
Abstract
Babesiosis is a tick-borne disease that is caused by intraerythrocytic protozoan parasites of the genus Babesia. Common symptoms of babesiosis are generally characterized as nonspecific flu-like symptoms, such as fever or chills. Human infections are reported to the Centers for Disease Control and Prevention (CDC) through the National Notifiable Diseases Surveillance System (NNDSS). This study summarizes data of Babesia infections reported to the CDC by the NNDSS from 2011 to 2018. In total, there were 14,159 reported cases of babesiosis, and the incidence rate was 5.55 cases per million persons per year, displaying an increasing trend during the study period. The demographic group most affected was middle-aged and elderly white males. Infections were most abundant in the New England and the Mid-Atlantic regions of the United States. Our study provides useful results for a basic understanding of incidence, spatial and temporal distribution, and severity of babesiosis.
Introduction
Babesiosis is caused by intraerythrocytic protozoan parasites of the genus Babesia (Vannier and Krause 2012). Babesiosis is typically transmitted through a tick vector (Vannier and Krause 2012). More recently, cases of babesiosis have resulted from blood transfusions (Gubernot et al. 2009), organ transplantation (Ather et al. 2017), and probably also congenitally from mother to child (Sethi et al. 2009).
Presentation of symptoms are similar to nonspecific flu-like symptoms, such as fever or chills, and therefore diagnosis can be missed or delayed (Vannier et al. 2015). While most patients make a complete recovery following treatment, which consists of atovaquone and azithromycin (Krause et al. 2000) with clindamycin and quinine as an alternative (Krause 2019) in the United States, the disease may be severe or fatal for those in high-risk categories (Vannier et al. 2015). Risk factors associated with acquisition or severe babesiosis include asplenia, cancer, HIV infection, hemoglobinopathy, chronic heart, lung, of liver disease, individuals >50 years, or those on immunosuppressive medications (Vannier and Krause 2012).
In this study, we summarize the passive surveillance data of Babesia infections reported to the Centers for Disease Control and Prevention (CDC) from 2011 to 2018. Our goal is to increase awareness of recent babesiosis trends and to analyze these patterns, following the methods used by Baker et al. (2020) and Mogg et al. (2020). Before 2011, babesiosis was not recognized as a nationally notifiable disease, therefore comprehensive national data do not exist for babesiosis before 2011 (Gray and Herwaldt 2019). We also characterize the epidemiology of reported cases, including demographic profiles, incidence rates (IRs), and the spatial/temporal patterns of infections.
Materials and Methods
National Surveillance Systems
Individual states and territory health departments use the National Notifiable Diseases Surveillance System (NNDSS) to report surveillance data to the CDC using manually completed Babesiosis Case Report Forms (
Case definition
Of babesiosis cases reported to the CDC, the infections can be classified as either confirmed or probable (Herwaldt et al. 2012). To be considered confirmed, a case must have both confirmatory laboratory results and meet at least one of the objective or subjective clinical evidence criteria, regardless of mode of transmission. Objective clinical criteria include fever, anemia, or thrombocytopenia, and subjective clinical criteria include chills, sweats, headache, myalgia, or arthralgia. Confirmatory laboratory evidence can include identification of Babesia organisms by microscopic examination of one or several blood smears from the patient, or detection of Babesia DNA through polymerase chain reaction or nucleic acid amplification.
There are two ways for a case to be considered probable: either a case that has supportive laboratory results and meets at least one of the objective clinical evidence criteria (subjective criteria alone are not sufficient), or a case that is in a blood donor or recipient epidemiologically linked to a confirmed or probable babesiosis case and has some form of laboratory evidence (whether it be confirmatory or supportive). Supportive laboratory criteria include a variety of antibody detecting assays, including Western blotting techniques.
Analysis
Babesiosis became a nationally notifiable disease in 2011, so prior data do not exist at the national level; note also that in 2011 cases were not classified as either probable or confirmed, but instead were reported as a single figure. Data before 2011 exist only in regions of high incidence in the northeast and Midwest, in states such as New York (Meldrum et al. 1992, Joseph et al. 2020) and Wisconsin (Stein et al. 2017). Gray and Herwaldt (2019) recently reported the trend in the national data covering the period from 2011 to 2015. The present study updates this trend based on data from January 2011 through December 2018.
