
Abstract
Zika virus (ZIKV) is an arthropod-borne RNA virus (arbovirus), belonging to the Spondweni serogroup. ZIKV was first described in Africa in 1947 and remained sporadic until Micronesia outbreak in 2007, which was followed by outbreaks in the Pacific Islands, Latin America, and the Caribbean. Subsequent to the epidemics, ZIKV revealed its severity as virus was sexually transmissible, and it was associated with serious fetal and neurological complications. ZIKV originated from Africa; however, little is known about the epidemiology of the virus in African populations. Following a recent study in Cameroon that evidenced low ZIKV epidemiology associated with a presumptive (peri-)sylvatic transmission, we performed a seroepidemiological study in Republic of the Congo, neighbor of Cameroon. To accomplish this, 386 serum specimens from volunteer blood donors collected in 2011 from rural and urban areas of Republic of the Congo were tested with ZIKV-specific methodology; primary screening with anti-NS1 ZIKV IgG ELISA followed by confirmation with cytopathic effect (CPE)-based virus neutralization test (VNT). ZIKV seropositivity was determined as low as 1.8%, varying slightly between urban and rural areas (1.7% and 3.6%). These results demonstrate that the majority of the population of Republic of the Congo is immunologically naïve against ZIKV with a presumptive (peri-)sylvatic transmission cycle, which emphasizes the importance of surveillance studies in Africa.
Introduction
A
Despite the undisputable African evolutionary origin of ZIKV and its early identification in Africa ∼70 years ago (Dick et al. 1952), the extent of viral distribution and the herd immunity in African populations still remain largely unknown. However, low ZIKV seropositivity rates have been reported recently in Central Africa (Cameroon) (Gake et al. 2017), (Democratic Republic of the Congo) (Willcox et al. 2018), East Africa (Uganda) (Kayiwa et al. 2018), and West Africa (Nigeria) (Herrera et al. 2017, Mathé et al. 2018), (Senegal) (Herrera et al. 2017). In the Republic of the Congo, one serological survey was reported in 1954, describing 0.4% ZIKV seropositivity in 460 serum samples using a complement fixation test (Pellissier 1954). However, since the complement test has been described as the least sensitive serological methodology for dengue (World Health Organization 2009), and for ZIKV the test was reported to be susceptible to cross reaction with other flaviviruses (Charrel et al. 2016); a definitive conclusion with the results of complement fixation test is not achievable.
Importantly, a recent Cameroonian study suggested a (peri-)sylvatic circulation of ZIKV, in contrast with the urban circulation model reported during recent outbreaks in the Americas, implying a natural cycle including different, (peri-)sylvatic mosquito vectors (Gake et al. 2017).
Here, we present a new ZIKV seroprevalence study performed on healthy volunteer blood donors of the Republic of the Congo.
Serum samples from 386 healthy volunteer blood donors residing in urban (Brazzaville, Pointe-Noire) and rural areas (Ewo, Gamboma, Oyo, Owando) were collected between March and July 2011 (i.e., several years before the virus did spread to the Americas and caused large-scale epidemics) and first used for an Ebola virus study (Moyen et al. 2014). Informed written consent was obtained from each blood donor. The study was approved by the Congolese Research in Health Sciences Ethics Committee (N° 00000065 DGRST/CERSSA). Alike previous studies in the French West Indies (Gallian et al. 2017), Cameroon (Gake et al. 2017), Bolivia (Saba et al. 2018), and Lao PDR (Pastorino et al. 2019), samples were primarily tested with anti-NS1 ZIKV IgG ELISA (EUROIMMUN, Germany). Subsequently, non-negatives were confirmed by cytopathic effect (CPE)-based virus neutralization test (VNT) as described previously (Nurtop et al. 2018).
Among the 386 blood donors, a large majority (92.7%) were living in urban areas (68.4% in Brazzaville; 24.3% in Pointe Noire) and in a modern house (84.7%). They were 18–63 years old, with 181 (46.9%) of them being <30 years old and a median age of 24. The gender ratio (Male/Female) was 3.65. The majority of blood donors were unemployed (26.9%), and the most common occupations were manual labor (20.5%) and studentship (17.6%).
ELISA testing identified 5.7% of non-negatives (including 3.4% of positive [ratio ≥1.1] and 2.3% of equivocal samples [0.8 ≥ ratio <1.1]). After seroneutralization, ZIKV seropositivity rate was 1.8%. It was 1.1% in Brazzaville, 3.2% in Pointe-Noire (altogether 1.7% in urban areas), and 3.6% in rural areas (Fig. 1). The differences between rural and urban areas and between Brazzaville and Pointe-Noire were insignificant given the limited numbers tested. No statistical association between antibodies to ZIKV and gender, age, or occupation was detected.
