
Abstract
Introduction:
In Asia, Borrelia garinii, B. afzelii, and B. bavariensis are transmitted by Ixodes persulcatus ticks and clinically present with a wide range of neurological and arthritic symptoms. This report aims to provide details on the geographic distribution of suspected cases of Lyme borreliosis (LB), reported to local Mongolian hospitals between 2007 and 2017.
Methods:
This report examines 150 reported cases of suspected LB from 13 aimags (provinces) in Mongolia from April 2007 to August 2017, including date and location of infection, method of diagnosis (indirect immunofluorescent assay and/or enzyme-linked immunosorbent assay test), frequency of specific symptoms, and case demographics. Information was gathered through collaboration with the National Center of Communicable Disease and the National Center for Zoonotic Diseases.
Results:
Zavkhan and Selenge, located in northern Mongolia, had the highest percentage of reported suspected cases, with 25% and 20%, respectively. Ages ranged from 1 to 78 years, with a mean age of 26 years, however, 37% of individuals were younger than 10. More than twice as many women sought treatment as men, and the distribution of men who sought treatment was skewed toward children and the elderly. Most frequently reported symptoms include fever, rash, headache, and enlarged lymph glands. Furthermore, peak months of tick bite and treatment seeking occurred between April and June.
Conclusions:
Based on these preliminary findings, syndromic surveillance should be expanded across northern Mongolia, with LB considered in differential diagnosis for patients reporting a recent tick bite.
Introduction
Lyme borreliosis (LB), caused by the spirochete Borrelia burgdorferi sensu lato, is the most abundant vector-borne disease in the Northern hemisphere (Higgins 2004). In Asia, Borrelia garinii, B. afzelii, and B. bavariensis are transmitted by the Ixodes persulcatus tick and clinically present with a wide range of neurological and arthritic symptoms (Stanek et al. 2011b, Sabitova et al. 2018). B. garinii, in particular, has caused neuroborreliosis with symptoms, including headache, paralysis, and issues with perception and coordination in Slovenia (Strle et al. 2006). While neighboring countries China and Russia have detected B. garinii in both clinical settings and from native I. persulcatus ticks, information about Borrelia in Mongolia is limited (Ishiguro et al. 2000, Rar et al. 2005). Selenge Aimag had 37 registered cases between 2005 and 2009, but no details regarding those cases were provided (Scholz et al. 2013). While studies from Mongolia have detected B. burgdorferi sensu lato in ticks, to our knowledge, there is only one human study in Mongolia examining LB, which focused on the seroprevalence of LB antibodies in nonclinical samples (Walder et al. 2006, Masuzawa et al. 2014, Sabitova et al. 2018).
This report aims to provide details on the geographic distribution of suspected LB cases reported to the Mongolian National Center for Zoonotic Diseases (NCZD) from April 2007 to August 2017. Additional information presented describes the range of symptoms, date of tick bite, and demographic characteristics of reported cases.
Subjects and Methods
Data were collected retrospectively using medical records from local hospitals in Mongolia between 2007 and 2017, coordinating between the National Center of Communicable Disease and the NCZD. Aimags where cases originated include Arkhangai, Bayankhongor, Bulgan, Darkhan-Uul, Dundgovi, Khentii, Khovd, Khuvsgul, Selenge, Tuv, Ulaanbaatar, Uvurkhangai, and Zavkhan. The following information was collected for each case: age, sex, occupation, aimag and soum (city) of infection, history of tick bite, date of infection, date of onset of clinical symptoms, dates of hospitalization, range of symptoms, and laboratory results used for diagnosis. All patient data were deidentified before analysis, with this study considered “exempt” by George Mason University's Institutional Review Board.
Anti-Borrelia-plus VIsE ELISA (immunoglobulin G [IgG]) and Anti-Borrelia ELISA (immunoglobulin M [IgM]) kits and immunofluorescence assay were used for laboratory diagnosis (Antibody Kit; EUROIMMUN, Germany). A neutralization titer of ≥1.1 was considered positive.
