
Abstract
Background:
Detection of local dengue transmission requires an aware and engaged medical community, as health care providers are the front line of public health surveillance. To assess the knowledge, attitude, and practice about dengue, an online survey was distributed among Arizona health care providers during 2014 and 2015.
Materials and Methods:
The survey consisted of a total of 10 knowledge, attitude, and practice questions divided as follows: 5 knowledge questions, 2 attitude questions, and 3 practice questions. The link to the Qualtrics survey was distributed through the Arizona Health Alert Network to a total of 4582 e-mail addresses, of which 335 participants opened the survey, and 196 completed and submitted their responses.
Results:
Less than half the respondents reported choosing the right dengue diagnostic test (40.4%) or understanding the epidemiology of dengue in Arizona (40.9%). Slightly more than half the respondents reported frequently asking for travel history (59%), and three-fourth of them would notify the local health department on suspicion of a dengue patient (76.1%). Survey score was associated with providers specialized in infectious diseases (1.88, 95% CI: 0.42–3.33, p = 0.01), medical doctors or doctors of osteopathic medicine (1.82, 95% CI: 0.98–2.65, p < 0.0001), and respondents who reported to have heard about the increase in dengue cases in Sonora (Mexico) in fall 2014 (1.51, 95% CI: 0.67–2.34, p = 0.0005), indicating better survey performance.
Conclusions:
These results indicate that education for health care providers on dengue should be improved particularly among general practice noninfectious disease providers who might be the first point of care for dengue patients. Findings suggest that additional training on clinical management, asking travel history, and notifying the local health department on suspicion of a dengue patient are needed.
Introduction
Dengue viruses can cause serious and potentially fatal acute febrile illness. An estimated 390 million cases of dengue infection occur annually worldwide (Bhatt et al. 2013), with infections increasing nearly 30-fold in the past 50 years (WHO 2009). An estimated 500,000 of these infections are cases of severe dengue, and 22,000 result in fatalities annually (Brady et al. 2012, Bhatt et al. 2013). Dengue is caused by infection with any one of four viral serotypes: DENV-I, DENV-II, DENV-III, or DENV-IV, which are transmitted by Aedes (Ae.) species mosquitoes, primarily Aedes aegypti and Aedes albopictus.
In the United States, dengue outbreaks have occurred in the last 15 years in Florida (CDC 2010), Texas (Abell et al. 2007, Thomas et al. 2016), and Hawaii (Johnston et al. 2016). The disease is endemic in Mexico, with the annual number of dengue cases increasing from 1714 cases in 2000 to 15,424 in 2011 (Dantes et al. 2014). The Mexican state of Sonora, which borders Arizona, has also seen an increase in the number of dengue cases in 2010 and in 2014, when it reached an incidence of 100 cases per 100,000 population (DGE 2014).
Beginning in September 2014, an increase in locally acquired dengue cases in Sonora, Mexico, was reported in the border region with Arizona. Between December 2014 and January 2015, a binational dengue outbreak was identified, with 52 cases detected in San Luis Rio Colorado, Sonora, and 70 cases reported in the neighboring Arizona border county of Yuma (Jones et al. 2016). This outbreak represented a ninefold increase in reported cases among Arizona residents compared with 10 dengue cases reported in 2010 and 2012 (1994–2009 median of 2 cases annually). Despite the increase in cases, no locally acquired cases in Arizona were identified as all cases reported travel to Mexico within 14 days before symptom onset (Jones et al. 2016).
Arizona is home to a dengue-competent mosquito vector, Ae. aegypti, which is known to be well-established across parts of the state (ADHS 2016). Although the complete range of Ae. aegypti in Arizona is unknown, current and historical data suggest substantial establishment in central and southern Arizona, including the Arizona-Sonora border region. The mosquito's presence in Arizona, along with the northward expansion of dengue virus infections toward the border, enhances the likelihood of both locally acquired and travel-associated dengue cases in Arizona. Early detection of locally acquired cases is particularly important, to promptly initiate a public and environmental health response to avoid the spread of the disease in Arizona. Identification of locally acquired dengue cases requires an aware and engaged medical community; as the front line of public health surveillance, health care providers start the process of outbreak investigation and control by reporting suspected cases to local public health officials. To detect locally acquired cases, health care providers should have detailed knowledge of dengue epidemiology, symptoms, appropriate diagnostic tests, and reporting procedures.
