
Abstract
Background:
Mosquito-borne diseases in the Republic of Korea have a unique epidemiology due to the rapid improvement in hygiene and economic status, occurrence of four distinct seasons, and separation from North Korea owing to the political situation. Therefore, we aimed to analyze and review the epidemiology of mosquito-borne diseases in Korea.
Methods:
The incidence and geographical distribution of malaria, Japanese encephalitis (JE), Zika virus infection, chikungunya fever, and dengue fever were investigated using data from the Korean Centers for Disease Control and Prevention. Lymphatic filariasis and West Nile fever, which have rarely been reported in Korea, have also been discussed in this literature review.
Results and Conclusions:
Malaria disappeared from Korea in 1979, but since its re-emergence in 1993 there has been constant occurrence with local transmission. In Korea, vivax malaria is the only prevailing disease, and the clinically problematic chloroquine resistance has not been reported. The incidence of JE has greatly reduced since the introduction of the national vaccination program for children in 1985. However, the incidence of JE has been increasing recently, especially in adults >40 years of age. Filariasis, which was previously endemic to Jeju Island and the southern coastal area, has not been reported since 2002. Although there are numerous imported cases with increasing overseas travel, there are still no indigenous cases of Zika, chikungunya, and dengue fever reported in Korea. The West Nile virus was isolated from migratory birds, but there has been only one imported human case to date.
Introduction
Various infectious diseases transmitted by mosquitoes occur worldwide, and several million people die annually from mosquito-borne diseases (WHO 2019). The risk of mosquito-borne diseases is further magnified due to climate change (Reiter 2001). Furthermore, rapid globalization and emerging infectious diseases have also increased the need for updated information regarding infectious diseases prevalent in individual countries.
The Republic of Korea (Korea) has a unique epidemiology of mosquito-borne diseases due to the following reasons: (i) Korea has four distinct seasons, unlike the tropical areas. (ii) South Korea's rapid economic growth since the 1980s has led to an improvement in hygiene/sanitation and implementation of national vaccination programs. (iii) Movement of civilian across land is impossible in Korea, but the movement of mosquitoes is possible in the area bordering North Korea, and this has led to the re-emergence of malaria in Korea (Chai 1999). (iv) Frequent movement of people between Korea and Southeast Asia has resulted in relatively large numbers of imported dengue fever and chikungunya-infected cases (Park and Lee 2012, Cha et al. 2013). Although there have been some good studies on mosquito-borne diseases in Korea, they were only written in the Korean language (Yeom 2017, Lee 2017). Therefore, the use of this information by foreign scholars and clinicians for research and medical treatment was limited. Consequently, this study aimed to analyze and review the epidemiology of mosquito-borne diseases in Korea.
Methods
For the epidemiology of mosquito-borne diseases, we analyzed the annual incidence, geographical distribution, and monthly distribution of malaria, Japanese encephalitis (JE), dengue fever, chikungunya fever, and Zika virus infection in Korea by utilizing the Infectious Diseases Surveillance Yearbook released by the Korean Centers for Disease Control and Prevention (KCDC 2019b). Since West Nile fever occurs rarely and lymphatic filariasis has already been eliminated in Korea, they have been described through a nonsystematic literature review.
Results and Discussion
Common mosquitoes in Korea
Korea is a part of Far East Asia and geographically located between the latitudes 33–38°N and longitudes 124–132°E. Four seasons are evident, and mosquito-borne infections are prevalent mainly from April to October (Yeom 2017). Three sides of the Korean peninsula are surrounded by the sea, and the demilitarized zone (DMZ) is in the middle of it, making it impossible for civilians to traverse the boundary. Hence, imported and domestic infections can be clearly distinguished. Korea is predominantly mountainous in the northeast and characterized by agricultural areas in the southwest. Half of the Korean population live in Seoul Metropolitan City and Gyeonggi-do (province).
There are 9 genera and 56 species of mosquitoes in Korea (Lee 2017). Eight Anopheline species had been recorded in Korea (Foley et al. 2014). Among these Anopheles (An.) sinensis is the most common species and the major vector species of malaria. Also, Anopheles pullus, Anopheles kleini, Anopheles belenrae, Anopheles lesteri, and Anopheles sineroides had been incriminated as malaria vectors in Korea (Foley et al. 2014). The remaining two species (Anopheles koreicus and Anopheles lindesayi japonicus) have not yet been identified as vectors of Plasmodium vivax in Korea (Foley et al. 2014). The larvae of Anopheles are most common in rural and mountainous areas because they spawn in relatively clean water sources, such as rice fields, irrigation water, swamps, and puddles. Anopheles spp. peak in summer (July to August) and disappear in the middle of October until the end of April due to hibernation.
