
Abstract
Objective:
This review describes the current scenario of a priority group of emerging infectious diseases (EIDs) listed by World Health Organization (WHO), and their main determinants and drivers for the emergence/spread of the diseases. The gaps and strategies developed by India to meet the WHO guidelines on the effective control of epidemic-prone diseases and outbreaks are also presented in the review.
Methods:
Epidemiologic information of EIDs, namely Crimean–Congo hemorrhagic fever (CCHF), Ebola and Marburg viruses (EboV and MarV), Zika virus (ZIKAV), Rift Valley fever (RVF), Middle East respiratory syndrome, severe acute respiratory syndrome (SARS), Nipah and Hendra virus (NiV and HeV), and Lassa fever virus (LASV), was drawn from international and national electronic databases to assess the situation. A brief view on the novel coronavirus disease 2019 (COVID-19) in India is also included.
Results:
There are no reports for human infection of EboV, MarV, RVF, and LASV in India. CCHF, SARS, ZIKAV, and NiV have been involved in outbreaks in eight states of India, while COVID-19 is currently reported from majority of states. India has deeply strengthened its surveillance and response system of outbreaks and epidemic-prone diseases.
Conclusions:
Despite its enormous improvements made in the anticipation of such threats, still more efforts are needed in sensitization of populations as well as hospital management in the context to EIDs, as addressed in the review. Furthermore, there is still a need for more research and development activities to efficiently control EIDs.
Introduction
Emerging infectious diseases (EIDs) are diseases that are newly recognized, newly introduced, or newly evolved, or that have recently and rapidly changed in incidence or expanded their geographic, host, or vector range (WHO/FAO/OIE 2004). They also include diseases that have affected a given region in the past, declined over time, or were controlled, but again resurfaced in growing numbers (WHO 2014). The recent outbreaks of Zika virus (ZIKAV) and Ebola virus (EboV) in different regions remind us that the world is still largely unprepared to fight promptly and efficiently with these EIDs (Noorbakhsh et al. 2019).
For the highly burdening infectious diseases such as malaria or human immunodeficiency virus infection, we have clearly defined and efficient diagnosis, treatment, and prevention strategies (WHO 2018), whereas the diagnosis and control-related scenario is much more complicated for EIDs. In general, the control strategies of EIDs are either absent or insufficient, thereby increasing their likelihood as a major public health concern when they occur in any area (Mehand et al. 2018). The other common characteristics of EIDs include their high morbidity, unpredictable aspect, explosive potential for increase in infection and death cases, and important economic consequences (Bloom et al. 2017).
A study revealed that 60.3% of EIDs infecting humans between 1940 and 2004 were zoonotic in nature (i.e., transmitted from animals to humans) with a great role of wildlife, and one in five was transmitted by invertebrate vectors such as mosquitoes, ticks, and midges (Jones et al. 2008). Reports on some EIDs such as Crimean–Congo hemorrhagic fever virus (CCHFV), a tick-borne disease, identified the cave-dwelling African bats as additional vectors of pathogen causing CCHFV (Müller et al. 2016). Besides, a large fraction of EIDs have a viral and bacterial origin, and unfortunately many of these EIDs are also neglected diseases, meaning little is dedicated to their control due to lack of funding and innovation (Mackey et al. 2014).
The main contributors for appearance of EIDs consist in human population growth, changes in the environment, climate change, and globalization (Bloom et al. 2017). Given the high deleterious potential of EIDs on human development and the urgent need for their efficient control, a broad group of experts on behalf of the World Health Organization (WHO) proposed in 2016—a Research and Development (R&D) blueprint for action to prevent epidemics (WHO 2016). This WHO R&D blueprint aims at reducing the time interval between the declaration of a disease as public health emergency and the implementation of control strategies that can save lives and avoid health disaster (WHO 2016, Mehand et al. 2018).
A WHO-endorsed expert committee updated the list of current and future priority emerging diseases based on a set of seven criteria (Fig. 1) (Mehand et al. 2018). These priority diseases include CCHFV, EboV, Marburg virus (MarV), ZIKAV, Rift Valley fever (RVF), Middle East respiratory syndrome (MERS) and severe acute respiratory syndrome (SARS), Nipah and Hendra diseases, and Lassa fever (Mehand et al. 2018). This list of infectious priorities has been recently updated again with the addition of the novel coronavirus disease 2019 (COVID-19) that currently hit the world (WHO 2020b).