To better understand the knowledge and behaviors of health care providers in Arizona with respect to dengue, we administered a knowledge, attitudes, and practices (KAP) survey to Arizona providers between December 2014 and March 2015, starting soon after the identification of the binational dengue outbreak in Yuma County. The goals of this survey were to assess providers' knowledge of dengue epidemiology, symptoms and transmission, confidence in diagnosing and treating the disease, and practices when treating a patient with suspected dengue virus infection. A few studies have been published on the knowledge, attitudes, or practices of providers with respect to dengue in the United States, specifically in Puerto Rico (Tomashek et al. 2014), in Florida (Doblecki-Lewis et al. 2016), and in Texas (Adam et al. 2017). However, our study is unique as it surveyed physicians in Arizona, a state that has not yet reported local dengue transmission, but that is at high risk of dengue emergence.
Materials and Methods
The survey consisted of a total of 10 multiple choice KAP questions divided as follows: 5 knowledge questions (clinical symptoms, transmission, diagnosis, treatment, and epidemiology), 2 attitude questions (confidence in diagnosis and treatment), and 3 practice questions (reporting, asking for travel history, and ordering of laboratory testing). In addition, an eight-question demographics section gathered information about the participants' county of practice, number of years practicing in Arizona, patient demographics, medical specialty, and type of health care practice.
Qualtrics software (Qualtrics, Provo, UT) was used to collect responses. A link to the survey was distributed thrice through the Arizona Health Alert Network, a tool used by the Arizona Department of Health Services (ADHS) to distribute important alerts to public health officials and health care professionals and to ADHS Division of Licensing e-mail lists, in December 2014, January 2015, and March 2015. These lists had a total of 4582 e-mail addresses, which included: ∼3000 points of contacts for licensed medical facilities, 1128 independent health care providers, 12 medical organizations, 250 hospital infection preventionists, and 192 emergency department directors. However, it is difficult to accurately determine the number of unique providers reached as some e-mails might have reached nonclinical or nonpracticing health care workers and some organizations might have further disseminated the link to their individual members.
This project was evaluated by the Arizona Human Subjects Review Board and found to be a nonresearch activity (HSRB 16-0042).
By the end of the survey period, 335 participants had opened the survey, and 196 completed and submitted their responses, corresponding to a 4.3% response rate (196/4582). Only respondents involved in direct patient care were included in the analysis (n = 188), excluding, for example, medical students and pharmacists. Differences in clinical degree type were analyzed by grouping doctors of medicine (MDs) or doctors of osteopathic medicine (DOs) (n = 106) and nurse practitioners (NPs) or physician assistants (PAs) (n = 39); registered nurses or nurses holding a bachelor of science in nursing (n = 15) and respondents with other or missing degrees (n = 6 and 22, respectively) were excluded from this component of the analysis due to the small numbers of these respondents.
To analyze a respondent's overall performance, each answer to the 10 KAP questions was given a point value of 1 (inadequate knowledge), 2 (adequate knowledge), or 3 (high knowledge) (see Supplementary Table S1 for details); an overall KAP score, ranging from 10 to 30, was calculated for each respondent as the sum of points from the 10 questions. For categorical variables, chi-squared test or Fisher's exact tests (for n < 21) were used to identify differences. t-Tests were used for comparisons of mean KAP scores between degrees or other characteristics. Associations with p < 0.05 were considered significant. Stepwise multivariate linear regression was used to identify independent predictors of KAP score, and predictors with p < 0.05 were retained in the final model. Data were analyzed using SAS 9.3 software (Institute, Inc., Cary, NC).