Aedes (Ae.) vexans is another common mosquito in Korea (Kim et al. 2010). Aedes vexans nipponi is a subspecies of Ae. vexans and mainly distributed in northeast Asia. Similar to the Anopheles larvae, their larvae are found in relatively clean water, such as rice fields, water ponds after floods, wildlife, and urban parks (Becker et al. 2003). Although the Chaoyang virus has been isolated from Ae. vexans (Lee et al. 2013), there is no evidence that it can transmit any other human pathogen in Korea. Aedes albopictus is known to be an important potential vector of dengue virus, Zika virus, and chikungunya virus. Although Ae. albopictus are found in the southern part of Korea, recent studies have shown no evidence of dengue, Zika, and chikungunya viruses in Korea (Yang Sung-Chan 2017). Unlike Culex or Anopheles, Aedes mosquitoes hibernate as eggs (Mitchell 1995). Therefore, establishing stable transmission of Aedes mosquito-borne diseases is difficult during winter in Korea, except for the possibility of vertical transmission through eggs (Ferreira-de-Lima and Lima-Camara 2018).
Culex (Cx.) tritaeniorhynchus is another common mosquito species in Korea distributed throughout the country, but it is more prevalent in the southern region of Korea during summer (Yu Hye-mi 2015). The larvae live mainly in rural areas in rice fields, irrigation water, and swamps. Cx. tritaeniorhynchus is a major vector of the JE virus in Korea; therefore, the mosquito is a principal surveillance target. The Culex pipiens complex, unlike Cx. tritaeniorhynchus, scatter in urban wastewater and reservoirs, and are active in winter. There is no evidence that the Cx. pipiens complex transmits the West Nile virus in Korea although the JE virus has been isolated from Cx. pipiens (Kim et al. 2015). Seasonal fluctuations and population sizes markedly differ by location and year, mostly according to the annual temperature and precipitation (Foley et al. 2014). The characteristics of the common mosquitoes are shown in Table 1. The guidelines of the Centers for Disease Control for Controlling the mosquito population are described in Supplementary 1.
Main Mosquito Species in South Korea
Malaria
Malaria is a mosquito-borne disease generally characterized by chills, rigors, and fever (Bennett et al. 2014). The first case in the Korean peninsula, which is almost certainly considered malaria, was recorded in the Goryeo dynasty period (10th to 14th century) and has subsequently been noted continuously (Kim 2015). In the late 1880s, many foreigners who came to Korea developed malaria, and the first scientific report was published in 1913 (Bahk et al. 2018). Of the five Plasmodium species causing infections in humans, only P. vivax is prevalent in Korea (Feighner et al. 1998). In the 1930s, Plasmodium malariae was reported in Seosan, but it disappeared soon afterward. Plasmodium falciparum had also been spreading among drug addicts in Seoul for a short period but then disappeared (Kim 2015). The incidence of malaria in the Korean peninsula was first investigated in 1928, and 2394 deaths were reported among 140,426 patients with malaria.
During the Korean War, foreign veterans in Korea were found to have a high incidence of vivax malaria marked by a long latency period (Hale and Halpenny 1953). In 1959, the national malaria control program was implemented in Korea with the support of the World Health Organization (WHO) (Bahk et al. 2018). One of the major efforts undertaken since then is the strengthening of surveillance. In 1960, 212 patients were diagnosed with malaria following an active case-detection drive conducted in 18,697 patients, whereas 13,929 (30.7%) patients were diagnosed with malaria as a result of passive surveillance performed on 45,395 febrile patients. Unlike now, Gyeongsangbuk-do was the highest endemic region in the 1960s. With the strengthening of surveillance and mosquito control, the incidence of malaria decreased, and Korea declared the eradication of malaria in 1979 (WHO 2016). However, Anopheles remained a major mosquito species in the country, posing a risk for malarial resurgence in Korea. In 1980–1992, there were only some independent cases of imported malaria, with no reports of domestic outbreaks. However, in July 1993, a soldier in the DMZ was diagnosed with vivax malaria (Kim et al. 2009). In the following year, malaria recurred in 21 patients in Korea, and the number of patients gradually increased to ∼4000 by the year 2000 (Chai 1999) (Fig. 1 and Table 2).