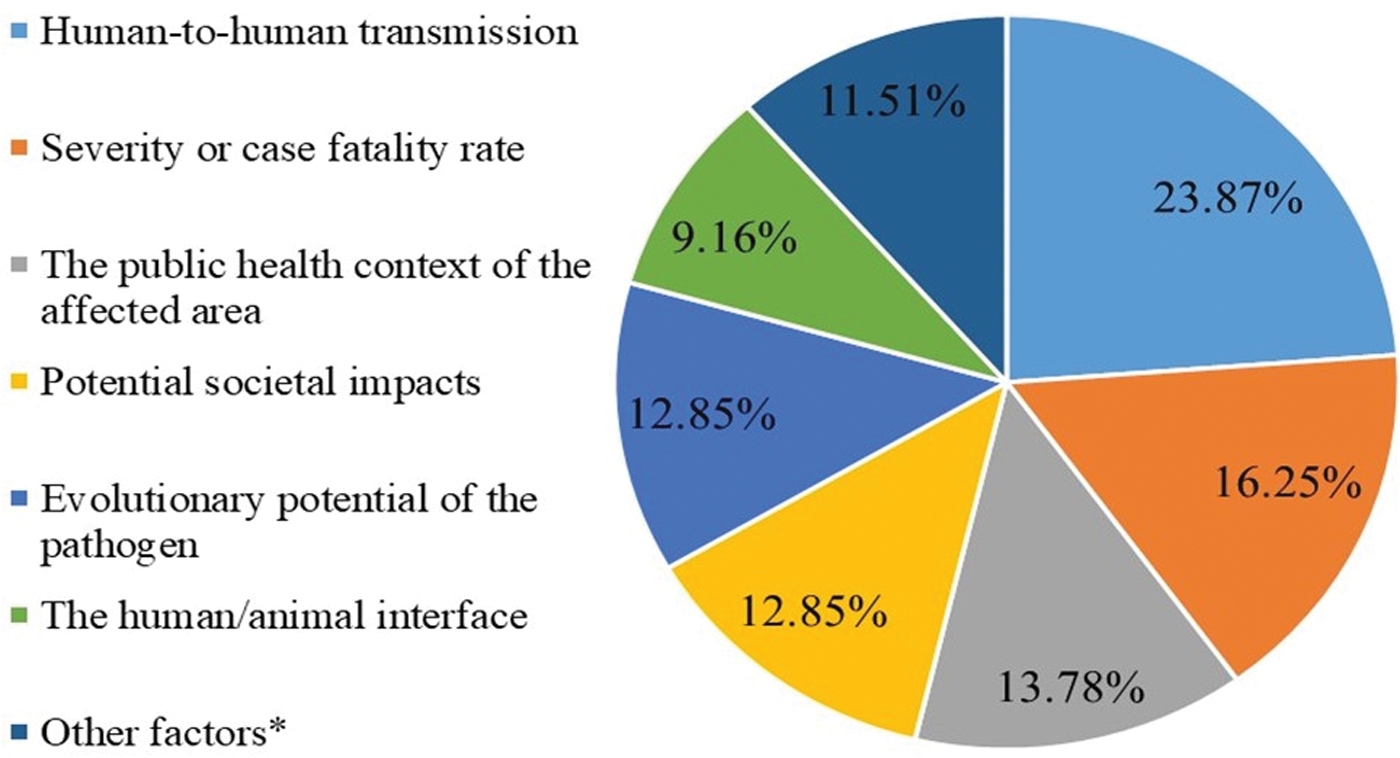
Prioritization criteria and weighing used to define the priority list of diseases described in the WHO R&D blueprint [Adapted from Mehand et al. (2018)]. *The factors include: pathogen's geographic range, shared epidemiological and/or genotypic characteristics with pathogens that pose an epidemic threat, the absence of robust protective immunity, a high risk of occupational exposure, or connections with biological weapon programs. WHO R&D, World Health Organization Research and Development. Color images are available online.
In this review, we present the current scenario and the main findings of studies having addressed these diseases in India, a subcontinent country highly at risk for the emergence and spread of zoonotic diseases and EIDs (Jones et al. 2008, Allen et al. 2017). We also discuss on the surveillance and response health system implemented by the Government of India (GOI) to face such outbreaks and epidemic-prone diseases.
Methodology
Data on WHO-prioritized EIDs were collected from international and national diverse sources, including (1) PubMed, (2) Google scholar, (3) the WHO, (4) Open Data Government Platform India (
Results
Basics and current scenario of R&D WHO blueprint EIDs in India
Crimean–Congo hemorrhagic fever
This infectious disease is transmitted to humans through bites of ticks infected with single-stranded RNA (ssRNA) virus (CCHFV) of the Bunyaviridae family in the Nairovirus genus, which is the deadliest genus in this family (Kuhn et al. 2016). The ticks responsible for the transmission of CCHFV belong to the genus Hyalomma, including species such as Hyalomma marginatum marginatum, Hyalomma detritum, and Hyalomma anatolicumanatolicum (Shayan et al. 2015). The large geographical distribution of CCHFV is strongly related to that of ticks (Charrel et al. 2004).