Results
Of the 188 respondents included in the final analysis, the majority (n = 106, 64%) were MDs or DOs; 22 had missing degrees. The most commonly reported specialties were family medicine (24%), pediatric medicine (18%), or emergency medicine (15%); practice locations were mainly private offices or clinics (48%) or hospitals (32%) (Table 1). The majority of the participants had practiced in Arizona for more than 10 years (57%), practiced in an urban county (73%), and practiced in a county not bordering Sonora, Mexico (65%). Participants were located throughout Arizona (11 of 15 counties), although the majority were from Maricopa (42%) and Pima (31%) counties (Fig. 1). Maricopa and Pima counties are the most populated counties in Arizona, making up ∼60% and 15% of the state's population, respectively, and are home to the top 2 most populated cities in the state (Phoenix and Tucson). Both cities are only a few hours away from the United States–Mexico border (181 miles for Phoenix and 68 miles for Tucson), so the population at risk of acquiring dengue from across the border and importing the disease in the state is potentially very high.
Characteristics of the Health Care Professionals Included in the Analysis (n = 188)
Percentages exclude missing values.
“Other” specialty includes: optometry, geriatrics, obesity medicine, hospitalist, dermatology, pain management, international practice/travel medicine.
CDC/NNDSS Clinical dengue case definition: fever as reported by the patient or health care provider and the presence of one or more of the following signs and symptoms: nausea/vomiting, rash, aches and pains, tourniquet test positive, leukopenia (a total white blood cell count of <5000/mm3), or any warning sign for severe dengue (abdominal pain or tenderness, persistent vomiting, extravascular fluid accumulation, mucosal bleeding at any site, liver enlargement >2 cm, increasing hematocrit concurrent with rapid decrease in platelet count) (WHO, 2009).
DO, doctor of osteopathic medicine; MD, doctor of medicine; NP, nurse practitioner; PA, physician assistant; RN, registered nurse; BSN, bachelor of science in nursing.
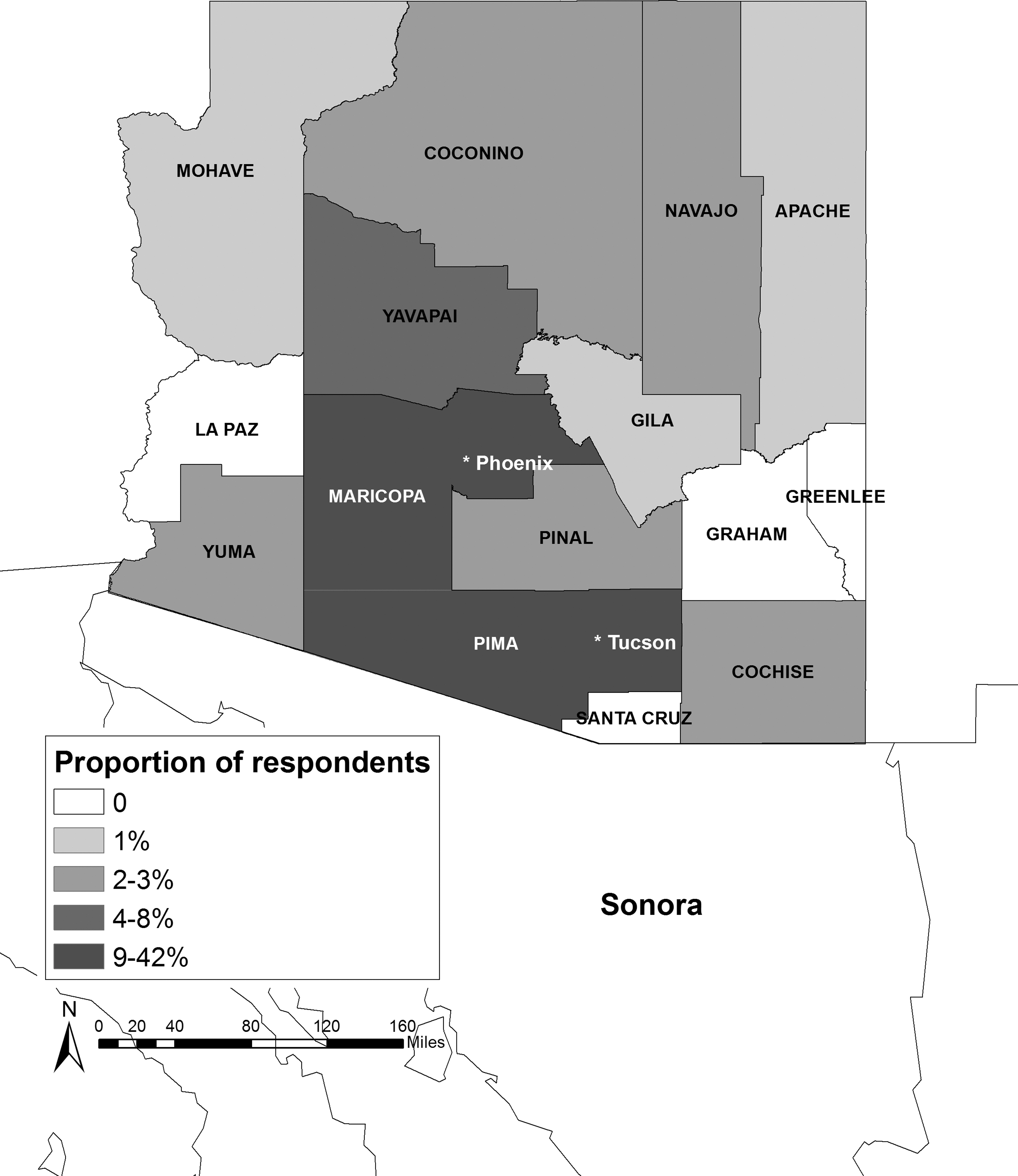
Map of Arizona showing the percentage of survey respondents by county of practice.