The IRs were calculated by year, state, and age, using the U.S. Census Bureau population estimates. This study does not include confidence intervals or results from statistical hypothesis testing since reported cases cannot be generalized to unreported cases or to other reporting time periods (Dahlgren et al. 2011, Heitman et al. 2016).
Results and Discussion
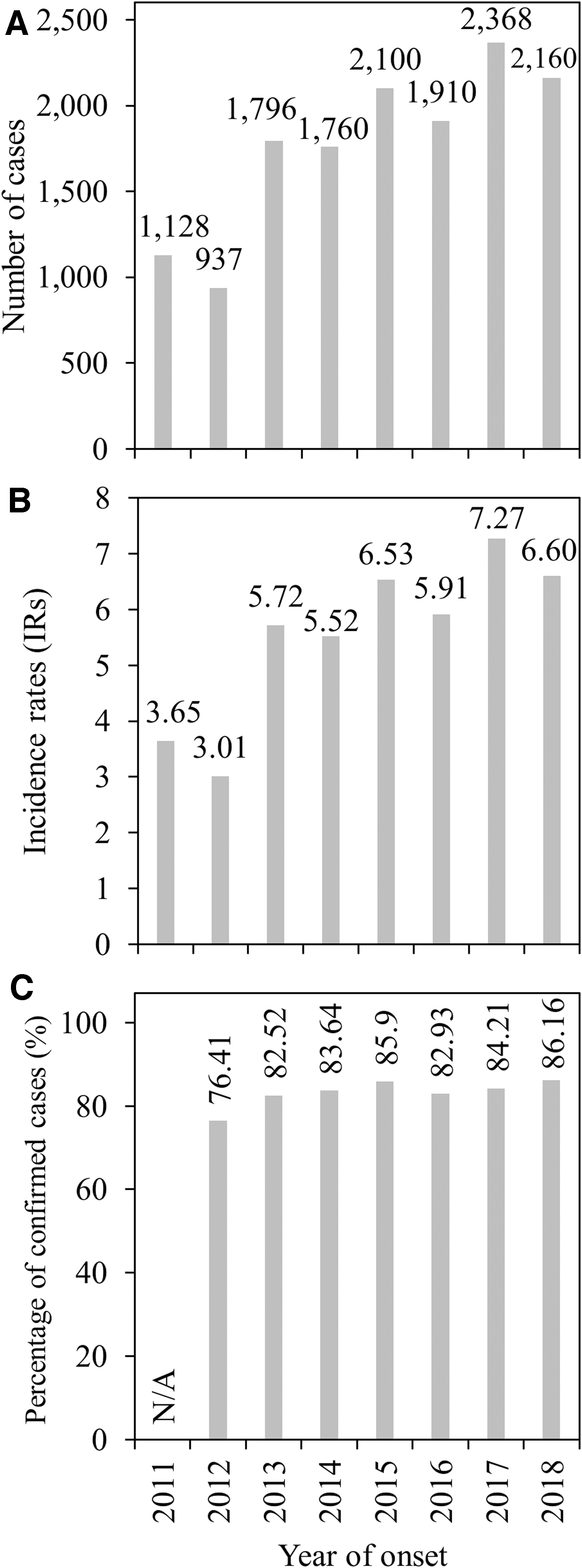
From 2011 to 2018, there were 14,159 cases of babesiosis reported to the CDC, with the number of new cases reported approximately doubling during this period (Fig. 1A). The IRs followed a similar trend, increasing from ≈3 in 2011 and 2012 to ≈7 in 2017 and 2018, with a mean of 5.55 for this period (Fig. 1B). The annual percentage of confirmed cases remained at ≈80, although it was slightly lower in 2012 (and was not reported in 2011) (Fig. 1C).
Number of cases of babesiosis
Demographic profiles of the infection cases indicated there was higher incidence among (1) males (64.62%, IRs = 3.59) than females (34.29%, IRs = 1.90), (2) whites (62.23%, IRs = 3.29) than any other race, (3) non-Hispanics (51.14%, IRs = 2.84) than any other ethnicity, and (4) the age group 65+ years (44.62%, IRs = 2.48) than any other age group (Table 1) (note there was high incidence among those reported as unknown race [33.33%, IRs = 1.85] and those reported as unknown ethnicity [43.26%, IRs = 2.40]). Thus, babesiosis primarily afflicted elderly white males, similar to other tick-borne disease such as anaplasmosis and ehrlichiosis (Adams et al. 2017, Mogg et al. 2020).