Although seroepidemiological studies that outlined the possible circulation of the CCHFV in India were existing, the first laboratory-confirmed CCHFV infection cases in India were reported in January 2011 during an outbreak at the Ahmedabad district, Gujarat State, Western India (Figs. 2 and 3) (Mishra et al. 2011, Patel et al. 2011). In the two studies, the index cases were 25- and 32-year-old housewives, respectively, a fraction of other cases were caring hospital staff consisting of medical doctors and nurses, and the fatality rates were high (Mishra et al. 2011, Patel et al. 2011). Another study conducted, in Ahmedabad as well, by a group of Indian scientists of the National Institute of Virology (NIV) reported the presence of IgM antibodies specific to CCHFV in blood samples of human and domestic animals (buffalo, goats, and sheep) (Mourya et al. 2012).
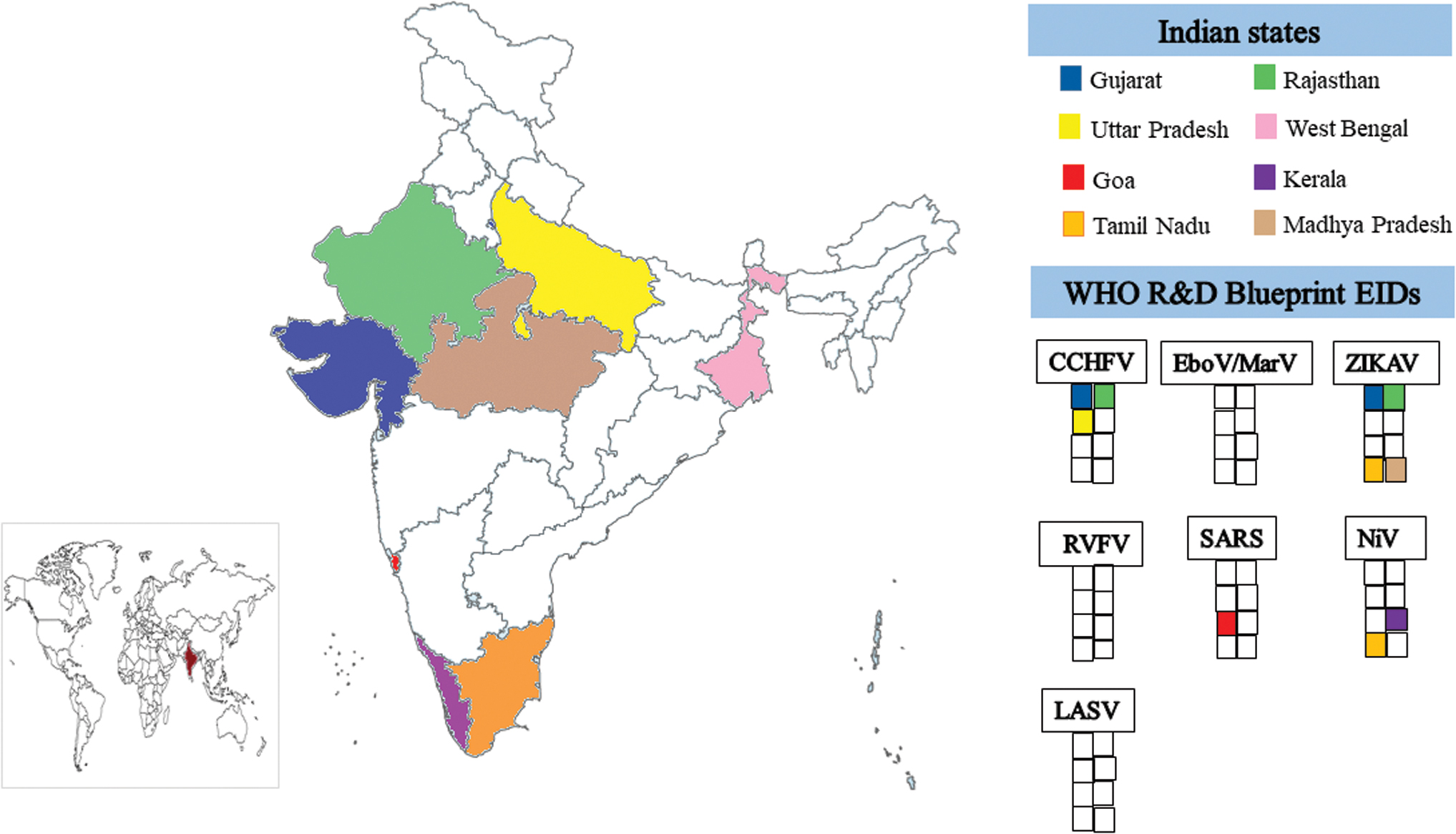
Geographical distribution of reviewed EIDs in different Indian states. The map was generated using ArcGIS version 10.5 for Desktop (ESRI). Each Indian state was attributed a color. Blank square means the absence of a given EID in India, and a colorful square means the presence of a given EID in the Indian state. CCHFV, Crimean–Congo hemorrhagic fever virus; EboV, Ebola virus; EID, emerging infectious disease; LASV, Lassa virus; MarV, Marburg virus; NiV, Nipah virus; RVFV, Rift Valley fever virus; SARS, severe acute respiratory syndrome; ZIKAV, Zika virus. Color images are available online.