Half of respondents reported a low proportion (1–24%) of primarily Spanish speaking patients; only 10% reported that >50% of their patients were primarily Spanish speaking. Approximately 11% of respondents reported serving a predominantly Native American population. Few (9%) reported seeing a patient in the past year that met the CDC/NNDSS clinical dengue case definition [“acute onset of fever plus two or more of the following signs or symptoms: headache, retro-orbital pain, myalgia, arthralgia, rash, hemorrhagic manifestation, leukopenia, and not fitting another diagnosis” (NNDSS 2010); Table 1].
In questions about knowledge of dengue symptoms and transmission, the majority of respondents correctly identified common symptoms of dengue (88% identified fever and 56% hemorrhagic manifestations), the correct route of transmission (89% reporting mosquito bite as possible transmission route), and appropriate treatment (64% reporting intravenous [IV] fluids) (Table 2). Respondents were less knowledgeable about geographic areas with active dengue transmission and clinical and laboratory diagnostic techniques (Fig. 2 and Table 2). Specifically, 41% of the respondents incorrectly reported that the Arizona border region (e.g., Yuma, AZ; Nogales, AZ; Douglas, AZ) was endemic for dengue virus; this region has reported only travel-associated cases to date. There was also a notable lack of knowledge about the appropriate diagnostic methods for dengue virus infection, with ∼60% of respondents unable to identify that ELISA (IgM/IgG) should be used ≥5 days after symptom onset and PCR should be used <5 days from symptom onset (Table 2). Participants also reported low confidence in diagnosis and treatment of patients with dengue virus infection, regardless of whether it was a mild case (35% confidence in diagnosis and 44% confidence in treatment) or a severe case (44% and 26% confidence for diagnosis and treatment, respectively). More than half of respondents reported that they regularly asked patients about travel history (60%) and would notify public health partners about suspected dengue cases (76%) (Fig. 2 and Table 2).
Dengue Knowledge, Attitude, and Practice Among All Respondents (Selected Questions) (n = 188)
Multiple answers allowed.
IV, intravenous.
