
Abstract
Vaccination against rabies and routine antibody testing of subjects participating in programs for the surveillance and control of rabies in animals is strongly recommended. The scope of this study is to describe the antibody level as measured by a commercial enzyme-linked immunosorbent assay (ELISA) after primary and booster intramuscular vaccination with a purified vero-cell rabies vaccine (PVRV) in high-risk professionals and to determine the influence of an array of factors on antibody level, that is, time elapsed since primary immunization series and booster dose, sex, age, pathologic conditions, high-risk occupation, and peak antibody level after initial scheme and booster dose. A primary series of three doses of PVRV was administered and a commercial ELISA was recommended 14 days postimmunization with continuous repetition at 6 months and yearly intervals for the laboratory personnel and the rest of the professionals, respectively. The protective antibody titer was defined as a minimum of 0.5 equivalent units/mL (EU/mL) (seroconvertion) and a booster dose was applied if the titer was determined nonprotective. The seroconversion rate (SCR) after primary vaccination was 100%, with a geometric mean titer (GMT) of 2.90 EU/mL (interquartile range [IQR]: 1.85–3.45). After booster vaccination due to nonprotective titer, the SCR was 100% and the GMT increased by 678% (95% confidence interval [CI]: 514–887) reaching 4.25 EU/mL (IQR: 4.00–4.60), 2.5 times higher than the GMT elicited by the primary vaccine scheme in the respective recipients. The titer dropped by 1.20% per month (95% CI: 0.52–1.89) regardless of booster administration or any other factor. Women had 51% higher titer compared with men (95% CI: 6–116). High-risk professionals should be verified for adequate antibody titers, but routine administration of a single booster dose of PVRV 1 year after the primary series could be considered; more evidence is needed to support the benefit in terms of immunity and logistics.
Introduction
Rabies is an almost invariably fatal viral disease for most mammals, including humans (Hemachudha et al. 2013). The virus is typically transmitted by the bite of an infected mammal, often a carnivore or a bat, and also via mucous membrane exposure, and, less commonly, aerosol inhalation (Mahadevan et al. 2016). Infective virions are mainly found in the neural tissue of central nervous system (CNS) and saliva and less commonly in organs innervated by sympathetic or parasympathetic fibers, for example, the liver, kidney, and heart (Robertson et al. 2012). Laboratory transmission has also been documented and is a recognized occupational hazard (Sewell 1995). Pre-exposure prophylaxis is recommended for people at continuous, frequent, or increased risk for exposure to rabies virus according to the WHO (2018).
Immunization protects high-risk professionals from unrecognized exposure to the virus, and in case of an exposure event, reduces the recommended regimen to just 2 doses of vaccine (days 0, 3) (Manning et al. 2008, Kessels et al. 2017) eliminating the need to administer immunoglobulin.
After the re-emergence of rabies in Greek fauna in October 2012 (Tsiodras et al. 2013, Tasioudi et al. 2014), a National Programme for Surveillance and Eradication of Rabies in animals (NPSER) was developed and coordinated by the Zoonoses Department of the General Veterinary Directorate and implemented by a network of public sector veterinarians, wildlife officers, game wardens, municipal animal workers and collaborating veterinarians, across the country. The collected samples, mainly red foxes, were examined by the personnel of the National Reference Laboratory for Rabies in animals. Results of animal surveillance are crucial for medical management of persons exposed to animals (Dougas et al. 2019) and for evaluating the implementation of the animal oral rabies vaccination.
Prophylactic vaccination against rabies of the participants in the NPSER was recommended since they were engaged in field sampling activities, laboratory examination of animal specimens, and handling live virus baits for oral vaccination of wildlife. Detailed guidelines for the vaccination schedule and the subsequent serologic tests to ensure an adequate (protective) antibody level were developed by the National Public Health Organization (NPHO) in 2014, based on the World Health Organization (WHO) and U. S. Centers for Disease Control recommendations (Manning et al. 2008, WHO 2013).
The scope of this article is to describe the antibody level as measured by a commercial enzyme-linked immunosorbent assay (ELISA) after primary and booster vaccination in high-risk professionals and to investigate the effect on the serology outcome of a battery of factors, that is, peak antibody level after the primary scheme and the booster dose, length of time following vaccination, age, sex, health status, and the high-risk profession of the participants.