Chronological succession of some outbreaks or alerts of reviewed EIDs in India. COV1D19, coronavirus disease 2019. Color images are available online.
The same research team has recently found a seropositivity rate of 0.5% based on the detection of anti-CCHFV IgG antibodies in 4978 human serum samples collected between 2015 and 2017 in the Gujarat State (Mourya et al. 2019). In addition, the risk for CCHFV seropositivity was two- and seven times higher in males and in persons in contact, or a neighbor, with a CCHFV case, respectively (Mourya et al. 2019). From June to July 2013, Yadav et al. (2014) detected the CCFHV in Karyana, a village in Amreli district (Gujarat State), as well as a fatality case in village Undra (Patan district), and the presence of anti-CCHFV IgG antibodies in domestic animals and Hyalomma ticks. This study thereby demonstrated the propagation of CCHFV to other districts in the Gujarat State.
Two further studies have laboratory confirmed the circulation of CCHFV in 4 and 21 blood samples from the Rajasthan State (Roy et al. 2016, Mourya et al. 2017), while another study reported the presence of the virus in the Uttar Pradesh and Rajasthan States (Singh et al. 2016). Three studies addressed the genotypic diversity of CCHFV isolates from the Gujarat, Uttar Pradesh, and Rajasthan States (Mourya et al. 2012, Yadav et al. 2013, Singh et al. 2016). Two of these studies identified CCHFV isolates as belonging to the Asia 2 group and genetically close to the strain Tajikistan TADJ/HU8966 (Mourya et al. 2012, Yadav et al. 2013), unlike the remaining study that reported CCHFV strains belonging to the Asia 1 group (Singh et al. 2016). Recently, Sahay et al. (2020a) analyzed pooled Hyalomma ticks collected in the districts of Jaisalmer, Jodhpur, and Sirohi of the Rajasthan State where a CCHFV outbreak occurred between August and November 2019, and found a similarity of virus genotypes with those observed in Africa.
EboV and MarV diseases
EboV was first discovered in 1976 near the Ebola River in what is now known as the Democratic Republic of the Congo (DRC) (WHO 1978). Marburg disease is caused by MarV, a negative ssRNA virus primarily recognized in 1967 during hemorrhagic fever outbreaks in laboratories in Marburg and Frankfort (Germany), and Belgrade (Serbia) (Slenczka and Klenk 2007). The animal reservoirs of both these viruses are thought to be cave-dwelling African fruit bats, but unlike EboV, the African bats Rousettus aegyptiacus have been definitely identified as the reservoir of MarV (Claire et al. 2017).
The natural circulation of EboV and MarV has not been officially recognized in India, despite the fact that on November 18, 2014, an Ebola infection case was identified in a facility at Delhi's Indira Gandhi International airport, in a 26-year-old man returning from Liberia (Bagcchi 2014). The Liberian authorities declared him Ebola-free as he had been treated and his blood was tested negative for the infection. Although the blood samples of this man also tested negative in India, his semen samples tested positive for the EboV infection, following which he was quarantined until negative results (Bagcchi 2014).
ZIKAV disease
The virus responsible for the disease is a Flavivirus; dengue, chikungunya, yellow fever, Japanese encephalitis, and West Nile viruses are transmitted to humans by the bite of infected female Aedes mosquitoes (Kuhn et al. 2010). The other reported routes of transmission for ZIKAV are sexual, intrauterine, laboratory exposure, perinatal, and blood transfusion (Baud et al. 2017). Based on genetic analyses, the different identified ZIKAV strains are regrouped into two lineages consisting of the ancestral African and contemporary Asian lineages (Li et al. 2018).