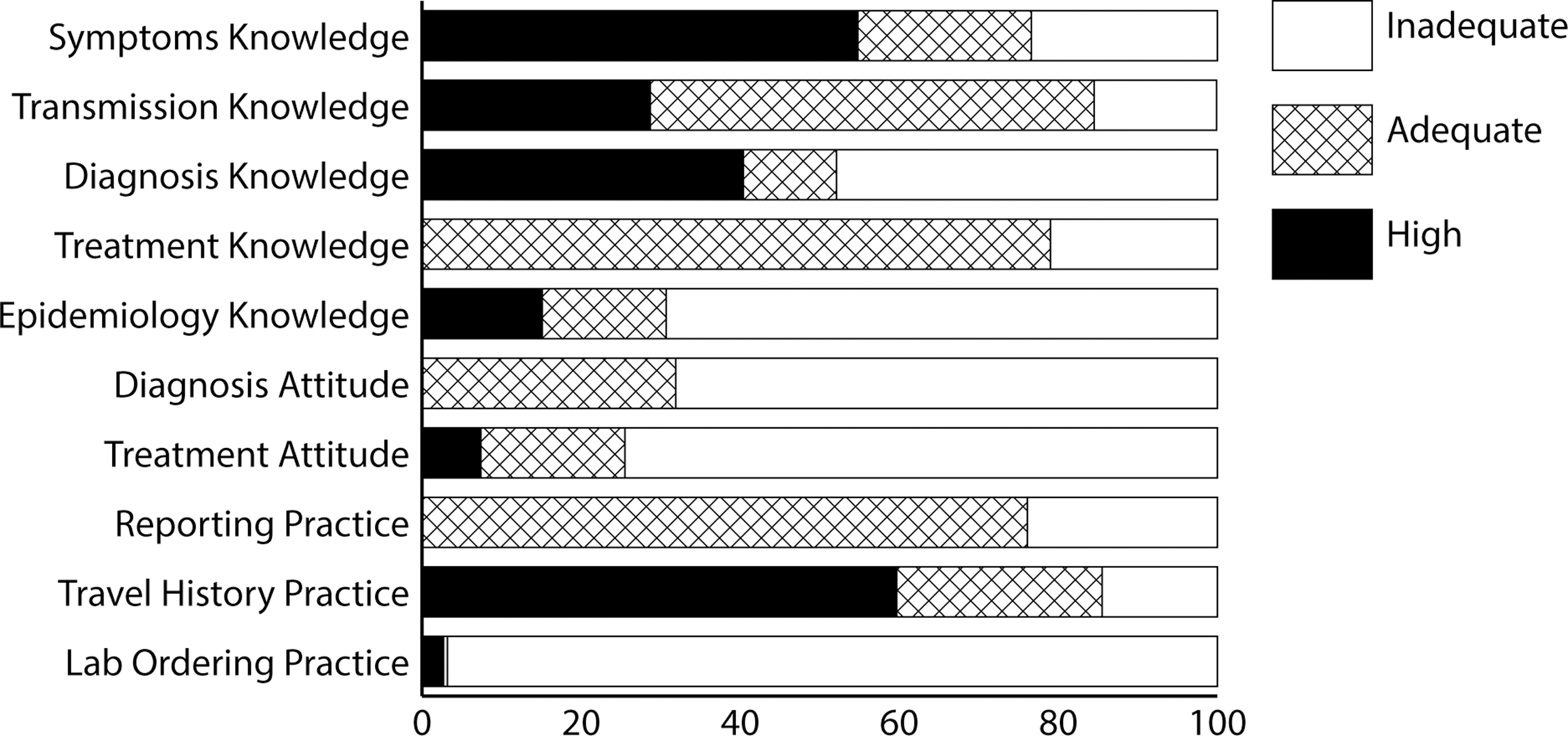
Overview of respondents' knowledge and gaps (n = 188). Proportion of respondents reporting high, adequate, and inadequate knowledge for the 10 KAP questions. KAP, knowledge, attitudes, and practices.