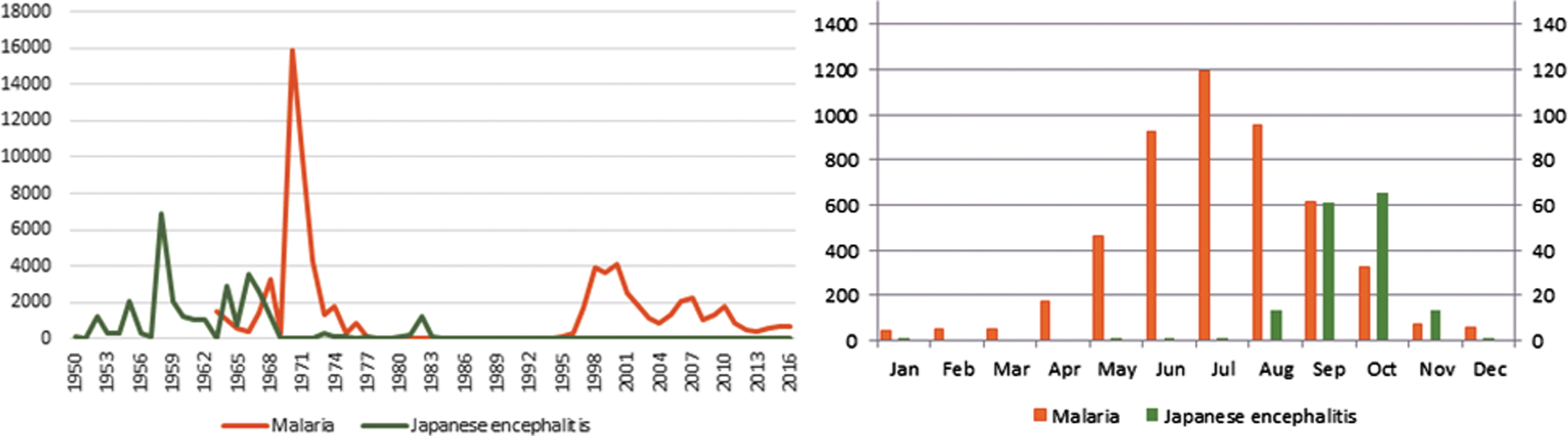
Annual incidence and monthly distribution of malaria and Japanese encephalitis cases in South Korea. The incidence of malaria slightly decreased in the 2000s after its resurgence in 1993. The incidence of Japanese encephalitis has been increasing gradually, but no major outbreak has been noted since 1982. Malaria usually occurs from April to November and also in winter due to long latency. Japanese encephalitis usually occurs from August to November. Color images are available online.
Annual Reported Cases of Mosquito-Borne Diseases in South Korea (2000–2018)
Chikungunya and Zika have been included in the surveillance since 2011 and 2015, respectively.
Although the reason behind this re-emergence is unclear, many specialists suggest the possibility of an inflow from North Korea (Kim et al. 2009, Ree 2000). Considering that most patients in the early period of re-emergence resided within the DMZ or within a few kilometers and that An. sinensis can fly up to 12 km, malaria may have presumably originated in the DMZ or North Korea. However, there is no obvious evidence to prove this theory. Since 1997, large-scale chemoprophylaxis was administered to the Korean army for early eradication of malaria (Im et al. 2018), but local transmission of the disease in civilians continued to increase. Over time, the proportion of civilians with malaria increased, and the disease covered an increasingly large area, spreading beyond 10 km of the DMZ. Following a peak of incidence in 2000, the number of patients decreased due to various preventive policies and early diagnosis. Nevertheless, elimination was not achieved, and 400–600 malaria cases were reported annually in the 2010s. The endemic areas of malaria include the neighboring areas of North Korea (Fig. 2). Recently, the endemic areas in Korea have shifted to the west, presumably due to the development of a new city and change in endemicity in North Korea. The distributions of malaria cases by age and sex are shown in Fig. 3.