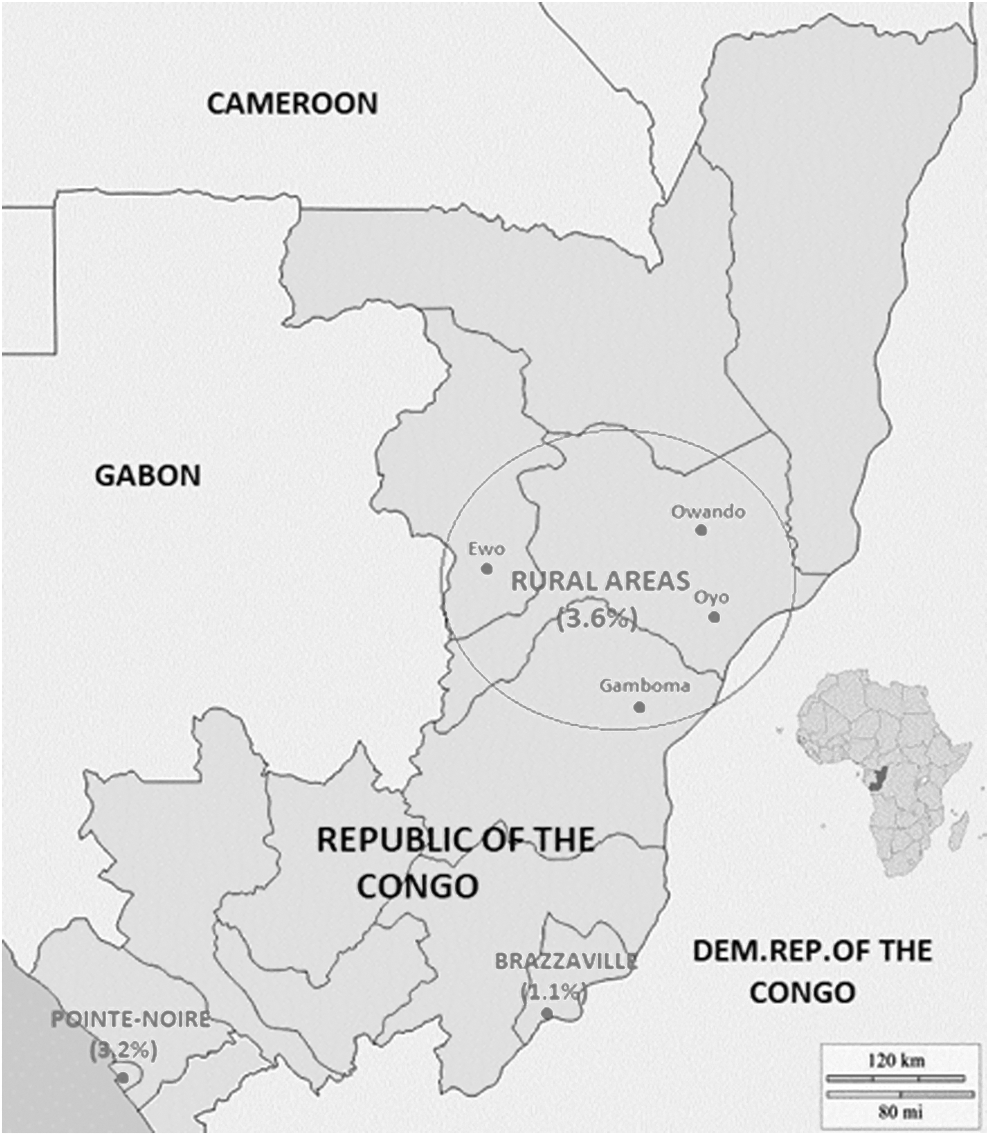
ZIKV seropositivity percentages in two cities and rural areas of Republic of the Congo. ZIKV, Zika virus.
In conclusion, our results evidence that the circulation of ZIKV in the Republic of the Congo is limited, resulting in a low level of specific immunity in the population, as previously observed in the neighboring Cameroon (Gake et al. 2017). Hence, the most probable model of virus circulation still refers to a (peri-)sylvatic natural cycle, as previously proposed in Cameroon (Gake et al. 2017), and not to an urban, dengue-like, cycle relying on transmission by domestic mosquitoes. This suggests that urban Aedes aegypti mosquitoes have not been implicated so far in epidemic transmission of ZIKV in the Republic of the Congo, possibly because their vector competence for (peri-)sylvatic ZIKV strains is limited. This obviously would deserve further experimental investigation.
Considering the low level of herd immunity in the Republic of the Congo, the outstanding question is whether epidemic transmission may occur after either importation of a ZIKV strain adapted to urban mosquitoes or the local emergence of a strain efficiently transmitted by (peri-)domestic mosquitoes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was partially supported by the European Union's Horizon 2020 Research and Innovation Programme under ZIKAlliance grant agreement no. 734548 and the European Virus Archive EVAg; European Union-Horizon 2020 programme under grant agreement no. 653316. We thank the GDRI GRAVIR—Groupement de Recherche sur les Arthropodes Vecteurs en afrIque centRale.