Demographic Profiles of Babesiosis Cases from 2011 to 2018 in the United States
The number of incidence cases is from the Nationally Notifiable Diseases Surveillance System, and the cases per million persons (IRs) at risk are calculated based on data from the Nationally Notifiable Diseases Surveillance System and the U.S. Census Bureau.
IR, incidence rate.
Patterns revealed by these profiles likely reflect behavioral and physiological differences among demographic groups. Higher levels of outdoor activity place individuals at higher risk for encountering ticks and contracting a tick-borne disease (Kilpatrick and Randolph 2012). White males may be more likely to spend time outside in areas where ticks are abundant (Gupta et al. 2018). Aging immune systems make elderly individuals more likely to develop severe infection leading to hospitalization than younger individuals (18- to 40-year-olds) with stronger immune systems (Vannier et al. 2004, Nikolich-Žugich 2018). Of course, these results also reflect an inherent reporting bias due to the unequal access to health care among demographic groups (Jones et al. 2012).
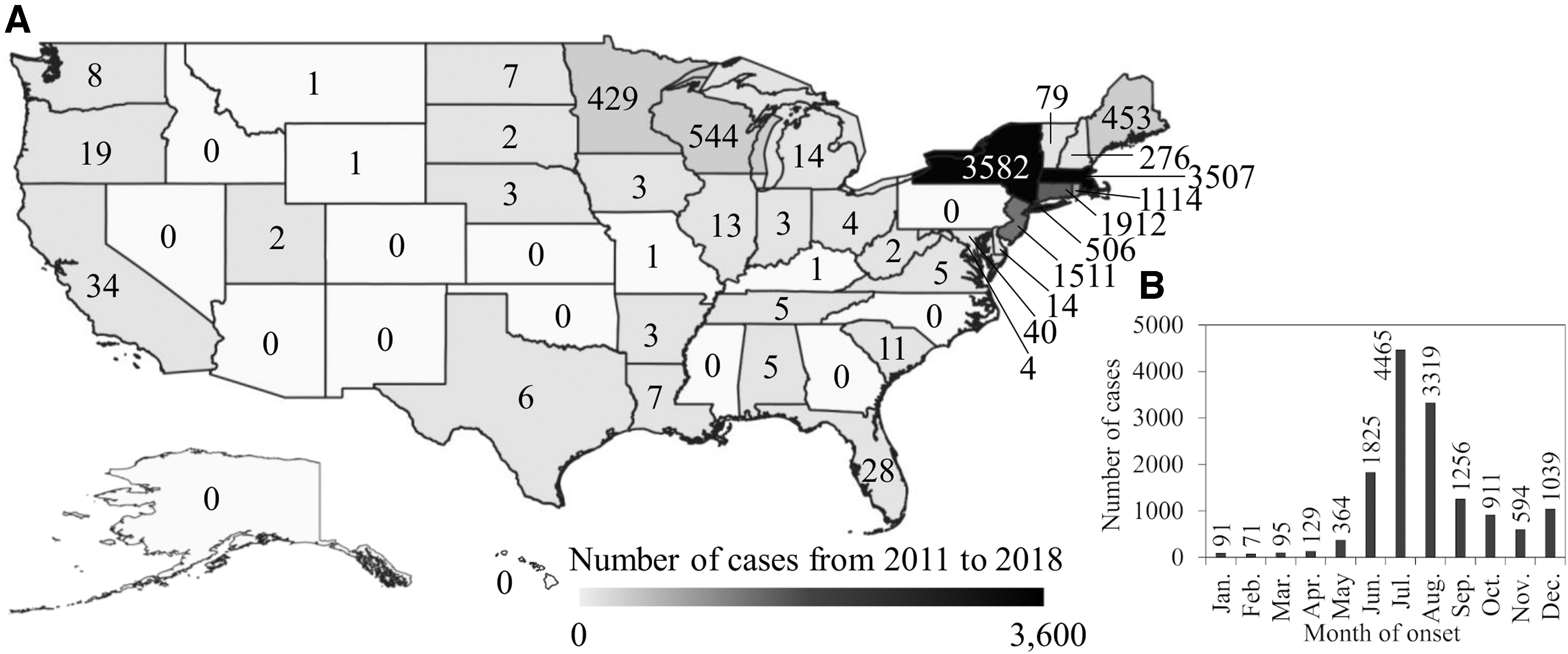
The geographic distribution of babesiosis reported from 2011 to 2018 was concentrated in New England and the Mid-Atlantic regions (Fig. 2A). The state of New York had 3582 cases (25.30% of the total), followed by Massachusetts (3507, 24.77%), Connecticut (1912, 13.50%), New Jersey (1511, 10.67%), Rhode Island (1114, 7.87%), Wisconsin (544, 3.84%), New York City (506, 3.57%), Maine (453, 3.20%), and Minnesota (429, 3.03%). Areas where babesiosis incidence was highest, such as New York and Massachusetts, are areas in which Babesia microti is endemic (Joseph et al. 2011).