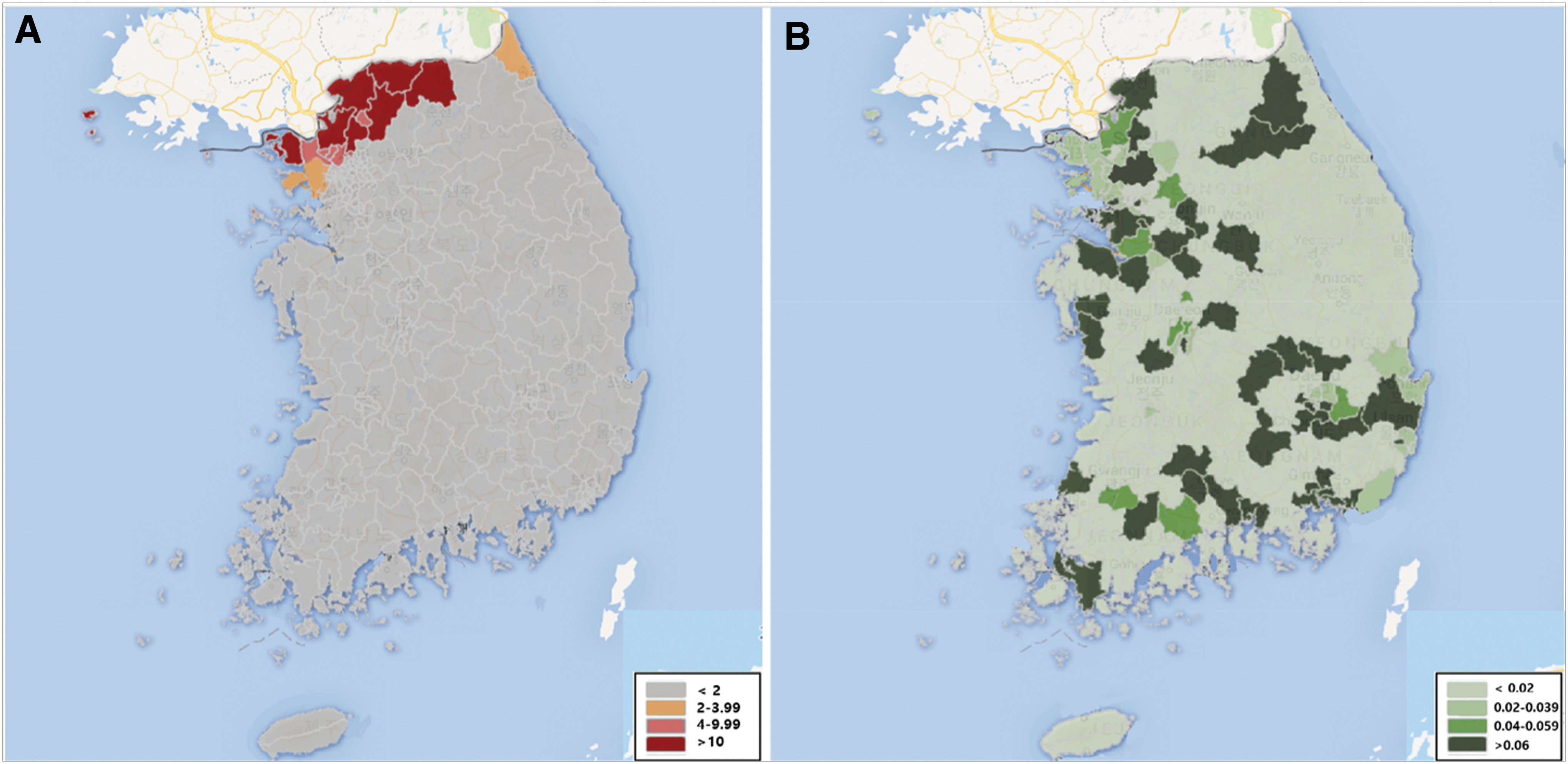
Geographical distribution of vivax malaria and Japanese encephalitis during 2011–2018. The endemicity of malaria and Japanese encephalitis in South Korea (rate for 100,000 persons).