The first three cases of ZIKAV infection in India were reported in January/February 2017 in two pregnant women (34 and 22 years old) and one 64-year-old male in Ahmedabad, Gujarat State (Figs. 2 and 3). A phylogenetic analysis on the isolate from the 34-year-old pregnant woman showed that this isolate had a high amino acid similarity with ZIKAV isolate MYS/P6-740/1966, an isolate reported in Malaysia in 1966 (Sapkal et al. 2017). A few months later, four cases of ZIKAV infection were reported in 2017 in the Krishnagiri district, Tamil Nadu State (Bhardwaj et al. 2017). The ZIKAV strains isolated were sequenced and have been shown to be of Asian lineages responsible for current outbreaks worldwide (Yadav et al. 2019). The most recent ZIKAV outbreak in the country was reported between September and October 2018 among 158 and 127 persons living in the Rajasthan and Madhya Pradesh States, respectively (Rolph and Mahalingam 2019, Saxena et al. 2019, Yadav et al. 2019). The authors have analyzed five ZIKAV isolates and noted the absence of mutations S139N and A188V associated with an increased neurovirulence and enhanced transmission potential in the current outbreak strains (Yadav et al. 2019).
Rift Valley fever
RVF is an acute, fever-causing disease mainly observed in domestic animals with the ability to elicit potentially severe disease in humans. The causative pathogen is a virus of the genus Phlebovirus in the Bunyaviridae family and is transmitted to humans by many mosquito species, including Aedes, Anopheles, and Culex genera (Pepin et al. 2010a). Rift Valley fever virus (RVFV) was originally identified in 1930 during an outbreak of abortions and sudden deaths among sheep in the Rift Valley of Kenya (Daubney 1932).
No human RVF infection case has been reported till now in India (Figs. 2 and 3). The virus is only encountered in small ruminants (goats and sheep) where it provokes high mortality rates and consequently enormous economic losses among farmers (Dubal and Gadekar 2013).
MERS, SARS, and COVID-19
The viruses responsible for MERS and SARS belong to the genus Betacoronavirus (CoV) in the family Coronaviridae under the Order Nidovirales. The coronaviruses encompass a large family of positive-sense ssRNA viruses, with genome length ranging between 27 and 32 kb thus making them the RNA viruses with the largest genomic material (Mackay and Arden 2015). The genomic structure of these two viruses is similar. MERS virus consists of an ssRNA encoding 10 proteins; three structural proteins (E, N, and M), two replicase polyproteins, a surface glycoprotein, and five nonstructural proteins (Mackay and Arden 2015).
The SARS-CoV genome contains five essential genes, including the open reading frames 1a and 1b (ORF1ab), S, E, M, and N genes, and coding viral protein indispensable for replication, transcription, and viral particle assembly. These essential genes are spaced by eight other genes called “accessory genes” (ORFs 3a and 3b between S and E genes, 6, 7a, 7b, 8a, and 8b between M and N genes, and 9b within the N gene) (Mackay and Arden 2015). The appearance of MERS and SARS in humans is a recent phenomenon and despite their origin being still elusive, it is thought to be originated from bats. Many studies reported the presence of these viruses in other animals such as MERS in camel (Hemida et al. 2015). SARS was first reported in 2003 during an outbreak of atypical pneumonia that occurred in Hong Kong (Lee et al. 2019).
No MERS cases have been reported in India (Figs. 2 and 3). The SARS human infections have been reported from a 32-year-old marine engineer in April 2003 in the Goa State. He sailed from Hong Kong to Mumbai before reaching Goa, where he was admitted at a health facility. Since then, no further cases have been reported in the country (Suresha et al. 2016).
A novel virus disease, COVID-19, has emerged from Wuhan, Hubei province, China, in December 2019, and has currently extended to all continents across 59 countries, including India, causing the WHO to declare this a pandemic (Jernigan and CDC COVID-19 Response Team 2020; WHO 2020a). A whole genomic study has established that this virus is a novel virus although phylogenetically closest to the SARS-like virus, and currently at least five main clades (S84, V251, I378, D392, and G614) are circulating across the world (Guan et al. 2020, Ren et al. 2020). On January 30, 2020, the first confirmed case of COVID-19 was primarily reported from the Kerala State, India (Andrews et al. 2020). She was a 20-year-old student who came back from Wuhan city on January 23, 2020. She was rapidly managed by the health authorities of Kerala and discharged a few days later (Andrews et al. 2020). Since then, many COVID-19 cases have been reported in other states and the disease is still present in the country (WHO 2020b).
Nipah and Hendra virus diseases
Nipah virus (NiV) and Hendra virus (HeV) are two virus species belonging to the genus Henipavirus in the Family Paramyxoviridae and Order Mononegavirales (Drexler et al. 2009). The first cases of NiV and HeV were initially reported in September 1998 (Ipoh, Malaysia) and September 1994 (Hendra, Australia), respectively (Sharma et al. 2018a). As in all Mononegavirales members, the genome of HeV and NiV is a nonsegmented ssRNA of 18.252 kb for HeV and 18.234 kb for NiV in length, and containing six genes encoding for six structural proteins (Lo and Rota 2008).