Materials and Methods
The study included professionals, vaccinated from 2013 onward, in compliance with NPHO guidelines, without a history of pre- or postexposure vaccination against rabies before their participation in the NPSER. Additional exclusion criteria for enrollment in the study were recent treatment with corticosteroids, immunosuppressive agents or antimalarial drugs, and a history of infectious diseases or conditions, which may seriously interfere with the development of active immunity (Taylor et al. 1984, Manning et al. 2008, Kopel et al. 2012). However, subjects suffering from chronic diseases, but under medical supervision and clinically healthy, were not prohibited from participation.
The vaccine used was a purified vero-cell rabies vaccine (PVRV) with the inactivated strain Wistar PM-WI 38-1503-3M grown in vero cells with a yield of ≥2.5 I.U./0.5 mL (VACCIN RABIQUE PASTEUR™ and VERORAB™). Vaccines were administered by health professionals in local public health directorates with intramuscular injection into the deltoid muscle. The primary schedule comprised three doses on days 0, 7, and 21 or 28, followed by a blood sample at least 14 days after the last (third) vaccine dose.
The serum samples were obtained from blood samples of the participants after clot formation, with centrifugation for at least 5 min at 4000 g, and were preserved at freezing temperature (≤−18°C) until laboratory examination. A commercial ELISA (PLATELIA™ II, BIORAD™), based on rabies glycoprotein/anti-human immunoglobulin enzyme conjugates, was utilized for determining the anti-rabies neutralizing antibodies in sera. According to the manufacturer, the protective antibody titer was set to a minimum value of 0.5 equivalent units/mL (EU/mL). If the titer was determined protective (≥0.5 EU/mL), blood sampling and titer investigation should be repeated annually for personnel engaged in high-risk activities in the field, for example, wildlife sampling, and every 6 months for laboratory employees working with live rabies virus. If the titer was determined nonprotective (<0.5 EU/mL), the person was advised to cease high-risk tasks until a booster vaccine dose was administered and the serological examination revealed a protective titer. Furthermore, if longer than 1 year for the field high-risk professionals and 6 months for the laboratory personnel had elapsed since the last identification of protective titer without a new titer determination, the participant was not considered protected until a test confirmed an adequate antibody level (Fig. 1).

Algorithm for rabies vaccination and serology testing for high-risk personnel of the National Programme for Surveillance and Eradication of Rabies.
Serology tests were conducted in the Department of Microbiology of the Medical School of the National Kapodistrian University of Athens. On the basis of titer determination, the history, and clinical examination, the recipients were evaluated by collaborating hospital physicians as immunologically fit for high-risk activities in the field.
Information on demographics, dates of primary vaccinations, blood samplings, boosters, as well as on the medical evaluation of the participants regarding immunocompetence and temporary or chronic disorders, was collected through dedicated report forms and retrieved on August 1, 2018 from the vaccinees registry, managed by the NPHO.
The participants were examined for the period after the primary series, for as long they did not receive the booster dose (nonbooster group), and for the period after they received one booster dose due to detection of nonprotective titer (booster group).
The postprimary series response and the postbooster response were defined as the ELISA result to the primary vaccine series and to the booster dose, respectively, measured in a blood sample drawn 14–90 days postvaccination since antibody level peaks during this period (Sabchareon et al. 1999, Cunha et al. 2010, Montaner et al. 2012).
The effect of time (days) postvaccination, booster dose, age, sex, postprimary series response, postbooster response, and the high-risk occupation on the log serum titer were explored using linear mixed-effects models, with random intercepts and random slopes per study participant. Likelihood-ratio testing was used for model comparison, to examine the effect of interactions with time and other covariates. Model coefficients were expressed as percentages (%) of change in the titer. Univariate comparisons were performed with the Mann–Whitney U test, the Fisher exact test, and the Wilcoxon signed-rank test as appropriate.
The R software environment, version 3.5.2, was used for all analyses. The threshold for statistical significance was set to p < 0.05.
Results
Among the 166 study participants, 7 had received the postexposure vaccination regimen (5 of them with immunoglobulin administration), 8 were vaccinated before the release of NPHO guidelines (no serology monitoring was available), while the rest (n = 151) fulfilled the selection criteria and were included in the study (nonbooster group).
The participants were mostly male (62.9%) and had a median age of 45 years (interquartile range [IQR]: 42–50); the majority were veterinarians employed in the local directorates, followed by game wardens (Table 1).
Participants by High-Risk Occupation
National Reference Laboratory for Rabies in animals.
Among the participants, 7% (n = 10) had a history of hypothyroidism, 1.3% (n = 2) of hyperthyroidism, 4% (n = 6) of dyslipidemia, 1.3% (n = 2) of diabetes mellitus, 0.7% (n = 1) of psoriasis, and 0.7% (n = 1) of chronic hepatitis B.