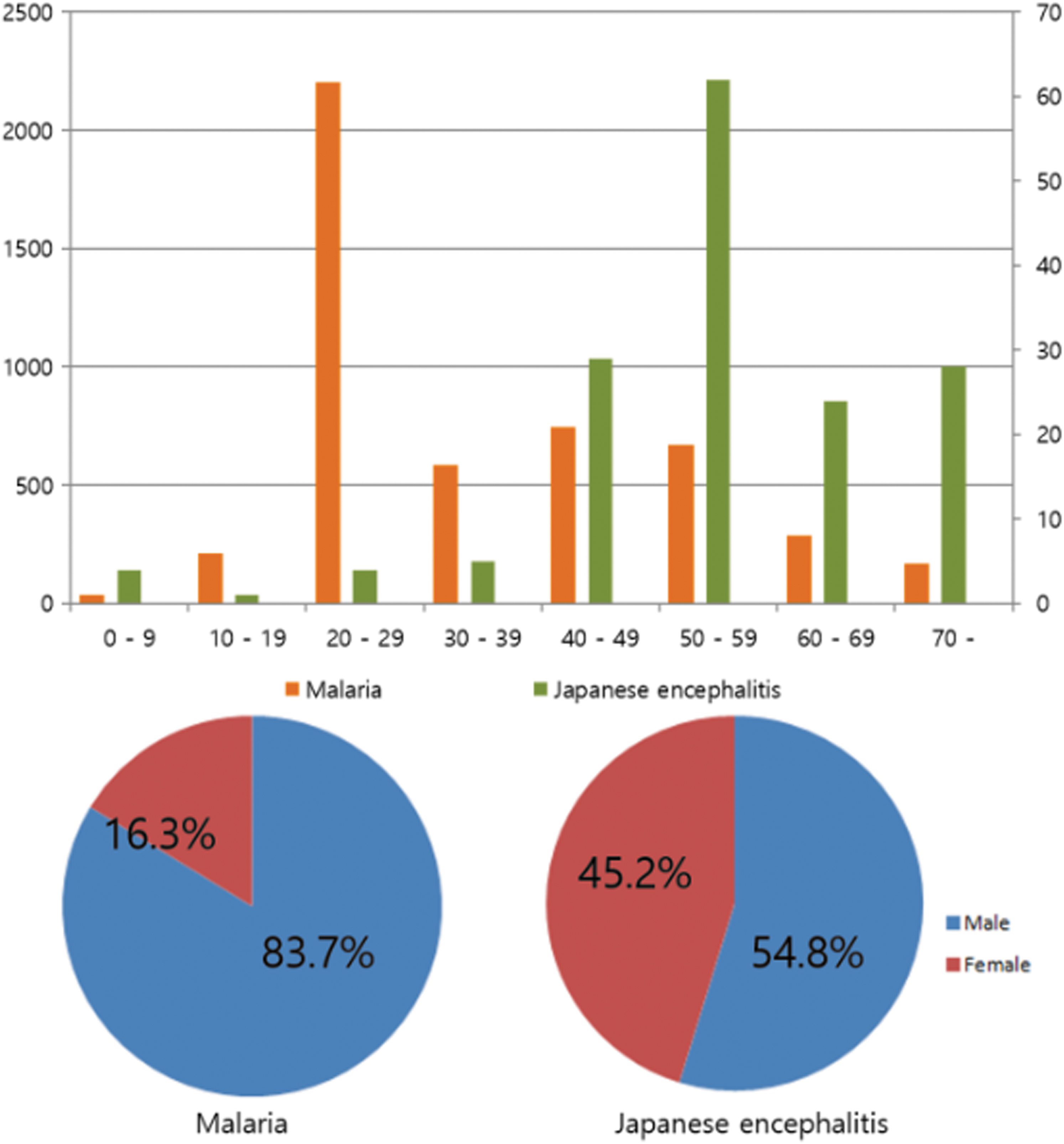
Sex and age distribution of malaria and Japanese encephalitis during 2011–2018. Malaria is prevalent in the below 50-year age group (especially 20s) due to military service and outdoor activity. Japanese encephalitis is more prevalent in the above 40-year age group. With regard to sex, malaria is more prevalent in men due to military service. Japanese encephalitis shows a relatively even prevalence in both sexes. Color images are available online.
To understand the epidemiology of malaria in Korea, it is necessary to understand the situation in North Korea. According to a WHO report, malaria in North Korea re-emerged in 1998 (WHO 2009). However, considering that there were 296,540 malaria cases in 2001, it was assumed that the malarial outbreak in North Korea occurred before 1998. With the help of the WHO, North Korea started its malaria control program in 1999 and continued its efforts until 2001. With mass primaquine chemoprophylaxis, the malaria cases reduced from 296,540 in 2001 to 9353 in 2006 in North Korea. Until recently, ∼10,000–20,000 patients are known to have been reported annually in North Korea, although it is difficult to determine the actual situation there. The endemic areas in North Korea are known to extend from Hwanghae-do to Gangwon-do covering entire North Korea, except for Gaema plateau (WHO 2009).