When results were compared by respondents' degree, DO/MDs had higher scores than NP/PAs in the knowledge and attitude questions. Specifically, NP/PAs less frequently identified hemorrhagic manifestations as a sign or symptom of dengue (33% vs. 68%, p < 0.001) (Table 3). They also less frequently reported that dengue can be transmitted through blood transfusions (36% vs. 61%, p = 0.006) or in utero (20% vs. 42%, p = 0.011). The correct diagnostic tests were less frequently reported by NP/PAs than by DO/MDs (13% vs. 55%, p < 0.001) and IV fluids less frequently recognized as a common dengue treatment (56% vs. 74%, p = 0.03). The KAP score was significantly different between DO/MDs and NP/PAs, with DO/MDs performing better (mean of 20.19, 95% CI 19.5–20.8 for DO/MDs vs. 17.70, 95% CI 16.8–18.5 for NP/PAs, t-test p < 0.001).
Differences in Dengue Knowledge, Attitude, and Practice by Respondent's Degree
Comparison of MD and DO to NP and PA.
Chi-square or Fisher's Exact tests (for n < 21).
Providers who reported hearing about the increase in dengue cases in Sonora, Mexico, in fall 2014 performed overall better than those who had not (n = 101, mean KAP score 17.3, 95% CI 16.8–17.8 vs. mean 15.4, 95% CI 14.6–16.1, t-test p = 0.01). Specifically, this group of providers more frequently identified the correct diagnostic tests (50% vs. 30%, p < 0.001), correctly reported IV fluids as common treatment for dengue (75% vs. 52%, p = 0.001), more frequently asked patients for travel history (70.2% vs. 46.4%, p = 0.001), and would notify the local health department about a patient with suspected dengue virus infection (84% vs. 68%, p = 0.009) (Table 4). However, this group also more frequently believed, incorrectly, that dengue virus can be locally acquired on the Arizona side of the United States–Mexico border region (56% vs. 23%, p < 0.0001). When asked about sources of the information regarding the increase in dengue cases in Sonora, the Arizona Health Alert Network (37/101) was most frequently mentioned, followed by the local health department (36/101), the mass media (34/101), and the local hospital (21/101).
Differences in Dengue Knowledge, Attitude, and Practice Between Respondents Who Heard About the Increase in Dengue Cases in Sonora (Mexico) in Fall 2014 Versus Those Who Had Not (n = 185)
Chi-square or Fisher's Exact test (for n < 21).
Respondents serving predominantly Native American populations more commonly reported the belief that dengue virus can be transmitted through close personal contact (21.0% vs. 5.3%, p = 0.03).
When analyzing the overall performance of the 188 respondents, three factors were identified as independent predictors of KAP score. These were: specializing in infectious diseases (parameter estimate = 1.88, 95% CI 0.42–3.33, p = 0.01), being a DO/MD (parameter estimate = 1.82, 95% CI 0.98–2.65, p < 0.0001), and having heard of the increase in dengue cases in Sonora (Mexico) in fall 2014 (parameter estimate = 1.51, 95% CI 0.67–2.34, p = 0.0005).
Among DO/MDs, predictors of KAP score were: specializing in infectious diseases (parameter estimate = 1.90, 95% CI 0.25–3.55, p = 0.024) and having seen patients meeting the dengue clinical case definition in the previous year (parameter estimate = 2.20, 95% CI 0.52–3.89, p = 0.01). Among NP/PAs, practicing in border counties was the only predictor of KAP score (parameter estimate = 2.98, 95% CI 0.61–5.36, p = 0.015). NP/PAs practicing in border counties had a significantly higher mean KAP score than their counterparts practicing in nonborder counties (mean KAP score 17.6, 95% CI 16.9–18.2, vs. 14.6, 95% CI 13.7–15.6, p = 0.02). Interestingly, this group of providers did not report seeing any patients meeting the clinical case definition for dengue since October 2014, nor did they have more years of practice, or report hearing more often about the increase of dengue in Sonora than NP/PAs from nonborder counties.
