 28 (Akin et al. 2015), and at 3 months of age (two cases) (Varon et al. 1990, Elkiran et al. 2010) in breastfed infants were assumed to be congenital as there was suspected or proven maternal brucellosis in pregnancy. The final two cases were based on a positive blood culture and on day 25 (Imani et al. 2007) and day 39 (Glocwicz et al. 2010) with breastfeeding history not provided.
One of the 21 cases had positive cultures from umbilical cord blood only.
Multiple antibiotic regimens were employed with durations varying from 21 to 90 days in infants who survived (Table 1). Infant outcome was available for 40 cases of which 8 (20%) died in the neonatal period, including one term infant; none had evidence of persistent brucellosis at the time of death, except for 2 infants who died within 24 h of birth (Oran et al. 1983, Sahin et al. 2015) (Table 1). Two infants had recurrent disease. The first was an asymptomatic term infant treated at 1 month of age with 21 days TMP-SMX and 3 months rifampin for B. melitensis bacteremia. The recurrence presented as septic arthritis of the knee at 12 months of age, treated with 5 days gentamicin and 42 days TMP-SMX and rifampin with no further recurrences (Carbajo-Ferreria et al. 1995). The other recurrence was in a preterm infant (25 weeks GA) who was bacteremic at birth, treated with gentamicin and ampicillin for 21 days, bacteremic 7 days later, and died on day 85 while still being treated (al-Eissa and al-Mofada 1992). Long-term sequelae were not described in survivors.
Discussion
Brucellosis is caused by Gram-negative, intracellular coccobacilli with goats, camel, and sheep (B. melitensis); swine (Brucella suis); cattle (B. abortus); and dogs (Brucella canis) being the major reservoirs of the disease. B. melitensis is the most important species for human brucellosis, but other species, including B. abortus, B. suis, B. canis, and novel marine Brucella have also been associated with human cases. Human brucellosis affects all age groups with variable incidence according to the geographic location and the strain.
Brucellosis is commonly acquired in Mediterranean countries, the Middle East, the Arabian Peninsula, Central and South America, Asia, and Africa. Saudi Arabia is still considered to be endemic for brucellosis despite great efforts by the Saudi Ministry of Agriculture to implement a regulatory control of imported livestock and compulsory brucellosis vaccinations for cattle. However, there is a lag in compliance with national and international policies of animal screening and with quarantine rules such as the prohibition against mixing different species of animal herds in the same pasture. Owners resist slaughtering infected animals. Low levels of public awareness about the seriousness of brucellosis in humans and the traditional belief of the great benefit of ingesting raw milk (especially camel milk) are other factors that contribute to the endemicity of the disease in Saudi Arabia (Alshaalan et al. 2014, Aloufi et al. 2016).
Pregnancy leads to impaired immunological status, and infection with Brucella can lead to devastating obstetric outcomes (Vilchez et al. 2015), including congenital infection. At one point it was believed that adverse pregnancy outcomes associated with human brucellosis should be uncommon due to the absence of erythritol in the human placenta (Nuri et al. 2011, Al-Tawfiq and Memish 2013) (a sugar present in animal placentas that promotes Brucella growth). Another theory was that amniotic fluid contains anti-Brucella activity (Al-Anazi and Al-Jasser 2013). However, many reports describe apparent increased rates of spontaneous abortion, intrauterine fetal death, and preterm birth for women with brucellosis during pregnancy (Arenas-Gamboa et al. 2016).
The incidence of published cases of congenital infection is surprisingly low considering that all pregnant women in endemic countries face potential exposure to Brucella. Potential explanations include maternal immunity from prior infection, fetal loss with acute infection, or failure to diagnose or report congenital infection. Four of the cases in the current review occurred in women who were thought to have completed therapy for brucellosis during pregnancy (Labrune et al. 1990, Shamo'on and Izzat 1999, Giannacopoulos et al. 2002, Imani et al. 2007). It is not clear if the problem was inadequate therapy versus relapse or reinfection. Although it is difficult to establish, it seems likely that recognition and treatment of infection early in pregnancy decreases the incidence of spontaneous abortion, intrauterine fetal death, and congenital infection. The clinical manifestations of brucellosis in pregnancy are similar to those in nonpregnant women; fever, chills, sweating, arthralgia, and hepatosplenomegaly are the most commonly encountered presentations (Al-Anazi and Al-Jasser 2013, Vilchez et al. 2015). However, symptoms are nonspecific and can be mild with 9 of the 44 mothers of cases in the current review (20%) denying compatible symptoms. The majority of infected pregnant women report a history of unpasteurized milk consumption or contact with animals (Vilchez 2015, Ali et al. 2016). Thus, potential occupational exposure and family history of brucellosis should be obtained during prenatal care in endemic areas.