Mosquitoes causing malaria in Korea are typically found from April to November (Park et al. 2009). However, vivax malaria can develop during the nonendemic period (December–March) after a long latency, when the hypnozoites emerge from their dormant state in the liver (Ko and Choi 2018). Specifically, 60–70% of patients experience a long latency (Kim et al. 2009). Factors affecting the long latency are still unclear, but temperature, time of infection, and number of sporozoites are speculated to play important roles. A study has also suggested that genotype of PvMSP-1 may affect the long latency (Goo et al. 2015).
Vivax malaria is known to be nonsevere, but a previous study has suggested that Korean individuals could be severely affected partially due to low immunity resulting from prior exposure to malaria (Im et al. 2017). However, despite the frequent cases of severe malaria, the mortality rate has been extremely low. The relatively high medical accessibility offered by the National Health Insurance Service in Korea is thought to contribute to the low mortality rates in the country. In Korea, all vivax malaria cases are clinically sensitive to chloroquine and a case of treatment failure due to chloroquine resistance has not yet been reported (Lee et al. 2009). Primaquine treatment is essential for preventing relapse in patients who had vivax malaria (Galappaththy et al. 2013). Since Korean individuals have an extremely low prevalence of glucose-6-phosphate dehydrogenase deficiency, it is rarely a problem associated with the use of primaquine in Korea (Goo et al. 2014).
When compared with the 1970s, eradication of malaria has not been attained despite improvement in diagnosis and mosquito control. Among the various underlying reasons, we believe that the influence of North Korea is obvious, but related studies have not been conducted effectively. Cooperation with North Korea is highly essential for malaria control, management, and research in the Korean peninsula.
Japanese encephalitis
JE is a mosquito-borne infectious disease, which occurs primarily in the Asia Pacific region. It is predominantly caused by Cx. tritaeniorhynchus and leads to neurological complications. In Korea, summer encephalitis has been recorded since the early 20th century. In 1946, Sabin et al. identified the JE virus in a Japanese soldier (Sabin et al. 1947) who was stationed in Korea (Sohn 2000). During the 1950s and 1960s, there were ∼1000–3000 patients annually. To control the mosquitoes, the government performed herbicide work, sewage disinfection, and disinfection around the houses. Dichloro-diphenyl-trichloroethane, which is no longer used, was used for these disinfections. During 1950–1960, the incidence of JE was 100–300 cases/100,000 population per year (Fig. 1). Since 1971, JE vaccination has been administered to children in Busan and Jeollanam-do. In the 1980s, the number of patients with JE decreased dramatically; the vaccination of pigs and intensive insecticidal treatment of pig cages played important roles in this reduction. To effectively prevent JE, the government has been conducting a survey of the density of mosquitoes, investigating the seroconversion rate in vaccinated pigs, and isolating JE viruses from mosquitoes since 1984 (May to October). However, after a small outbreak of JE in 1982, the government recognized that management of vectors and intermediate hosts alone cannot prevent an epidemic completely (Sohn 2000). Consequently, in 1984, the government adopted a national pediatric vaccination program for children between 3 and 15 years of age. Subsequently, the JE vaccine coverage increased significantly from 5% in 1980 to 87% in 1984. Since 2000, the age of children receiving the JE vaccination has been changed to 12–23 months. After the introduction of the vaccination program, the incidence of JE decreased to 0.02/100,000 population in the 2000s (Sohn 2000). However, since 2010, the incidence of JE has been rising (Table 2). Majority of these patients are ≥40 years of age and were born before the implementation of the national JE vaccination program (Jung et al. 2015). JE usually develops between April to November, and the geographical distribution is shown in Fig. 2.
Cx. tritaeniorhynchus (major vector for the transmission of JE in Korea) is distributed in the southern region. The incidence of JE per 100 million individuals between 1955 and 1966 was 18.5 in Jeollabuk-do, 12.5 in Busan, 8.9 in Jeollanam-do, and 5.3 in Gyeongsangnam-do. However, recently, the incidence of JE has been higher in large cities like Seoul. The reason for this discrepancy is unclear, although it is possible that mosquito species other than Cx. tritaeniorhynchus are involved in the transmission (Kim et al. 2015, Shin 2014). Wild animals (birds and wild boar) affect JE virus amplification (Yang et al. 2012, Bae et al. 2018), and the high medical accessibility in urban areas can also cause this discordance. Considering the high incidence of JE in the southwestern area in the previous years (Lee and Hong 2005), southwestern residents >50 years of age may have higher protective antibody titers than those living in Seoul. While this difference in immunity may also affect the regional incidence, there is no evidence to support this theory.