The seroconversion rate (SCR) postprimary series vaccination was 100% for samples drawn 14–90 days after the third dose (n = 31) with titer equal or above 0.5 EU/mL. The respective geometric mean titer (GMT) was 2.9 EU/mL (IQR: 1.85–3.45).
Among 144 participants who were tested >90 days (median = 520, IQR: 350–898) after the completion of the primary series vaccination and before any booster shot, nonprotective titer was registered in 38 (26.4%), in a median period of 351 days (IQR: 155–476). All participants identified with nonprotective titer received a booster dose (booster group) and presented 100% SCR when sampled 14–90 days postvaccination (n = 32). In total, 312 and 73 serology tests were conducted with participants sampled a median of three times (IQR: 2–3) and a median of two times (IQR: 1–2) before and after booster, respectively (Fig. 2).
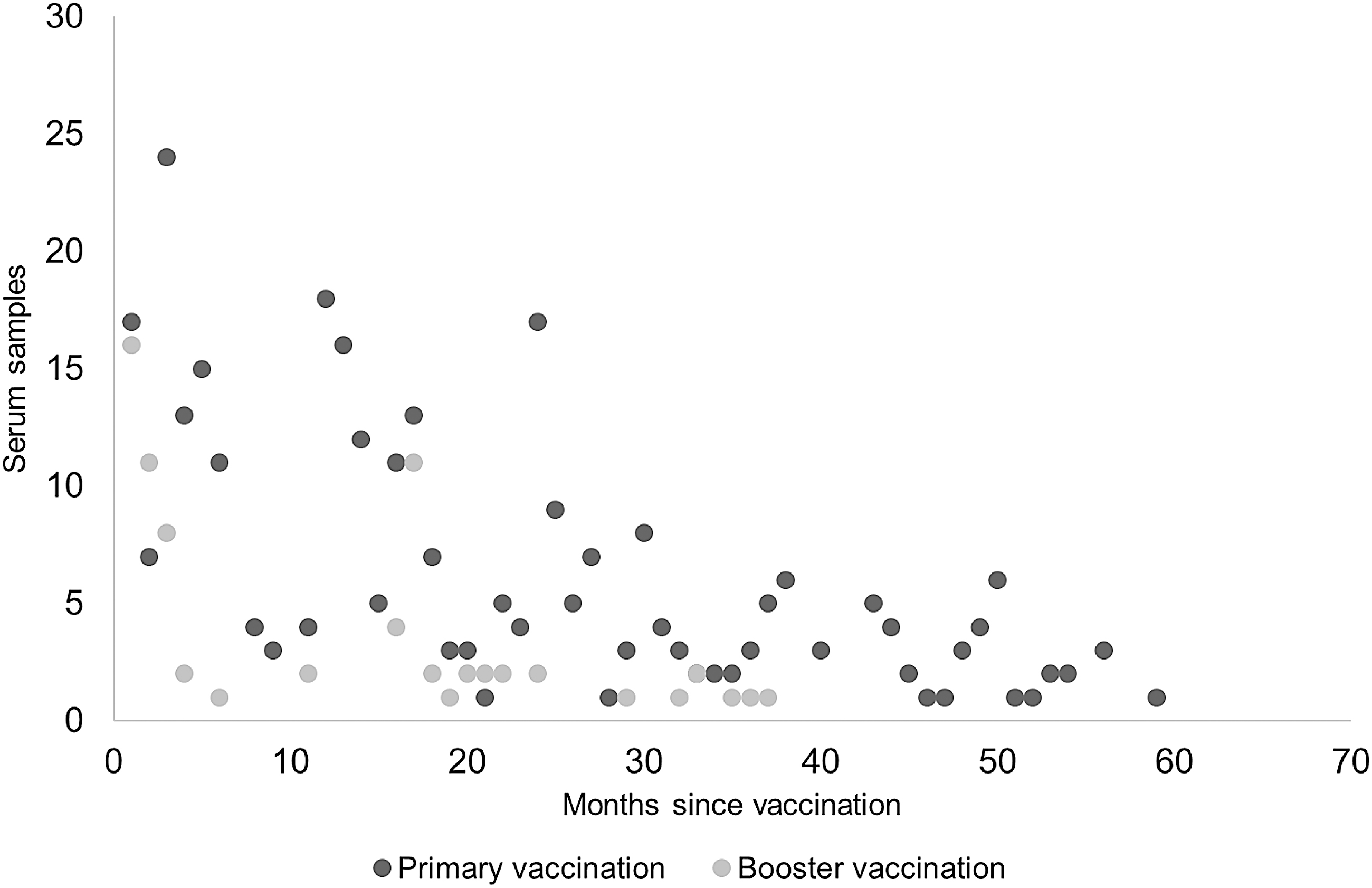
Scatterplot of serum samples examined per month since primary and booster vaccination.