Results
A total of 150 suspected clinical cases of LB originated from 13 different aimags (provinces) in Mongolia (Fig. 1), 78.7% (118/150) of whom recalled experiencing a tick bite before onset of symptoms. Information on cases and symptoms by aimag can be found in Table 1. Both Zavkhan and Selenge aimags, located in northern Mongolia, had the highest number of suspected LB cases, with 25% of all reported cases originating in Zavkhan and 20% in Selenge. The majority of patients (125/150) received indirect immunofluorescent assay (IIFA) testing to check for the presence of IgG and IgM antibodies, with 42 cases testing positive via enzyme-linked immunosorbent assay (ELISA), which became the common form of diagnosis in 2016. All patients received IIFA testing and/or ELISA testing and 35 patients were tested for other tick-borne diseases during differential diagnosis, two of whom tested positive for a Rickettsia coinfection, another emerging tick-borne disease of concern in Mongolia (Boldbaatar et al. 2017).
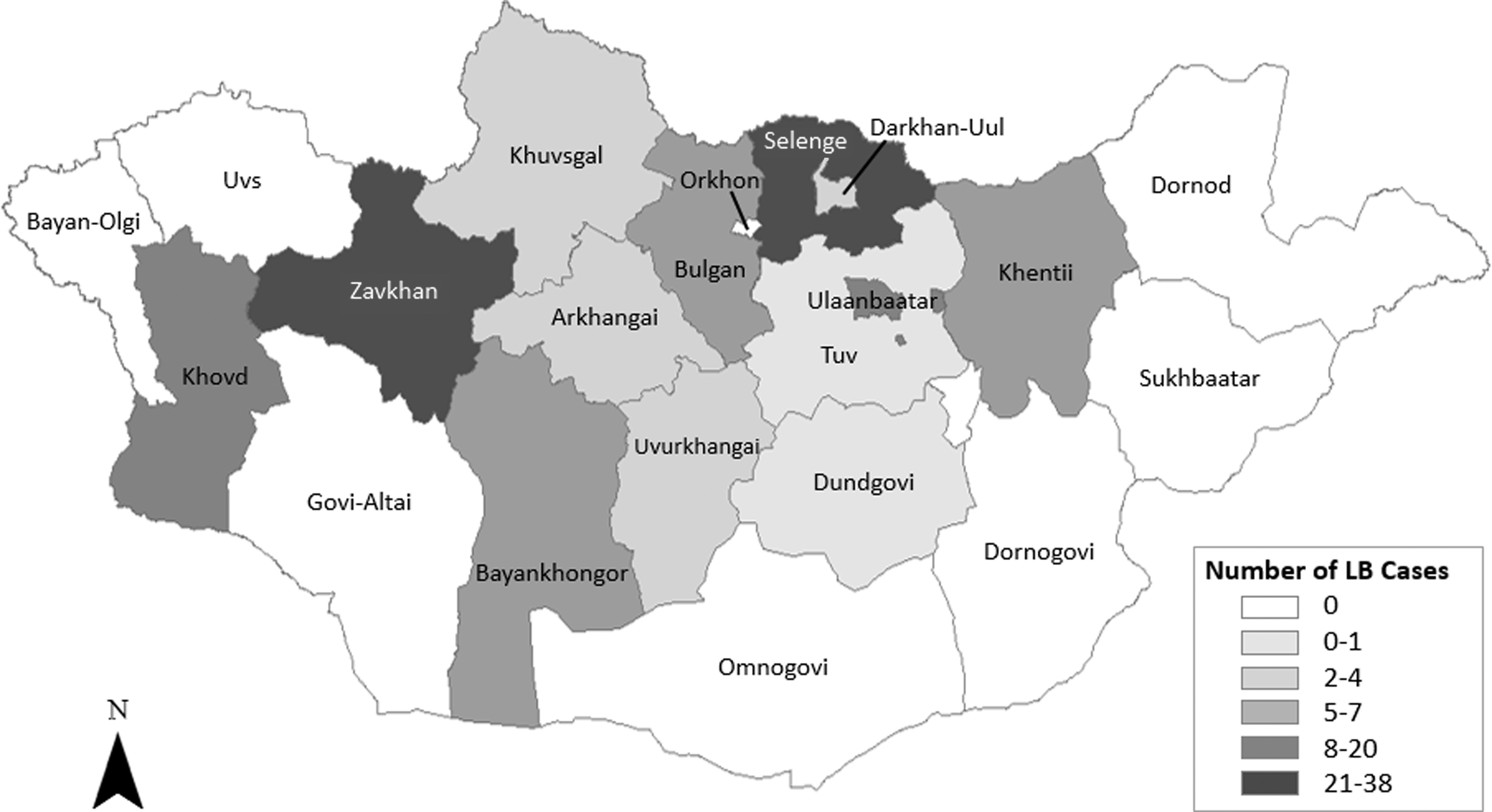
Map of Mongolia depicting suspected Lyme borreliosis cases from individuals reported to local Mongolian hospitals in each aimag from 2007 to 2017 (n = 150 cases).