The disease burden of JE is perhaps underestimated. The larger number of cases of JE in urban areas compared with those in rural areas suggests that there may have been differences in access to laboratory tests depending on the region. Furthermore, JE may have an atypical presentation in vaccinated individuals that can be overlooked, and thus misinterpreted as low incidence. Therefore, the disease burden of JE needs to be re-evaluated in Korea. Moreover, it is important to study the change in immunogenicity 40–50 years after vaccination and decide whether vaccine supplementation is necessary for adults >50 years of age.
In Korea, the national JE vaccination program consists of three doses of immunization (the primary two doses are administered 1–4 weeks apart and a booster dose after 1 year) with two additional doses (after 3 and 6 years) (KCDC 2017). Reducing the number of additional doses and extending the vaccination to adults have been discussed, but no clear conclusions have been drawn. The genotype shifting of the JE virus also needs to be studied. The JE virus has recently been replaced by genotype I (Yun et al. 2010). The relatively limited diversity of the JE virus has ensured effective vaccination (Tsarev et al. 2000, Kurane and Takasaki 2000), but recent pig experiments have shown a low cross-neutralizing effect on genotype I (Fan et al. 2013). Generally, a genotype III-derived vaccine is considered to be capable of providing protection against genotype I, but the long-term defense capability needs to be verified (Nah et al. 2015). There is little research on the efficacy of the genotype III-derived vaccine against genotype V, which has not been reported to cause human infection in Korea. However, recent reports on genotype V (in Culex orientalis and Cx. pipiens) suggest close monitoring of this genotype (Kim et al. 2015).
Lymphatic filariasis
Lymphatic filariasis is mostly asymptomatic in the acute phase, but some patients present with edema, thickening of the skin, and pain in the arms and legs. In 1927, microfilariasis was scientifically identified in Korean individuals (Yun 1927). In 1943, Korean lymphatic filariasis was found to be caused by the parasite Brugia malayi, not Wuchereria bancrofti (Senoo 1943). In the 1950s, lymphatic filariasis spread widely throughout Korea, except in Gyeonggi-do and Gyeongsangnam-do. It was particularly prevalent in Jeju-do, coastal regions of Jeollanam-do, and inland areas of Gyeongsangbuk-do. Ochlerotatus togoi, the major arthropod vector of lymphatic filariasis in Korea, lives in beaches that are mainly composed of rocks, especially in the saline rock pools in the beaches. Lymphatic filariasis was endemic mainly in Jeju Island and the southwestern coastal area of Jeolla-do. In Gyeongsangbuk-do, An. sinensis was the main vector of lymphatic filariasis. Jeju Island was the region with the highest prevalence of this disease, and massive chemotherapy with diethylcarbamazine was administered here between 1968 and 1973. In the inland area of Gyeongsangbuk-do, selective mass treatment was conducted in 1970. Although mass chemotherapy was effective, it was accompanied by the problem of poor compliance due to adverse drug reactions. This problem was overcome by gradually increasing the daily dose over time. In 1986–1992, diethylcarbamazine chemoprophylaxis was administered in several islands of Jeollanam-do, including the Heuksan Island, due to the relatively high prevalence rate of 11.2% (2159 individuals) in the area. As a result of mass chemotherapy and economic development, the prevalence of lymphatic filariasis has decreased rapidly (Cheun et al. 2009). Since the last two reported cases of lymphatic filariasis in Jeolla-do in 2002, there have been no further cases. The Korean Government and WHO declared Korea as a filariasis-free area in March 2008 (Cheun et al. 2009).
Although there have been no cases of lymphatic filariasis, mosquitoes that predominantly transmit lymphatic filariasis still exist in Korea, and seroprevalence studies or active surveillance for lymphatic filariasis have rarely been performed. Regular national surveillance is necessary to prevent future cases of lymphatic filariasis.
Imported mosquito-borne diseases
Dengue fever, chikungunya fever, and Zika virus infection are relatively common imported mosquito-borne diseases in Korea.