According to the linear mixed-effects model, a booster dose resulted in a significant rise of the titer (p < 0.001, Mann–Whitney test) (Table 2).
Geometric Mean Titer in Equivalent Units/mL, Before and After the Booster Dose (n = 32)
14–90 days postbooster administration.
CI, confidence interval; GMT, geometric mean titer; IQR, interquartile range.
The 14–90-day postbooster titer (GMT = 4.70 EU/mL, IQR: 4.28–5.30) was also significantly higher than the postprimary series response (GMT = 1.85 EU/mL, IQR: 1.30–3.30) (p = 0.03, Wilcoxon signed-rank test), for the participants for whom the information was available (n = 6).
According to the linear mixed-effects model, the titer dropped by 1.20% per 30 days (95% confidence interval [CI]: 0.52–1.89) postvaccination, and this was similar between men and women (p-value for interaction = 0.27) and between the nonbooster and booster groups (p-value for interaction = 0.26) (Fig. 3).

GMT and IQR in nonbooster and booster groups of vaccinees by semester of sampling after vaccination—dotted line represents the threshold of 0.5 EU/mL. EU/mL, equivalent units/mL; GMT, geometric mean titer; IQR, interquartile range.
Women had a 51% higher titer than men (95% CI: 6–116) in all ELISA results, in both booster and nonbooster groups.
Adding underlying pathologic conditions, high-risk occupation, age, postprimary series response, and postbooster response as fixed effects in the base model did not improve the model fit (all p-values for interaction >0.05).
Discussion
Postimmunization periodical rabies antibody titer examination is essential to ensure maximum protection of people involved in high-risk activities for exposure to Lyssavirus spp.
The particular ELISA (PLATELIA II, Bio-Rad) is a widely utilized method for determining the postvaccination rabies antibody level since it is simple, safe, and rapid, and with comparable sensitivity and specificity with the reference method (rapid fluorescent focus inhibition test—RFFIT) (Feyssaguet et al. 2007, Welch et al. 2009). Specifically, Feyssaguet et al. (2007) reported a sensitivity of 98.6% and specificity of 99.4% of this particular ELISA when compared with RFFIT, with high linearity and metric concordance between cutoffs and titers obtained by both assays. On the contrary, PVRV due to exceptional immunogenicity and reduced cost is a frequently used type of vaccine for the prevention of rabies in high-risk groups (Kitala et al. 1990).
However, while there is a considerable body of studies on the immunologic impact of rabies vaccines, to our knowledge, there is a scarcity of reports investigating the influence of an array of factors to the serology outcome, as measured by a commercial ELISA after pre-exposure intramuscular PVRV; moreover, others (Lim et al. 2010) recognize an insufficiency of rabies vaccination studies regarding high-risk professionals.
This study affirmed that a recommended schedule of a three-dose primary vaccination series in high-risk professionals using an intramuscularly administered PVRV provided appropriate protection as evidenced by a commonly used commercial ELISA (≥0.5 EU/mL). In addition, the postbooster antibody response was significantly higher than the postprimary vaccination response in the respective individuals. Among the examined variables, sex and length of time following vaccination were found to influence the immune response; female employees seroconverted better than males; and the length of time after the primary vaccination or the booster shot was negatively associated with the serology outcome and statistically described. The rate of titer drop, on the contrary, neither differed between nonbooster and booster groups, males and females, nor was associated with any other examined factor.
Almost 15% of the participants in this study had a history of a chronic underlying condition with possible immune-modulating attributes (Lösche et al. 1992, Muldoon et al. 1997, Geerlings 1999, De Vito et al. 2011). According to our results, these conditions were not associated with any effect in the titer outcome in accordance with previous reports (Banga et al. 2014). However, the low number of subjects might not be sufficient for statistical outcomes.
A similar response to vaccination, using PVRV or chromatographically PVRV, and the immunological benefit of a booster dose of PVRV have been documented in other studies (Lang et al. 1998, Jones et al. 2001, Strady et al. 2009, Medeiros et al. 2016). In a similar study in terms of materials and recipients (Lim et al. 2010), describing the immune response of at-risk professionals using the same type of vaccine and serology method, 39.4% of vaccinees exhibited titers ≤0.5 EU/mL 1 year postprimary series immunization. However, quantified comparisons with other reports were not feasible since materials and methods did not concur with those used in our study; in several reports, we identified a tendency of higher numerical values (IU/mL) and for longer periods when sera were examined with RFFIT (Strady et al. 2009, Banga et al. 2014, Medeiros et al. 2016). According to Welch et al. (2009), the commercially available ELISA tends to provide more specific results, but tends to undercalculate the outcome (EU/mL) in comparison with RFFIT.