Summary of Demographic Features and Symptom Distribution by Aimag, from North to South, Among Suspected Lyme Borreliosis Cases Reported to Local Mongolian Hospitals (n = 150 cases, 2007–2017)
Cases reported in major cities.
MM, expanded vessels of the mucous membranes; LG, enlarged/painful lymph glands; SD, standard deviation.
Eighty-five percent of patients (128/150) received their initial diagnosis of LB based cumulatively on history of tick bite in a suspected endemic region, clinical symptoms, and a positive antibody test. Thirteen others lived in endemic areas and were diagnosed through a positive antibody test, and two patients who did not live in endemic areas were diagnosed using laboratory testing. Eight cases occurred within the Gobi region, located in southern Mongolia outside the suspected range for I. persulcatus ticks.
The mean age was 26 years, ranging from 1 to 78 years, with 37% of reported cases in children younger than 10. In addition, more than twice as many women sought treatment as men. Fever, headaches, and localized inflammation at the site of a bite were the most frequently reported symptoms among other less frequently experienced symptoms reported in Table 1. The time span from recall of tick bite to date of hospitalization for clinical symptoms is displayed in Fig. 2. Roughly 70% of cases reported experiencing onset of symptoms within 6 weeks following a tick bite, with the majority of cases reported in May each year.
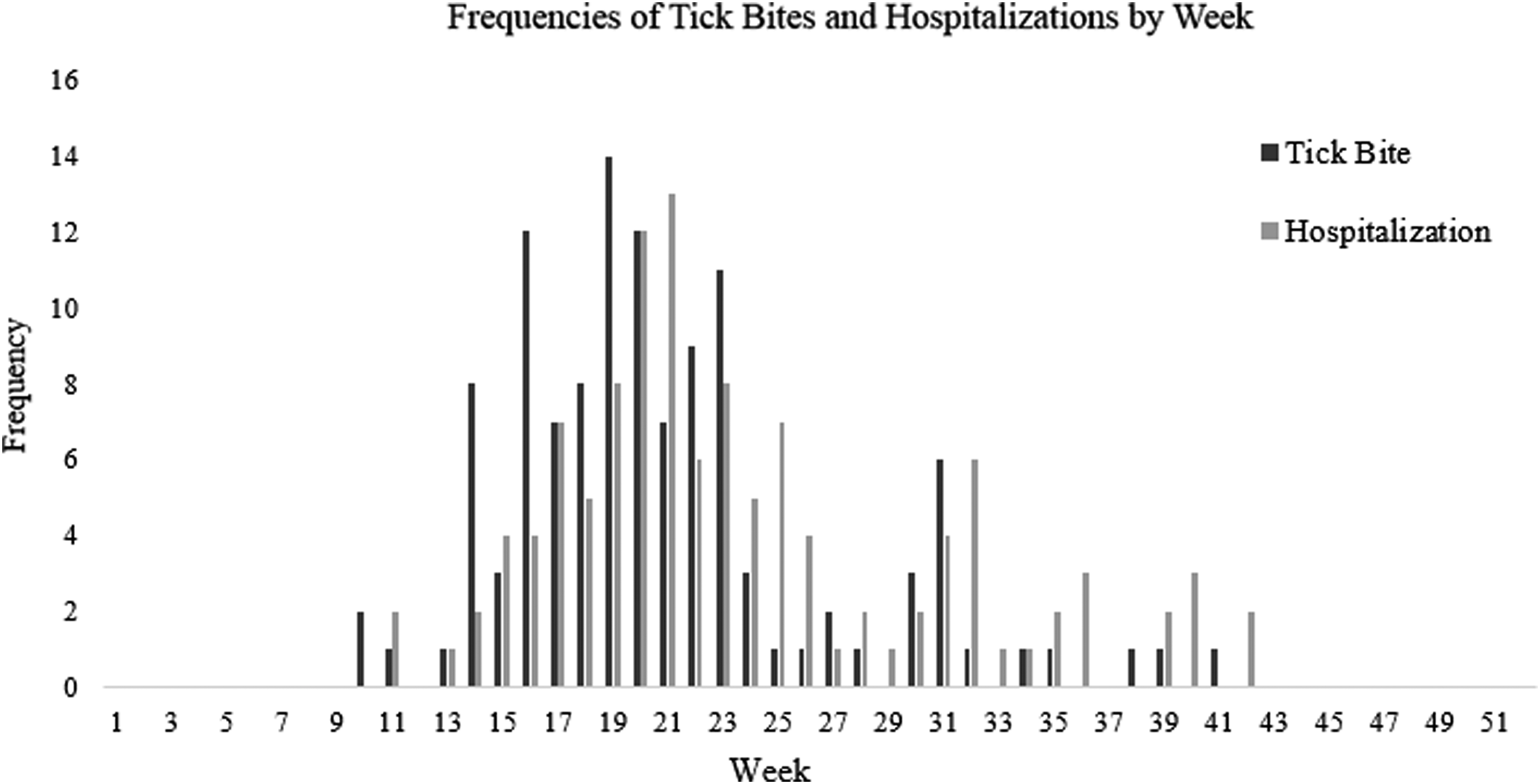
Reported tick bites and hospitalizations by week of 118/150 cases who reported a tick bite and sought treatment in hospital from 2007 to 2017.
Discussion
Selenge has been shown to have the highest detection rates of Borrelia spp. in I. persulcatus ticks and incidence of LB in humans; thus, it is not surprising that a large proportion of cases originated there within the known range and habitat of I. persulcatus ticks (Scholz et al. 2013, Sabitova et al. 2018). The relatively high number of cases (20) reported in Ulaanbaatar, the capital of Mongolia, likely occurred in the surrounding countryside and were reported when individuals sought care on returning to the city.
The distribution of ages in presented cases is consistent with findings, in the United States, that 30% of Lyme diagnoses are made in children (Hildenbrand et al. 2009). It is unknown if these results can be attributed to heightened risk of tick bite in children due to more time spent outdoors or because of increased reporting by parents. Furthermore, two-thirds of reported cases were female, which may represent a discrepancy in health care-seeking behaviors between Mongolian men and women.