Dengue virus is classified as a flavivirus and causes dengue fever in the tropics of Asia, the South Pacific, Africa, and America. Dengue fever has a latent period of 3–14 days and causes severe headache, muscular pain, and arthralgia. Most patients present a benign course, but death can occur in cases of severe shock or bleeding tendency (Bennett et al. 2014). Aedes aegypti, the major vector of dengue fever, is not found in Korea. While Ae. albopictus, which is regarded as a potential vector for dengue fever, is present in Korea, it has not been yet identified to carry the dengue virus in the country. Nevertheless, there has been a steady rise in the imported dengue infection cases associated with increasing travel to Southeast Asia (Table 2). Considering the numerous imported cases, autologous transmission of dengue virus is possible in Korea, similar to that observed in France and Japan. However, since Aedes spp. cannot hibernate as adults in winter, it is somewhat difficult to transmit in Korea. Nevertheless, attention should be paid to the possibility of climate warming or vertical transmission through eggs. In July 2019, two dengue viruses were detected in two Cx. bitaeniorhynchus mosquitoes in Yeongjong Island (near Incheon International Airport). The serotype DENV-2 was identified and is believed to have come from Thailand. However, it is necessary to carefully monitor the cases (KCDC 2019a).
Chikungunya fever (family Togaviridae, genus Alphavirus) can infect primates, birds, cattle, and rodents. Chikungunya fever has a latency of ∼2–12 days, and after a high fever of ∼40°C, there is onset of severe muscle aches, headache, and joint pain. Although it is difficult to differentiate between dengue fever and chikungunya fever exclusively on the basis of clinical symptoms, chikungunya fever can have a longer duration (up to 1 year), lower bleeding tendency, and more frequently, symmetrical involvement of the small- and medium-sized joints than dengue fever (Bennett et al. 2014). Ae. aegypti is known as the main vector, but it does not exist in Korea. Another vector (Ae. albopictus) is present in Korea, but the virus has not yet been detected in the mosquitoes in Korea. All cases of chikungunya fever identified in Korea were imported cases and the number of patients is gradually increasing with growing travel to Southeast Asia (Table 2).
The Zika virus belongs to the genus Flaviviridae and infection is characterized by a mild headache, rash, fever, malaise, conjunctivitis, and arthralgia. Recent evidence has revealed that it also causes microcephaly in the fetuses of infected mothers, arousing increasing interest in Zika virus infection (Plourde and Bloch 2016). Zika virus is mainly transmitted by Ae. aegypti. Zika virus has also been detected in Anopheles coustani, Mansonia uniformis, and Culex perfuscus, but it is difficult to identify these as obvious vectors of Zika virus (Epelboin et al. 2017). Although transmission by Ae. albopictus (one of the common mosquitoes in Korea) caused an outbreak in 2007 in Gabon (Africa), Zika virus has not yet been isolated from Ae. albopictus in Korea. Stable transmission through Ae. albopictus is difficult due to the four distinct seasons, but attention must be paid to the possibility of Culex species acting as a potential vector in light of climate warming in Korea. All patients with Zika virus infection were found to be imported cases. The annual incidence is shown in Table 2.
West Nile virus, classified as a flavivirus, can cause a sudden onset of fever, headache, myalgia, digestive symptoms, lymphadenopathy, and skin rash after 1–2 weeks of incubation. Depending on the area of involvement, neurological symptoms may be observed, such as optic neuritis, cranial nerve abnormalities, neuromyelitis optica, myelitis, and convulsions (Bennett et al. 2014). West Nile fever is geographically prevalent in the Americas, Africa, and South Asia and geographically separated from the JE virus distribution, but in some regions, the distribution overlaps. Cx. pipiens and Ae. vexans are considered the main vectors, and the virus can spread rapidly because these mosquito species are commonly found in urban areas. In a Korean study, West Nile virus was isolated from 3/75 pigeons captured from Paju, Mungyeong, and Busan (Kim et al. 2016). Moreover, 0.3% of 1500 migratory birds were positive for the West Nile virus antibody (Yeh et al. 2011). Despite the abovementioned evidence, there has been only one imported human case (Hwang et al. 2015), and there have been no indigenous cases.
Conclusion
Malaria and JE have re-emerged in Korea. However, Korea has been filariasis free since 2008. Meanwhile, the number of patients with Zika, dengue, and chikungunya virus infections is increasing because of the increasing number of travelers to Southeast Asia, but no indigenous evidence supports these data. Various infectious diseases are increasing because of the global climate change since the last 10 years. The rapid worldwide rise in human and physical exchanges is spreading infectious diseases between countries, and therefore, the management of mosquito-borne infectious diseases is emphasized. To achieve this, measures such as domestic distribution of mosquitoes, density, investigation of pathogen infection rate, and research on ecology and control, should be reinforced. Additionally, more comprehensive management and additional ecological studies and analyses are required.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
This work was supported by a research grant from Inha University Hospital.
Supplementary Material
Supplementary 1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.