Spatial
Babesia microti is a blood-borne apicomplexan parasite transmitted by blacklegged ticks (Ixodes scapularis) among animal reservoirs such as white-footed mice (Peromyscus leucopus), raccoons (Procyon lotor), short-tailed shrews (Blarina brevicauda), and eastern chipmunks (Tamias striatus), and is a primary cause of babesiosis in humans in the United States (Hersh et al. 2012).
The seasonal distribution of onset of babesiosis was concentrated during the summer from June through August, with approximately two-thirds of the cases reported during this period (Fig. 2B). Reported cases declined during fall and early winter (September through December) and were relatively rare during mid-winter and spring (January through April), with cases beginning to rise again in May. Adult tick activity peaks during the warmest months (June through August in the northern United States) when vertebrate hosts also are active, and gradually declines over the next few months (Wang et al. 2012). Thus, the seasonal distribution of babesiosis largely reflects the coincidence of months of high host-seeking activity by ticks with months of relatively high outdoor activity levels of humans (Wang et al. 2015, 2016).
Our data are limited to passive data surveillance, so we are unable to detect discrepancies in the identification of tick-borne diseases. Therefore, increased diagnostic testing is needed to improve data on both babesiosis and other similar tick-related diseases. Furthermore, converting the Nationally Notifiable Disease Surveillance System from a mail-in system to an electronic system would improve data (Gray and Herwaldt 2019).
Unfortunately, symptoms characteristic of babesiosis are common to many illnesses, and it is unlikely that a physician would test for the disease during early stages of infection unless a tick-borne infection was already suspected. Thus, ongoing surveillance and reporting of babesiosis remain essential to inform public health practice and guide disease treatment and prevention efforts (Leiby 2011). Nonetheless, our results provide a useful indicator of the general incidence, distribution, and severity of babesiosis.
Conclusion
Our results update an earlier report (Gray and Herwaldt 2019) and confirm the rising incidence of human babesiosis in the United States during the past decade. The blacklegged tick, I. scapularis, continues to act as a vector for babesiosis, as well as other well-known diseases such as Lyme disease and anaplasmosis (Eisen and Eisen 2018). These diseases, without proper detection and treatment, can impose a severe health burden. To reduce the severity of these tick-borne diseases, increased early on identification is required (Baker et al. 2020, Mogg et al. 2020).
To combat the increasing incidence of babesiosis, the implementation of prophylactic measures, such as reducing risk of transmission by daily body checks for ticks, minimizing skin exposure to ticks, and use of tick repellents, is needed (Sanchez et al. 2016). This means increasing the percentage of confirmed diagnoses compared with probable, and testing for these diseases from an early onset of symptoms. Once again, this also poses an issue as symptoms characteristic of babesiosis are common to many illnesses. Furthermore, ongoing reporting and surveillance of babesiosis remain essential (Leiby 2011).
Footnotes
Acknowledgment
The authors would like to thank the anonymous reviewers for the time and effort they devoted to helping us improve the article.
Author Disclosure Statement
No conflicting financial interests exist.
Funding Information
No funding was received for this study.