Our data indicate that peak LB transmission occurs between weeks 14 and 25, which is from April through June. Patients in this study presented the majority of symptoms between 0 and 49 days after reporting a tick bite, which is in line with previous reports of LB symptoms occurring 4–6 weeks after tick bite (Knudtzen et al. 2017).
Treatment with antibiotics is effective for LB; however, delayed LB treatment results in greater variability in recovery time (Zajkowska et al. 2012). For this reason, it is vital that clinical symptoms of this disease be well-described and that populations most at risk for infection are properly educated, as it is likely this disease is frequently misdiagnosed and underreported in Mongolia. Although serological antibody testing is sufficient for a Lyme arthritis diagnosis, diagnosing Lyme neuroborreliosis requires intrathecal-specific antibody synthesis, which is difficult to conduct in resource-limited rural clinics (Stanek et al. 2011a).
In Lyme endemic areas, working outdoors in any capacity has been shown to increase likelihood of infection 10-fold (Donohoe et al. 2015). It is important to note that nomadic herders, who make up roughly 26% of Mongolia's population, are unlikely to be captured in hospital-based surveillance used in this study (Boldbaatar et al. 2017). Furthermore, given the amount of time Mongolian herders spend outdoors and around livestock, they are likely a group at highest risk of exposure to tick-borne diseases. Future studies that focus on the rate of LB infection and perception of risk in Mongolia are needed to better understand the burden of disease and identify how education and preventative measures for tick-borne diseases can be improved.
As with any retrospective study, this case series was dependent on the accuracy of existing medical records, which are prone to inconsistencies in data reporting and often have missing data fields. In addition, many cases reported neurological symptoms, but did not have an accompanying intrathecal-specific antibody test needed to confirm neuroborreliosis. Finally, this study only includes information from cases reporting to aimag center hospitals and clinics, with no reports of nomadic herders recorded within this data set. Given the severity of symptoms associated with untreated LB, active surveillance is needed within these geographic regions to better estimate the true incidence of LB in Mongolia.
Informed Consent and Patient Details
All patient data were deidentified and shared by the Mongolian Ministry of Health.
Footnotes
Author Disclosure Statement
No competing financial interests exist.