The sex-based differentiation of immune response was in accordance with similar observations for rabies (Mansfield et al. 2016, Medeiros et al. 2016) or other viral vaccines (Klein et al. 2010).
Variable adherence to the recommended immunization schedule and multiple tests per person resulted in increased variance of the time elapsed from vaccination to blood sampling. To our knowledge, while in similar studies a declining titer over time has been frequently demonstrated, a quantification of the association of time since vaccination with the titer drop rate has not been previously described and would be useful for public health purposes when devising strategies for pre-exposure prophylaxis.
Based on our findings that the antibody level declined over time at a rate unaffected from booster, the earliest nonprotective titers appeared in a median period of 1 year, and a booster dose of PVRV had a high impact on the antibody titer, we suggest, as indicated by others (Morris et al. 2007, Strady et al. 2009), that a booster could be considered for routine administration 1-year postprimary vaccination, in people engaged in high-risk activities, regardless of the simultaneous occurrence of protective titer. However, more evidence is needed to support this practice as a suggested modality in vaccination schedules relying on titer determination by serology tests.
Our study had several limitations. First the number of participants was relatively low. Second the limited duration of the study (nine semesters for nonbooster and six semesters for booster group) might compromise the generalization of our findings. Third, the narrow age span of the participants might have introduced a bias since younger individuals have been previously reported to develop higher antibody titers and to maintain these for longer periods (Giefing-Kröll et al. 2015). In addition, data related to the batch of the ELISA, the type (VACCINE RABIQUE PASTEUR™ or VERORAB™), and LOT number of vaccines, as well as the preservation conditions or the administration technique, were not obtained. The potency of rabies vaccines may reportedly vary from manufacturer to manufacturer or from batch to batch (Cunha et al. 2010), but at least in two studies failed to reveal an association with the immune response (Taylor et al. 1984, Strady et al. 2009). Moreover, the immunocompetence status of the participants may have a huge impact on the antibody response (Tantawichien et al. 2001, Kopel et al. 2012). We accommodated this by deriving a careful clinical evaluation by the appointed physicians; however, neither complete medical records nor specialized laboratory examinations for diagnosing immunodeficiency were available. According to Horowitz et al. (2010), the assessment of natural killer cell activation and T cell interleukin-2 secretion should be included in the evaluation of immune responses induced by vaccination. Further understanding of the cellular immune response to rabies vaccination is required. Nutritional status, obesity, genetic background, or environmental factors, which reportedly may influence the postvaccination immune response, were not addressed in this study (Wilson et al. 1995, Moore et al. 2006, Banga et al. 2014, Castrucci 2017).
Conclusions
All high-risk individuals for exposure to rabies were vaccinated with the primary scheme of PVRV and developed protective antibody titer, as proven by a commercial ELISA. Decline to nonprotective titer (<0.5 EU/mL) was observed in a median time of 1 year in 26.4% of participants in whom a single booster dose elicited a GMT 2.5 times higher than the postprimary series one. Only sex of the participants had an effect on the antibody titer, whereas the rate of titer drop was quantified at 1.20% per month and remained unaffected from booster or any examined factor. Our results suggest that even in vaccination protocols relying on determination of antibody level, a booster dose would prolong protective antibody titers and could be considered for routine administration 1 year postprimary series in people engaged in high-risk activities; more evidence is needed to support the benefit in terms of immunity and logistic convenience.
Footnotes
Acknowledgments
We thank Dr. Olga Mangana, Dr. Aristarchos Seimenis, Dr. Marilina Korou, Dr. Konstantia Tasioudi, and Thomas Alexandropoulos, General Director of Veterinary Services, for their participation in organizing the framework of vaccinations and serological tests. We are deeply grateful to the physicians and nurses in all the collaborating hospitals for their relentless efforts in evaluating the vaccinees and to the health professionals of the health directorates for their pivotal role in carrying out the vaccinations and locally coordinating the vaccinees and the stakeholders.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
We are grateful to Mrs. Aikaterini Liona and Mrs. Eleni Vrachnou; without their exceptional work and administrative support, the coordination of vaccinations and serology examinations of such a great number of people in various locations would not be possible.