Discussion
The results of our survey suggest that responding Arizona practitioners tend to be aware of and have some basic knowledge about dengue. However, incorrect responses were sometimes reported, suggesting that education on these topics is still important. In addition, most respondents did not feel confident in diagnosing or treating dengue and had poor knowledge of the appropriate diagnostic tests to perform. The analysis also revealed that practices important from a public health perspective, such as reporting suspect cases to public health officials or asking for travel history, are not performed widely enough.
One surprising finding was the misconception that the Arizona border region is endemic for dengue virus, whereas only travel-associated cases have been reported to date. Providers possessing this misconception might not recognize the urgency of reporting potentially locally acquired cases to public health officials.
Some results of this study were expected, such as findings that respondents who specialized in infectious diseases or who were aware of the increase in the dengue cases in Sonora would have higher overall scores, as providers more trained or informed will likely know more about the disease. Similarly, the observation that participating DO/MDs performed better than NP/PAs may be related to the more extensive and comprehensive nature of the curriculum. Some observations from this analysis suggest that factors in addition to educational background could influence dengue knowledge in these two groups, as predictors of KAP score were having seen a patient with dengue-compatible symptoms since October 2014 for DO/MDs and practicing in border counties for NP/PAs. These findings may be helpful in tailoring education and training on dengue to different subgroups of health professionals.
Conclusions
Overall, the results from this survey indicate that education for health care providers on dengue should be improved particularly among noninfectious disease providers in general practice who might be the first point of care for dengue patients. Among all topics, findings suggest that additional training on dengue clinical management is needed. The epidemiology of dengue in Arizona (including the difference between locally acquired and travel-associated cases) should also be highlighted, stressing the importance of asking for travel history, as well as notifying the local health department on suspicion of a dengue patient, as required by rule (A.A.C. R9-6-202).
This KAP survey had several limitations. The main limitation is likely the low response rate and the difficulty in calculating it accurately. As a result, the presence of some selection bias is possible as survey respondents often represent those more interested or more knowledgeable about a topic. This decreases the representativeness and the generalizability of our results to all Arizona providers. In addition, survey questions could also have been misinterpreted, with possible impact on the validity and reliability of the information collected; however, we tried to minimize misinterpretation by carefully drafting the questions and piloting the survey with providers before dissemination. Despite these limitations, this work represents one of the first surveys of health care providers in the United States in a region at high risk of dengue emergence and elicited responses from providers with diverse backgrounds and geographic range.
As clinicians tend to be unfamiliar with newly emerging infectious diseases, that this and similar studies found mostly low levels of confidence in treating or diagnosing dengue is not surprising (Tomashek et al. 2014, Adam et al. 2017). However, the potential for fatal outcomes without proper fluid management, the importance of timely reporting of dengue cases to public health officials, and the potential for locally acquired cases in Arizona requiring response underscore the importance of, at a minimum, health care providers being aware of the symptoms of dengue virus infection, knowing which diagnostic tests to select, and alerting public health partners about suspected cases.
Since the administration of this dengue KAP survey, chikungunya and Zika viruses have also rapidly emerged throughout the Americas, raising the additional threat of the spread of these viruses into Arizona Aedes mosquito populations. While this survey was specific for dengue, some of these results are relevant to chikungunya and possibly Zika, although with heightened media and medical attention to Zika, providers may now be more familiar with Zika than dengue. Knowledge of both diseases is critical, as dengue and Zika present as similar acute febrile or rash illnesses, have different clinical management, and can be difficult to diagnostically distinguish by serologic tests. These disease features further highlight the importance of effective strategies for training providers about emerging infectious diseases, such as the use of CDC online continuing education (CDC TRAIN 2017) or similar methods.
Footnotes
Acknowledgments
This work was supported by the CDC Epidemiology and Laboratory Capacity (ELC) for Infectious Diseases cooperative agreement and the Public Health Emergency Preparedness (PHEP) cooperative agreement. Other individuals who contributed to this work are Jefferson Jones, MD, MPH and Lisa Villarroel, MD, MPH.
Author Disclosure Statement
No conflicting financial interests exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.