All but one of the seven deaths in this review occurred in a preterm infant. The degree to which Brucella contributed to morbidity or mortality is difficult to ascertain given the extreme prematurity of many infected infants, but it seems likely that maternal brucellosis sometimes precipitates preterm delivery and the accompanying adverse long-term outcomes.
Transplacental transmissions from a bacteremic mother, exposure to maternal blood, urine, or genital secretions during delivery are the proposed routes of transmission for congenital brucellosis. Half of the cases in the current review were bacteremic on the day of birth, suggesting the former mechanism. As mentioned previously, presumed transmission through breast milk is well documented. There is a single case presumably acquired from a blood transfusion (al-Kharfy 2001). Two other infants had positive blood cultures following exchange transfusions, but neither developed symptoms nor Brucella antibodies (Akcakus et al. 2005). Cases with symptom onset in the first week of life are presumably congenital as although the incubation period of Brucella in humans can vary from <1 week to months, it is typically 2–4 weeks (Gul and Khan 2007). Delayed recognition of congenital infection can occur with preterm infants as the manifestation of brucellosis overlap with other diseases of prematurity. Term infants with onset of symptoms beyond 1 week of age may have acquired Brucella through breastfeeding or ingestion of nonhuman milk but congenital infection can also have a delayed presentation (Carbajo-Ferreria et al. 1995).
The clinical manifestations of brucellosis in the neonate are nonspecific and it is very difficult to distinguish brucellosis clinically from other bacterial infections. Fever, symptoms of anemia or features of bone marrow failure, jaundice, respiratory distress, vomiting, irritability, convulsions, and hepatosplenomegaly have all been described (Al-Anazi and Al-Jasser 2013). The role of Brucella in myocarditis (Elkiran et al. 2010) and hydrocephalus (Drutz 1989) is difficult to determine; both occurred in infants who could have acquired Brucella from breast milk. Two of the infants in the current review were reported to be well at day 13 (Singer et al. 1991) and day 30 (Carbajo-Ferreira et al. 1995) and were investigated only because of a maternal diagnosis of brucellosis; presumably they would have eventually manifested signs of infection.
In most cases, the diagnosis of congenital brucellosis was made by the unexpected isolation of Brucella from blood culture obtained from a sick neonate with suspected sepsis. Serologic tests are also important methods for clinical diagnosis but should be interpreted judiciously because of transplacental passage of maternal IgG antibodies (Yagupsky 2010). A negative serologic test should never exclude the diagnosis, particularly in preterm neonates who may not have mounted their own antibody response nor received transplacental antibodies.
A wide array of antimicrobial regimens was used for treatment of neonatal brucellosis in this review with a recurrence documented in 2 of 38 cases. The first recurrence could have been due to noncompliance as the mother was noncompliant with her own therapy during pregnancy (Carbajo-Ferreria et al. 1995). The second recurrence occurred 7 days following a 21-day course of ampicillin and gentamicin given in hospital (al-Eissa and al-Mofada 1992). There is not thought to be aminoglycoside resistance (Al-Tawfiq and Memish 2013), but beta-lactams may lack efficacy against this intracellular organism as they do not penetrate macrophages. Initial therapy with intravenous aminoglycosides for 5–14 days combined with rifampicin and TMP/SMX orally to complete 6–8 weeks is a commonly described regimen, but many cases in the review were cured without an aminoglycoside. One caveat is that TMP/SMX is relatively contraindicated in the first 2 months of life because it can displace indirect bilirubin from albumin. Quinolones and doxycycline are sometimes used for treatment of brucellosis in adolescents but their safety in infants has not been established. There are no cases where breastfeeding was reported to have been continued following diagnosis of congenital infection; it is possible that continuation would be safe if mother and infant are both treated.
The main limitation of this study is that it seems likely that a minority of cases of congenital brucellosis are reported. Our search may have missed cases reported in local medical journals. Some of the cases attributed to congenital infection could have been acquired from breast milk or blood transfusion.
Conclusion
In conclusion, brucellosis remains a serious threat and public health concern for those living in endemic areas. Congenital brucellosis is a very rare cause of early onset neonatal sepsis but should be considered in neonates born to women at risk. Physicians dealing with women who lived in endemic areas during pregnancy should maintain a high index of suspicion when they present with unexplained symptoms, especially for those with social and occupational risk for brucellosis as early diagnosis and prompt therapy have been shown to improve the outcome. Education for pregnant women living in endemic areas about avoidance of unnecessary exposure to sheep, goat, and camels and consumption of unpasteurized dairy products is highly recommended.
Footnotes
Acknowledgment
This work was supported by the Alberta SPOR SUPPORT Unit Knowledge Translation Platform.
Author Disclosure Statement
No competing financial interests exist.