The first NiV outbreak was reported in 2001 in Siliguri district in the West Bengal State, India (Figs. 2 and 3). In April 2007, a second NiV outbreak involving five family members was reported by the Indian authorities at the village Belechuapara, Nadia district, West Bengal (Chadha et al. 2006, Kulkarni et al. 2013). A study showed a genomic similarity of 99.2% of these isolates responsible for this second outbreak with the Bangladesh-2004 isolate, suggesting a common source of the virus (Arankalle et al. 2011). The third outbreak occurred in May 2018 in Kozhikode and Malappuram districts in the Kerala State. The index case was in fact a cluster of four family members consisting of two brothers (26 and 28 years old), their father, and their aunt. This was the first NiV outbreak in the southern area of the country. A total of 19 cases were reported with 17 mortalities (Chadha et al. 2006, Kulkarni et al. 2013, Chatterjee 2018, Kumar et al. 2019).
Lassa fever
Lassa virus (LASV) is a highly prevalent rodent-borne virus originally isolated from a nurse in 1969 on the Jos Plateau in Nigeria (Troup et al. 1970). The virus belongs to the Old World group of the genus Mammarenavirus in the Arenaviridae family and shares morphological similarities with the lymphocytic choriomeningitis virus (Lukashevich et al. 2019). The genome of LASV consists of bisegmented (S and L) negative-sense ssRNA. The small segment (S), 3.4 kb in length, encodes for enveloped glycoprotein precursor and the viral nucleoprotein while the large segment (L), 7.4 kb in length, encodes for an RNA polymerase and a matrix Z protein (Lukashevich et al. 2019).
No LASV infection cases have been reported in India until now (Figs. 2 and 3).
Determinants and drivers for WHO-prioritized R&D blueprint EIDs reported in India
All diseases considered by the WHO-consulted experts requiring the most attention in future in terms of research and development are caused by RNA viruses. Viruses such as LASV, EboV, or MarV are classified as biosafety level four or “high containment,” with high-level human-to-human transmission and high fatality rates (Andersen et al. 2015). The nature of pathogen underlies mainly the (re) emergence of a pathogen in an area (Fig. 4). RNA viruses have high evolutionary potential due to high rates of mutations. These mutations may confer new advantageous phenotypic traits to pathogens with new opportunities to cause infections in humans.

India is a large country and because of its topographical location, it is considered a hotspot for the emergence and re-emergence of various diseases (Allen et al. 2017). Many factors can determine and drive the emergence or the re-emergence of these diseases (Fig. 4). Environmental changes due to anthropogenic activities and population growth are two likely interrelated and key drivers for these EIDs presented in this review. As a consequence of urbanization, the pressure from farmland on the environment is immense, thereby changing the environmental geographic range of potential reservoirs for viruses and increasing the contact frequency of these reservoirs with humans (Semenza et al. 2016). The chances for zoonotic transmission and emergence of new human diseases are higher accordingly. This effect of human activities was proposed as the cause of NiV outbreaks that occurred in Sumatra, Indonesia. The authors hypothesized that deforestation via forest fires was responsible for the migration of NiV-carrying fruit bats to human habitations and in fine led to the infection of slaughterhouse workers and farmers (Lo and Rota 2008, Daszak et al. 2013).
Also, the awareness of population and caregivers on EIDs is crucial to limit the appearance and propagation of these diseases. Some studies reported the low level of knowledge of health workers and caregivers on diseases such as ZIKAV and CCHFV infections in many parts of India, as shown in the present review (Fig. 2). The authors, Sharma et al. (2018b), found a low knowledge, attitude, and practice score toward ZIKAV infection among many categories of health care providers, including medical doctors and nurses, from health facilities in the Uttar Pradesh State.
This review outlines the absence of EboV human infection case outbreaks in India. The presence of vector fruit bats, R. aegyptiacus (Pteropodidae), has been reported in northwestern India (Strachinis et al. 2018), thereby delineating a real risk for transmission of EboV if favorable conditions occur in this part of the country. Besides, the high human migration due to the globalization of the world is another key determinant for the emergence of infectious diseases such as RVFV disease in India. Despite the fact that no RVFV infection human case has been reported in the country, the presence of vector mosquito species along with human migration constitutes a strong factor for the future appearance of this viral disease in India.
Finally, the experts proposed a last disease referred to as “Disease X” to outline the potential emergence of a pathogen currently unknown to cause human disease (Mehand et al. 2018). This disease X could appear in humans through the so-called phenomenon, adaptive emergence, which is the genetic change of a microorganism resulting in the acquisition of a new phenotype allowing this microorganism to invade a new ecological niche, particularly by jumping to a new host species including humans (Pepin et al. 2010b). The adaptive emergence is thought to have occurred in SARV and MERS to enhance their transmission fitness between species (Pepin et al. 2010b).
Given the high risk for (re) emergence of infectious diseases in India (Allen et al. 2017), the question is to know what can the Disease X be in the country. Strengthening the activities in the relevant areas with research capacity building would improve the response strategies in tackling these emerging diseases.
Need for efficient surveillance and response health systems
The global capacity to respond promptly to potentially epidemic-prone infectious threats depends greatly on an increased readiness, efficient surveillance, and response systems. The lack of research studies in areas of these “neglected” diseases unfortunately has not allowed effective response systems to be developed, especially in low-income countries from where most of the outbreaks and epidemics of EIDs are reported worldwide (Mehand et al. 2018). This is exemplified by the enormous difficulties that have been to jugulate the recent Ebola outbreaks in Western African countries (Murray 2015, Baseler et al. 2017). There is a lack of development of potentially efficient diagnostic, preventive, and curative tools to control epidemic-prone EIDs when reported in a country (Mackey et al. 2014). This is the case for LASV and NiV, for instance, for which no vaccine or treatment is available (Azeez-Akande 2016). Recently, efforts have been made to improve surveillance and response systems to inform outbreak management.
Management of suspicious EIDs cases is an essential part of surveillance and response systems. Several studies found hospital-acquired cases in health workers, reported during the recent CCHFV and NiV outbreaks in India (Mishra et al. 2011, Mourya et al. 2012, 2017). Also, even with hospital staff adequately trained to manage EIDs, the abovementioned diagnostic and therapeutic difficulties are still present. Generally, these control tools are developed in response to an emergency health situation. An edifying example is the rapid development of a vaccine to stop the EboV epidemic, which was responsible for the death of thousands of people in Africa.
Outbreaks and epidemic-prone disease surveillance and response system in India: the integrated disease surveillance program
Since the first NiV, SARS, and CCHFV outbreaks in the early 2000s and having had disastrous health consequences, the GOI made tremendous efforts to strengthen its epidemic-prone infectious disease surveillance and response system (NCDC 2019b). The Ministry of Health and Family Welfare, GOI, in collaboration with the World Bank implemented an integrated disease surveillance program (IDSP) under the NCDC. The IDSP was undertaken to meet the WHO guidelines for Southeast Asian countries on disease surveillance to track outbreaks. This program since 2004 aims at monitoring communicable diseases and investigating any suspected or confirmed outbreaks at the nationwide level, with reports submitted weekly (NCDC 2019b).
A large amount of data on disease are collected and analyzed to identify any potential outbreaks, identify its causes and potential transboundary threats, and deploy adapted control measures. An early alert system has been implemented to take timely preventive steps. The IDSP relies on three types of surveillance methods to collect data, namely syndromic, presumptive, and laboratory (NCDC 2019b). Data on syndromic, presumptive, and laboratory cases are filled by health workers, clinicians, and laboratory staff, respectively (NCDC 2019b). The system of collection, collation, processing, and interpretation of data is organized in a pyramidal way through three units, namely Central Surveillance Units (CSUs), State Surveillance Units (SSUs), and District Surveillance Units (DSUs) (Fig. 5).

IDSP organization structure. IDSP, integrated disease surveillance program [data were extracted from
The DSUs are at the bottom of the pyramid and are based in all districts of the country where they collect data, thereafter transfer these data to SSUs based at each state and union territories (UTs), and finally, the data are sent to a CSU grounded in the Delhi UT (NCDC 2019b). The CSU receives disease outbreak reports from each SSU, which are compiled in the form of a weekly outbreak report (Monday-Sunday) and then made available on the website of the NCDC. An average of 40–50 outbreaks are reported to the CSU on a weekly basis (NCDC 2019d).Whenever there is a rising trend in any given area, it is investigated by Rapid Response Teams (RRT) to diagnose and contain the outbreak.
Investigation of outbreaks
The methodology for the identification of an outbreak varies from one institution to another (i.e., government agency, private institution, academic institution) and thus there is no uniform investigation approach used by the abovementioned stakeholders. However, the following 10 steps are invariably used by the different agencies: (1) prepare for field work, (2) establish the existence of an outbreak, (3) verify the diagnosis, (4) define and identify cases, (5) perform a descriptive epidemiology study, (6) develop hypotheses, (7) evaluate/perform additional studies as necessary, (8) implement control and prevention measures, (9) communicate findings, and (10) follow-up recommendations (for more details:
Achievements of NCDC-IDSP
The NCDC has been provided with new technologies for the diagnosis of diseases, many of which are indigenously developed (Mourya et al. 2019). The divisions have well-equipped laboratories with modern equipment capable of undertaking tests using latest technology. Also, NCDC developed many tools such as “CDAlert,” a newsletter used to easily disseminate the information on outbreaks at different levels, including Directorates of Health Services of different states, districts, primary health centers, medical colleges, and ultimately, individuals (NCDC 2019a). In addition, IDSP published online a number of guidelines on the epidemic-prone diseases that have recently burdened the country (NCDC 2019c). Besides, the NCDC also addresses vector control questions under its division called the Centre for Medical Entomology and Vector Management. Other achievements made by IDSP included the following: completion of trainers' training in all states/UTs, the establishment of a media scanning and verification cell that analyzes all media alerts about disease cases and a call center that receives disease alerts and transfers them to each SSU/DSU for further investigation, and an extension of the referral laboratory network across the country (NCDC 2019c).
Success stories
India has been facing several outbreaks of the EIDs addressed in the present review and a large number of fights have been remarkably won. Two success examples with NiV and ZIKAV are particularly interesting.
In 2018, an outbreak of NiV occurred in two districts of Kerala as previously mentioned (Baggchi 2018, Sahay et al. 2020b). The first case was recorded at the Baby Memorial Hospital in Kozhikode district and medical doctors suspected a rare virus infection and thereafter sent the sample to referral centers (Manipal Centre for Virus Research in Karnataka and then NIV in Pune, Maharashtra), which confirmed the infection with NiV (Baggchi 2018, Sahay et al. 2020b). Very rapidly, the Government of Kerala with the assistance of the GOI, other national agencies, and the WHO coordinated their actions through a set of measures, including among others tracking and isolation of contact cases, large-scale surveillance, and mass awareness campaign (Baggchi 2018, Sahay et al. 2020b). This “No Nipah” campaign has been particularly efficient through using simple messages (e.g., put a lid on date palm sap collection container) on how populations could prevent NiV infection. After June 1, 2018, no NiV cases were reported in Kerala.
The same year on September 21, 2018, an outbreak of ZIKAV started in the Jaipur district of Rajasthan State. The authorities rapidly responded by implementing a containment strategy consisting of laboratory testing, sequencing of the ZIKAV, active human and vector surveillance, vector management, multisectoral collaboration and coordination, social mobilization, and risk communication all in a predefined geographic area around the epicenter (Singh et al. 2019). No more than 1 month later the outbreak had been contained in the infected areas.
Gaps identified and solutions proposed to improve some key components of response system
Details are shown in Table 1.
Gaps and Solutions Proposed to Improve Some Components of the Response System
EID, emerging infectious disease; IDSP, integrated disease surveillance program; NIE, National Institute of Epidemiology; NIV, National Institute of Virology; UTs, union territories; WHO, World Health Organization.
Strengths of India to achieve the WHO roadmap
India can play a more preponderant role in the WHO roadmap for the control and elimination of EIDs. Some of the following strengths can support this statement: India has been facing a large number of EID outbreaks and alerts all over the territory each year and its response time is generally efficient and prompt. Other countries can benefit from the Indian experience to tackle the outbreaks as promptly and efficiently as India. The country has a great adaptation capacity to face EIDs as seen in the development of new technologies such as indigenous diagnostic tests to fight against previous and future NiV or CCFV outbreaks (Shrivastava et al. 2019). India is taking a large place in innovative researches and has emerged as a new hub for the vaccine and drug industry in the last decade. In this regard, India can play a major role in the eradication of EIDs through the development of new vaccines/drugs.
Conclusions
This review presents the current scenario of zoonotic diseases, considered by the WHO as the future threat, in India. To date, CCHFV, SARS, ZIKAV, and NiV diseases are reported responsible for outbreaks in humans in eight states of the country, while COVID-19 is currently reported from most of the states. There are no reports for human infection of EboV, MarV, RVF, and LASV in the country. Anthropogenic activities and the lack of effective control strategies were some of the drivers responsible for the emergence and spread of these viruses in the different Indian states. To this fact, the GOI has deeply strengthened its surveillance and response system of outbreaks and epidemic-prone diseases through the implementation of the IDSP. Despite profound improvements made in the anticipation of threats, there are still enormous efforts in strengthening manpower capacities, sensitization of populations, as well as hospital management of the EIDs addressed in the review.
Footnotes
Acknowledgment
The authors are grateful to Mr. Stephane Koum (Department of Earth Sciences, University of Douala, Cameroon) for generating maps using ArcGIS version 10.5.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this article.